ww w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Methylene
tetrahydrofolate
reductase,
transforming
growth
factor-

1
and
lymphotoxin-
␣
genes
polymorphisms
and
susceptibility
to
rheumatoid
arthritis
Olfat
G.
Shaker
a,
Amina
M.
Alnoury
b,c,
Gehan
A.
Hegazy
b,d,
Hemmat
E.
El
Haddad
e,
Safaa
Sayed
f,
Ahmed
Hamdy
e,∗aMedicalBiochemistryandMolecularBiologyDepartment,FacultyofMedicine,CairoUniversity,Cairo,Egypt bClinicalBiochemistryDepartment,FacultyofMedicine,KingAbdulazizUniversity,Jeddah,SaudiArabia cMedicalBiochemistryDepartment,FacultyofMedicine,AinShamsUniversity,Cairo,Egypt
dMedicalBiochemistryDepartment,NationalResearchCenter,Cairo,Egypt eInternalMedicineDepartment,FacultyofMedicine,CairoUniversity,Cairo,Egypt
fRheumatology&RehabilitationDepartment,FacultyofMedicine,CairoUniversity,Cairo,Egypt
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received17October2015 Accepted16March2016 Availableonline25May2016
Keywords:
Rheumatoidarthritis Genepolymorphism MTHFRC677TandA1298C TGF-1T869C
LT-␣A252G
a
b
s
t
r
a
c
t
Background:Rheumatoidarthritisisawidelyprevalentautoimmunedisorderwithsuggested geneticpredisposition.
Objectives:Theaimofthisstudyistodetectthepatternofgeneticpolymorphismof methy-lenetetrahydrofolatereductase(MTHFRC677TandA1298C),transforminggrowthfactor-1 (TGF-1T869C)andlymphotoxin-␣(LT-␣A252G)inpatientshavingrheumatoidarthritisand correlatethesepatternstodiseaseactivityandserumlevelsoftumornecrosisfactor-alpha (TNF-␣),B-CellActivatingFactor(BAFF),andosteopontin.
Methods:Atotalof194subjects,90controlsand104patientswithrheumatoidarthritiswere genotypedforMTHFRC677TandA1298C,TGF-1T869CandLT-␣A252Gpolymorphisms usingamethodologybasedonPCR-RFLP.AlsoserumlevelsofTNF-␣,osteopontinandBAFF weremeasuredbyELISAkits.
Results:TheCTgenotypeandTalleleofMTHFRC677TandGGgenotypeandGalleleofLT-␣
A252GareassociatedwiththeriskofRAandwithhigherlevelsofthepro-inflammatory cytokine,TNF-␣inpatientswithrheumatoidarthritis.
Conclusion:OurfindingssuggestthatthereisassociationbetweenMTHFRC677TandLT-␣
A252GgenespolymorphismsandincreasedriskofRAinthissampleofEgyptianpopulation. ©2016PublishedbyElsevierEditoraLtda.ThisisanopenaccessarticleundertheCC BY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mail:[email protected](A.Hamdy). http://dx.doi.org/10.1016/j.rbre.2016.04.002
Polimorfismos
dos
genes
metilenotetrahidrofolato
redutase,
fator
de
crescimento
transformador

1
e
linfotoxina-
␣
e
susceptibilidade
à
artrite
reumatoide
Palavras-chave:
Artritereumatoide Polimorfismogenético MTHFRC677TeA1298C TGF-1T869C
LT-␣A252G
r
e
s
u
m
o
Antecedentes: Aartritereumatoideéumadoenc¸aautoimuneamplamenteprevalentecom sugeridapredisposic¸ãogenética.
Objetivos: Detectaropadrãode polimorfismodosgenesmetilenotetrahidrofolato redu-tase(MTHFRC677TeA1298C),fatordecrescimentotransformador1(TGF-1T869C) elinfotoxina-␣(LT-␣A252G)empacientescomartritereumatoideecorrelacionaresses padrõescomaatividadedadoenc¸aeosníveisséricosdefatordenecrosetumoralalfa (TNF-␣),fatorativadordelinfócitosB(BAFF)eosteopontina.
Métodos: Foramgenotipados194indivíduos–90controlese104comartritereumatoide–à procuradepolimorfismosdosgenesMTHFRC677TeA1298C,TGF-1T869CeLT-␣A252G comumametodologiabaseadanaPCR-RFLP.Mensuraram-setambémosníveisséricosde TNF-␣,osteopontinaeBAFFcomkitsdeElisa.
Resultados: OgenótipoCTeoaleloTdoMTHFRC677TeogenótipoGGealeloGdoLT-␣
A252GestãoassociadosaoriscodeAReaníveismaiselevadosdacitocinapró-inflamatória TNF-␣empacientescomartritereumatoide.
Conclusão: Osachadosdopresenteestudosugeremqueháassociac¸ãoentreos polimorfis-mosdosgenesMTHFRC677TeLT-␣A252GeumriscoaumentadodeARnessaamostrada populac¸ãoegípcia.
©2016PublicadoporElsevierEditoraLtda.Este ´eumartigoOpenAccesssobuma licenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Rheumatoidarthritis(RA)isawidelyprevalentautoimmune disorderwhichaffects∼1%ofthepopulationsindeveloped countries withwomen morefrequently affected than men (∼3:1).1Inthisdisease,thejointsarethemaintargetofattack withgreat tendency tojoint destruction and consequently impairmentofallaspectsoflifequality.2 Theexact causes ofthediseaseareunknown,butenvironmentalfactorsand geneticpredispositionareinvolved.Althoughthesefactorsare notsufficientfordevelopmentofdisease,yettheymayhavea roleintheheterogeneityoftheclinicalpicture,theresponse totreatmentand theycanbetargetfortherapeuticagents. Polymorphicformsofmethylenetetrahydrofolatereductase (MTHFR)geneandsomecytokinegeneshavebeenstudiedas possiblemarkersofsusceptibility,severity,and/orprotection inRA.3
C677 T (Ala 222 Val) and A1298 C (Glu 429 Ala) are two common genetic polymorphisms of MTHFR gene. They are both associated with decrease in the activity of the enzyme 5, 10-methylenetetrahydrofolate reductase (MTHFR)withlower degreeinA1298CcomparedtoC677T polymorphism.4 Thisenzymeisresponsibleforthe synthe-sisof5-methyltetrahydrofolate,requiredforpyrimidineand purinesynthesisandregenerationofmethioninefrom homo-cysteine.5 Decreasedactivity ofthisenzymeresultsinhigh levelsofhomocysteinewhichiscommonlyfoundinpatients withrheumatoid arthritis(RA), and is partiallyresponsible for the high rate of cardiovascular complications in these subjects.6
Transforminggrowthfactor-1(TGF-1) isagrowth fac-torthatregulatescellularproliferation,woundhealing,and
angiogenesis inacell-specificmanner.7 Itispresent abun-dantly in rheumatoid joints and it has anti-inflammatory functionbecauseoverexpressionofthisgenereducedarthritis inananimalmodel.8IndividualswithTGF-1polymorphisms inthecodingandregulatoryregionshaveagreaterpropensity todevelopimmunesystemdisorders.TGF-1(T869C) poly-morphismaffectstheserumlevelsofTGF-1andisusedas markerforincreaseddiseaseriskinseveraldiseases.9
CytokinesplayanimportantroleinpathogenesisofRAand itsassociatedinflammatoryprocessesandarticular destruc-tion.Thisoccursmainlythroughdeviationofbalancetoward higherlevelsofpro-inflammatorycytokinesontheexpense ofanti-inflammatory cytokines. Thus,the concentrationof membersofpro-inflammatoryTNF-␣superfamilyhavebeen directlycorrelatedwithdiseasepathology.10TNF-␣isapotent pro-inflammatorycytokineproducedmainlybymacrophages. Itisconsideredoneofthemaininflammatorymediatorsof jointinflammationanddestructioninRAbyinducingother inflammatorycytokinesandstimulatingexpressionof adhe-sionmoleculesbyfibroblasts.11Lymphotoxin-␣(LT-␣),another memberoftheTNFsuperfamilypreviouslyknownastumor necrosisfactor-(TNF-)inducescellapoptosisand inflam-matoryresponsesuponbindingtoTNFreceptortype1and2 respectively.12Asinglenucleotidepolymorphism(A252G)was detectedwithinthefirstintronofLT-␣geneanditwasreported toincreaseexpressionofLT-␣plasmalevel.13Thetwoalleles resultingfromthissinglenucleotidepolymorphismare desig-natedLT-␣(10.5kb)andLT-␣(5.5kb).TheLT-␣(5.5kb)alleleis associatedwithhigherplasmalevelsofLT-␣,lymphoid malig-nanciesandaworseoutcomeofautoimmunediseases.14
regulationofbothinnateand adaptive immuneresponses. Deregulation of BAFF has been observed in patients with autoimmunediseasessuchasrheumatoidarthritis.15 Osteo-pontin(OPN)isalsoapro-inflammatorycytokinewhichhas immunoregulatoryeffectsinautoimmunediseasesandcould beinvolvedinthepathogenesisofRA.16
Theaimofthis studyistodetect thepatternofgenetic polymorphismofMTHFRtypes(C677T)and(A1298C),
TGF-1(T869C)andLT-␣(A252G)inrheumatoidarthritisEgyptian patientsandifthereisanycorrelationofthosepatternswith diseaseactivity andserumlevelsofTNF-␣,BAFFand osteo-pontin.
Subjects
e
methods
Subjectsselection
Thisisacrosssectionalobservationalcomparativestudythat was conductedin Kasr Al Aini rheumatology unit, Faculty ofMedicine,Cairo University from May to December 2013. Thestudywasconductedaccordingtotheprinciplesofthe Helsinki Declaration and was approvedby the localethics committeeoftheFacultyofMedicineofCairoUniversity.
Informed written consent was obtained from all sub-jectswhoparticipatedinthisstudyafterexplainingtheaim and nature of the study. One hundred and four patients with rheumatoid arthritis (16 males and 88 females) and ninetyhealthycontrolsubjectsofmatchedageandsexwere includedinthestudy.Thepatientswereonregulartreatment withnon-steroidalanti-inflammatorydrugs(NSAID)(n=42), methotrexate(n=88),Prednisone(n=24),Leflunomide(n=32) andHydroxychloroquine(n=56).Patientsweretreatedby dif-ferentcombinationsofthepreviousdrugs.Thoroughhistory takingandphysicalexaminationweredone forallpatients andDisease activityscorein28 joints(DAS-28) andHealth AssessmentQuestionnairetotal(HAQ)totalwerecalculated.
Laboratoryassays
SerumBAFF,OPN and TNF-␣ were measured byELISA kits obtainedfromR&DSystems,Minneapolis,MN,fortheformer twoandfromAviBion,HelsinkiFinlandforTNF-␣according tothemanufacturer’sprotocol.
Molecularanalysis
DNAextraction
GenomicDNAwasextractedfromperipheralbloodusingaQIA ampDNABloodMiniKit(Qiagen,Valencia,CA,USA)according tothemanufacturer’sprotocol.Genotypingwasperformedby polymerasechainreaction-restrictionfragmentlength poly-morphism(PCR-RFLP).
GenotypingofMTHFRA1298C17
Onesetofforward“5′-CTTTGGGGAGCTGAAGGACTACTA C-3′′andreverse“5′-CACTTTGTGACCATTCCGGTTTG-3′′ primerswereusedforamplificationofafragmentof241base pairsandthentheamplifiedfragmentwasdigestedwithMboII enzyme.ThePCRprofilewas:initialdenaturationat95◦Cfor
5min,followedby35cycles eachof30sat94◦C,51◦C and 72◦C,then for 10minat 72◦C.The AAgenotype produces twobandsof211and30bp,theCCgenotypeproducesa sin-glebandof241bp(uncut),andACgenotypesproducesthree bandsof241,211and30bp.
GenotypingofMTHFRC677T18
Onesetofforward“5′-CATCCCTATTGGCAGGTTAC-3′′and reverse“5′-GACGGTGCGGTGAGAGTG-3′′primerswereused foramplificationofafragmentof198basepairs,andthenthe amplifiedfragmentswere digestedwithHinfI enzyme.The PCR profilewas: initialdenaturationat94◦C for5min, fol-lowedby35cyclesof30seachat94◦C,61◦Cand72◦Canda finalelongationat72◦Cfor5min.ThewildCCgenotypewas identifiedbyonlya198bpfragment,the(TT)genotypebythe 175/23bpfragmentsandheterozygotes(CT)genotypebyboth the198,175and23bpfragments.
GenotypingofTGF-ˇ1T869Cgenotypes19
One set offorward primers 5′-TTCCCTCGAGGCCCTCCTA-3′ and reverse 5′-GCCGCAGCTTGGACAGGATC-3′ primers were usedforamplificationof294bpfragmentsoftheTGF-1gene. PCR products were then digested byMspA1I enzyme.The PCR profilewas: denaturation at96◦C for 10min, followed by35cyclesof75seachat96◦C,62◦Cand72◦C,andafinal extensionat72◦Cforfiveminutes.TheTalleleresultedin 4fragmentsof161,67,40,and26bp.TheCalleleresultedin fragmentsof149,67,40,26,and12bp.
GenotypingofLT-˛(A252G)20
A 782bp fragment of the intron 1 (+252A/G) of the LT-␣ gene was PCR-amplified with the primer set: (for-ward) “5′-AGAGGGGTGGATGCTTGGGTTC-3′′ and (reverse) “5′-CCGTGCTTCGTGCTTTGGACTA-3′′. PCR products were digestedwithNcoIrestrictionenzyme.TheAallelegivesa sin-glefragmentof782-bp(notdigested).TheGalleleisdigested into586-bpand196-bpbands.ThePCRprofilewas:incubation for5minat95◦C,followedby35cyclesof1minat95◦C,1min at52◦C,and1minat72◦C,withafinalextensionof72◦Cfor 7min.
Statisticalanalysis
StatisticalPackageofSocialScienceSoftwareprogram(SPSS), version 19 was used to analyze data. Data were summa-rized using frequency and percentage for qualitative data or meanandstandarddeviationforquantitativeones. Chi-squaredanalysiswasusedtotestfordeviationofgenotype distribution from Hardy-Weinberg. Comparison of patients andhealthycontrolgroupswereperformedusingChisquare testorFisher’sexact testforqualitativedataand Studentt
Table1–Patients’characteristics.
Parameters Min Max Mean±SD
Age(years) 22.0 70.0 42.7±12.1 Diseaseduration(month) 6 216 66.7±52.5 Morningstiffness(min) 3.0 120.0 29.9±38.2 Numberofswollenjoints 0.0 18.0 3.3±5.5 Numberoftenderjoints 0.0 20.0 5.0±5.9
ESR 5.0 125.0 36.4±36.0
DAS28 1.4 7.7 3.9±1.6
Results
Patients’characteristicsincludingage,diseaseduration, clin-icalmanifestations, disease activity and ESR are shown in Table1.
ComparisonbetweenserumlevelofOsteopontin,BAFFand TNF-␣(expressedasmean±SD)inpatientsandcontrolgroups showedthatserumlevelsofOPNandTNF-␣weresignificantly higherincasescomparedtocontrols(p<0.001).SerumBAFF levelshowednostatisticaldifferencebetweenpatientsand controlgroups(p=0.6)(Table2).
OncomparingtheabilityofTNFandOsteopontinin dis-criminatingcontrol from rheumatoid arthritis patients the ROCcurve showed thatTNF-␣ has ahigherdiscriminating abilitythanOPNwithsensitivity(94.2%)andspecificity(84.4%) atcutoffvalue15.2pg/ml.Ontheotherhand,OPNhas sensi-tivity(71.2%)andspecificity(53.3%)atcutoffvalue5.7ng/ml ascalculatedbyROCcurve(Figure1).
Theresultsofthisstudyshowedthatthegenotype frequen-ciesofallstudiedcaseswereinHardy-Weinbergequilibrium forMTHFRC677T&A1298CandTGF-1T869C.Asfor
LT-␣A252G,thegenotypefrequencieswereinHardy-Weinberg equilibriumonlyincontrolgroup.
Onstudyingtheassociationbetweenrheumatoid arthri-tisanddifferentpolymorphicformsofMTHFRC677T,MTHFR A1298C,TGF-1T869CandLT-␣A252G(Table3).Theresults ofthisstudyshowedsignificantassociationbetween rheuma-toidarthritisandCTgenotype,TalleleofMTHRFC677Tand the GGgenotype and Gallele ofLT-␣ A252G. On the other hand,theACgenotypeofMTHFRA1298Cshowedaprotective effectfromthediseasewhencomparedtothewildgenotype AA.Moreover,no significantassociation hasbeen detected betweendifferentpolymorphicformsofTGF-1T869C poly-morphismandrheumatoidarthritis(Table3).
HAQtotalshowednoassociationwithdifferent polymor-phicformsofMTHFRC677Tpolymorphism(2=5.5,p=0.06), MTHFRA1298C(2=2.26,p=0.32),TGF-1T869C,(2=1.31,
p=0.52) or LT-␣ (2=1.1, p=0.57). Also, disease activity as
1.0
0.8
0.6
Sensitivity 0.4
0.2
0.0
0.0 0.2 0.4 ROC curve
Osteopontin TNF Reference line 0.6
1 - specificity
0.8 1.0
Figure1–ROCcurveshowingabilityofTNFand osteopontinindiscriminatingcontrolfromrheumatoid arthritispatients.
shownbyDAS28wasnotassociatedwithpolymorphicforms ofallexaminedgenes;forMTHFRC677T(2=0.4,p=0.81),for MTHFRA1298C(2=0.69.p=0.7),forTGF-1T869C(2=4.27,
p=0.12)andforLT-␣(2=4.54,p=0.1).
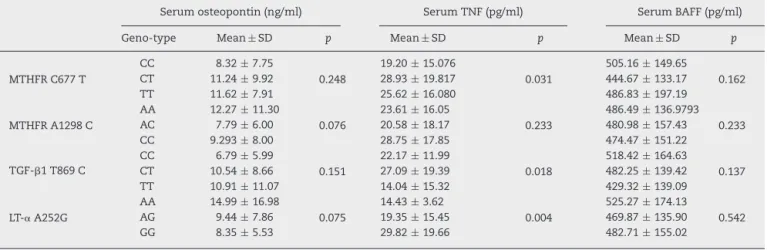
Wefoundthatserum TNF-␣leveldifferssignificantlyin the different polymorphicformsofall tested genesexcept MTHFRA1298CasshowninTable4.PostHoctestshowed thatserumTNF-␣issignificantlyhigherinCTgenotypethan inCC genotypeinMTHFRC677 T,p=0.009, inCT genotype thanthatinTTgenotypeinTGF-1T869C,p=0.005,inGG genotypewhencomparedtothatinAAgenotype,p=0.008, andAGgenotype,p=0.005,inLT-␣A252G.Thereisno signifi-cantdifferenceinOPNandBAFFserumlevelsinthedifferent genotypesofexaminedgenes(Table4).
Discussion
Although the etiology of RA remains unclear, susceptibil-ity factors that includeenvironmental and genetic factors are evident. The genetic factors constitute about 50% of thesefactors.3Thepro-inflammatorycytokinesamplifythe inflammatoryprocessanddestructioninrheumatoidjoints. Tumornecrosisfactor,osteopontinandBAFFareamongthese cytokines.3
Table2–Comparisonbetweenserumlevelofosteopontin,BAFFandTNF-␣(expressedasmean±standarddeviation)in patientsandcontrolgroups.
Cases(n=104) Mean±SD
Controls(n=90) Mean±SD
pvalue
Osteopontin(ng/ml) 12.9±10.6 5.9±2.5 <0.001
BAFF(pg/ml) 474.5±151.1 489.7±145.6 0.6
Table3–AssociationbetweenrheumatoidarthritisanddifferentpolymorphicformsofMTHFRC677T,MTHFRA1298C, TGF-1T869CandLT-␣A252G.
Genotypeand allele
Patients Control p OR(95%CI)
n % n %
MTHRFC677T
CC 46 44.2 64 71.1
CT 50 48.1 22 24.4 0.011 3.16(1.30–7.69)
TT 8 7.7 4 4.4 0.260 2.78(0.47–16.5)
C 142 68.3 159 83.3
T 66 31.7 30 16.7 0.028 2.18(1.09–4.38)
MTHFRA1298C
AA 46 44.2 20 22.2
AC 34 32.7 56 62.2 0.006 0.26(0.10–0.69)
CC 24 23.1 14 15.6 0.629 0.75(0.23–2.45)
A 126 60.6 96 53.3
C 82 39.4 84 46.7 0.383 0.74(0.42–1.32)
TGF-1T869C
TT 18 17.3 20 22.2
CT 68 65.4 36 40.0 0.173 2.10(0.72–6.10)
CC 18 17.3 34 37.8 0.390 0.59(0.18–1.97)
C 104 50 104 58
T 104 50 76 42 0.313 0.73(0.41–1.29)
LT-␣A252G
AA 6 5.8 16 28.9
AG 42 40.4 48 17.8 0.252 2.33(0.55–9.95)
GG 56 53.8 26 53.3 0.021 5.74(1.31–25.26)
A 54 26 80 44
G 154 74 100 56 0.007 2.28(1.25–4.18)
Inthisstudy,serumlevelsofTNF-␣aresignificantlyhigher inpatientcomparedtocontrolgroup.Theresultsregarding TNF-␣arecoincidedwithresultsofpreviousstudiessuchas Gheitaetal.,21andIsmailetal.,22whoexplainedtheseresults byitsvitalandcentralroleintheetiologyandpathogenesisof RA,henceTNFinhibitorswerethefirstofthebiologicaldisease modifyinganti-rheumaticdrugs(DMARDs)tobeapprovedfor the treatmentof RAand now theyare partof the routine treatmentofpatientswiththisdisease.23However,Ebrahimi etal.,24reportednon-significantincreaseinserumTNF-␣ lev-elsinpatientswhencomparedtocontrolgroup.
Also, our results showed significant increase in serum OPNlevelsinpatientswithRAthaninhealthycontrolgroup which are in accordance with results of Ji et al.,25 Chen et al.26 who explained these results by the cardinal role of OPN and its receptors in pathogenesis of RA. So, sev-eralexperimentalstudiesaimingtouseOPNastherapeutic
targetarebeingperformedandtheoutcomesoftheseresults arepromising.27
On the contrary,the serum BAFF showed no significant difference betweenbothgroupswhich iscomingwith pre-vious resultsofEldin et al.28 However,Mahdyet al.,29 and Mouraet al.,30 reported significantincrease inserum BAFF levelsamongRApatientsespeciallypatientswithhigher dis-easeactivityandshorterdiseaseduration.Thisdiscrepancy inresultsmaybeattributedtodifferentdiseaseactivityand durationinthestudiedgroup.
TheCTgenotypeandTalleleofMTHFRC677Tare asso-ciatedwithRA,higherserumlevelofTNF-␣,buttheyhave nosignificanteffectonOPNandBAFFserumlevels.Onthe otherhand,thedifferentMTHFRA1298Cpolymorphicforms werenotassociatedwithRA,orserumlevelsofTNF-␣,OPN or BAFF. TheACgenotypeofMTHFRA1298 C showed pro-tective effect from the disease.Thismay bedue tohigher
Table4–Comparisonbetweenserumlevelsofosteopontin,TNF-␣andBAFFindifferentgenotypesinallstudiedcases (n=194).
Serumosteopontin(ng/ml) SerumTNF(pg/ml) SerumBAFF(pg/ml)
Geno-type Mean±SD p Mean±SD p Mean±SD p
MTHFRC677T
CC 8.32±7.75
0.248
19.20±15.076
0.031
505.16±149.65
0.162
CT 11.24±9.92 28.93±19.817 444.67±133.17
TT 11.62±7.91 25.62±16.080 486.83±197.19
MTHFRA1298C
AA 12.27±11.30
0.076
23.61±16.05
0.233
486.49±136.9793 0.233
AC 7.79±6.00 20.58±18.17 480.98±157.43
CC 9.293±8.00 28.75±17.85 474.47±151.22
TGF-1T869C
CC 6.79±5.99
0.151
22.17±11.99
0.018
518.42±164.63
0.137
CT 10.54±8.66 27.09±19.39 482.25±139.42
TT 10.91±11.07 14.04±15.32 429.32±139.09
LT-␣A252G
AA 14.99±16.98
0.075
14.43±3.62
0.004
525.27±174.13
0.542
AG 9.44±7.86 19.35±15.45 469.87±135.90
effect of MTHFR C677 T on MTHFR enzyme resulting in hyper-homocysteinaemiaandsubsequentcascadeofcytokine activation.Resultsofprevious studies wereheterogeneous; someshowednoassociationbetweenriskofRAanddifferent polymorphicformsofMTHFRC677TandA1298C.31,32 Oth-ersreportedassociationofTallele,butnotanyoftheMTHFR C677TpolymorphicformswithRA.3Rubinietal.33reported associationofCCgenotype ofMTHFRA1298 Cbut notany ofMTHFRC677Tpolymorphicformswithsusceptibility to RAinItalianpopulation. Thisheterogeneityinresultsmay beattributedtoracialvariationsinalleleand genotype fre-quenciesasreportedbyHughesetal.,32whofoundsignificant increaseinTalleleinMTHFRC677TandCalleleofMTHFR A1298C(independentondiseasestatus)inCaucasianswhen comparedtoAfricanAmericans.Also,asignificantinteraction betweenMTHFRpolymorphismsandnutrient/environmental factors(i.e.folatestatus,age,smokingandalcoholintake)was reported.4Transforminggrowthfactor-1(TGF-1)isan anti-inflammatorycytokineassociatedwithdiseaseremission,and inadditionhasthepotentialtobepro-inflammatorycytokine. PolymorphismsofTGF-1havebeen reportedtobe associ-atedwithvariationsintheserumlevelsofTGF-1andwith severaldiseases.34 Inthisstudy,the TGF-1(T869C) geno-typeswerenotassociatedwithRA.However,theCTgenotype wasassociatedwithsignificantincreaseinserumTNFwhen comparedtoTTgenotype.Thisiscomingwithresultsofthe twometa-analysisstudiesdonebyZhangetal.35andChang etal.36whichshowednoclearassociationofTGF-1T869C polymorphismandTallelewithRAonaworldwide popula-tionbutassociationwassuggestedonlyinthepeopleofAsian descent.TheresultsofHusseinetal.37wasdifferentasthey foundassociationofTGF-1TallelewithsusceptibilitytoRA inEgyptianpatients.Ourresultsalsoshowedassociationof theGalleleandtheGGgenotypeofLT-␣A252GwithRAand higherTNF-␣serumlevels.These resultsareinaccordance withthatofKarrayetal.38andAl-Rayesetal.,39whichreported associationbetweenGGandAAgenotypeswithRA,whileGA genotypewasrefractory.
From the above we can conclude that CT genotype of MTHFRC677T,ACgenotypeofMTHFRA1298CandGG geno-typeofLT-␣A252GareassociatedwithincreasedriskofRAin Egyptianpatients.
Toourknowledge,thisisthefirststudytoevaluate simulta-neouslytheassociationofMTHFRC677TandA1298C,TGF-1 T869 C and LT-␣ A252G polymorphisms with RAand with pro-inflammatorycytokinesTNF,BAFFandOPNinEgyptian patients.
Somelimitations werefacingthisstudy asitincluded a verybroadgroupofpatientsregardingdiseaseduration, dis-easeactivity,patientstakingdifferentdrugsandnomention wasmadeaboutrheumatoidfactorandAnti-CCPpositivity. Thecytokinesmeasurementsmayvarywidelywiththese fac-torsand alsowithothermethodology details,suchastime betweenthesampleiscollectedandprocessed,DAS-28,drugs andits’doseswhenthesampleswerecollected.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.HelmickCG,FelsonDT,LawrenceRC,GabrielS,HirschR, KwohCK,etal.Estimatesoftheprevalenceofarthritisand otherrheumaticconditionsintheUnitedStates.PartI. ArthritisRheum.2008;58:15–25.
2.VinayDS,KwonBS.TargetingTNFsuperfamilymembersfor therapeuticinterventioninrheumatoidarthritis.Cytokine. 2012;57:305–12.
3.InanirA,YigitS,TekcanA,TuralS,KismaliG.IL-4andMTHFR genepolymorphisminrheumatoidarthritisandtheireffects. ImmunolLett.2013;152:104–8.
4.DeMattiaE,ToffoliG.C677TandA1298CMTHFR polymorphisms,achallengeforantifolateand
fluoropyrimidine-basedtherapypersonalisation.EurJCancer. 2009;45:1333–51.
5.SpyridopoulouKP,DimouNL,HamodrakasSJ,BagosPG. Methylenetetrahydrofolatereductasegenepolymorphisms andtheirassociationwithmethotrexatetoxicity:a meta-analysis.PharmacogenetGenomics.2012;22: 117–33.
6.ErbN,KitasG.Homocysteinemodulationasareasonfor continuousfolicacidsupplementationin
methotrexate-treatedrheumatoidarthritispatients. Rheumatology.2001;40:715–6.
7.EpsteinFH,BlobeGC,SchiemannWP,LodishHF.Roleof transforminggrowthfactorinhumandisease.NEnglJMed. 2000;342:1350–8.
8.EvansCH,GhivizzaniSC,KangR,MuzzonigroT,WaskoMC, HerndonJH,etal.Genetherapyforrheumaticdiseases. ArthritisRheum.1999;42:1–16.
9.AokiCA,BorchersAT,LiM,FlavellRA,BowlusCL,AnsariAA, etal.Transforminggrowthfactorbeta(TGF-beta)and autoimmunity.AutoimmunRev.2005;4:450–9.
10.PerriconeC,CeccarelliF,ValesiniG.Anoverviewonthe geneticofrheumatoidarthritis:anever-endingstory. AutoimmunRev.2011;10:599–608.
11.VasanthiP,NaliniG,RajasekharG.Roleoftumornecrosis factor-alphainrheumatoidarthritis:areview.APLARJ Rheumatol.2007;10:270–4.
12.LuR,DouX,GaoX,ZhangJ,NiJ,GuoL.Afunctional polymorphismoflymphotoxin-alpha(LTA)geners909253is associatedwithgastriccancerriskinanAsianpopulation. CancerEpidemiol.2012;36:e380–6.
13.MesserG,SpenglerU,JungMC,HonoldG,BlomerK,PapeGR, etal.Polymorphicstructureofthetumornecrosisfactor (TNF)locus:anNcoIpolymorphisminthefirstintronofthe humanTNF-betagenecorrelateswithavariantaminoacidin position26andareducedlevelofTNF-betaproduction.JExp Med.1991;173:209–19.
14.Partida-RodríguezO,TorresJ,Flores-LunaL,CamorlingaM, Nieves-RamírezM,LazcanoE,etal.PolymorphismsinTNF andHSP-70showasignificantassociationwithgastriccancer andduodenalulcer.IntJCancer.2010;126:1861–8.
15.SunJ,LinZ,FengJ,LiY,ShenB.BAFF-targetingtherapy,a promisingstrategyfortreatingautoimmunediseases.EurJ Pharmacol.2008;597:1–5.
16.WangKX,DenhardtDT.Osteopontin:roleinimmune regulationandstressresponses.CytokineGrowthFactorRev. 2008;19:333–45.
17.VanderPutNM,GabreelsF,StevensEM,SmeitinkJA,Trijbels FJ,EskesTK,etal.Asecondcommonmutationinthe methylenetetrahydrofolatereductasegene:anadditionalrisk factorforneural-tubedefects?AmJHumGenet.
1998;62:1044–51.
acommonmutationinmethylenetetrahydrofolatereductase. NatGenet.1995:111–3.
19.WoodNA,ThomsonSC,SmithRM,BidwellJL.Identification ofhumanTGF-beta1signal(leader)sequencepolymorphisms byPCR-RFLP.JImmunolMethods.2000;234:117–22.
20.VasconcelosDF,DaSilvaMA,MarquesMR,DeBritoJuniorRB, VasconcelosAC,BarrosSP.Lymphotoxin-alphagene
polymorphism+252A/G(rs909253,A/G)isassociatedwith susceptibilitytochronicperiodontitis:aPilotStudy.ISRN Dent.2012;2012:617245.PubMedPMID:23050158.Pubmed CentralPMCID:3463161.
21.GheitaTA,AzkalanyGS,GaberW,MoheyA.Clinical significanceofserumTNF␣and-308G/Apromoter polymorphisminrheumatoidarthritis.EgyptRheumatol. 2015;37:49–54.
22.IsmailF,AliHA-H,IbrahimHM.Possibleroleofleptin,and tumornecrosisfactor-alphainhypoandrogenicityinpatients withearlyrheumatoidarthritis.EgyptRheumatol.
2011;4:209–15.
23.WillrichMA,MurrayDL,SnyderMR.Tumornecrosisfactor inhibitors:clinicalutilityinautoimmunediseases.TranslRes. 2015;165:270–82.
24.EbrahimiAA,NoshadH,SadreddiniS,HejaziMS,
MohammadzadehSadighY,EshraghiY,etal.Serumlevelsof TNF-alpha,TNF-alphaRI,TNF-alphaRIIandIL-12intreated rheumatoidarthritispatients.IranJImmunol.2009;6:147–53. 25.JiH-I,LeeS-H,SongR,YangH-I,LeeY-A,HongS-J,etal.
Serumlevelofosteopontinasaninflammatorymarkerdoes notindicatediseaseactivityorresponsivenesstotherapeutic treatmentsinpatientswithrheumatoidarthritis.Clin Rheumatol.2014;33:397–402.
26.ChenG,ZhangX,LiR,FangL,NiuX,ZhengY,etal.Roleof osteopontininsynovialTh17differentiationinrheumatoid arthritis.ArthritisRheum.2010;62:2900–8.
27.ZhangF,LuoW,LiY,GaoS,LeiG.Roleofosteopontinin rheumatoidarthritis.RheumatolInt.2015;35:589–95. 28.EldinAB,SayedS,HegazyG,ShakerO.B-CellActivating
Factor(BAFF)insystemiclupuserythematosus,rheumatoid arthritis,andBehc¸et’sdisease.ArchRheumatol.
2012;27:185–94.
29.MahdyAA,RaafatHA,El-FishawyHS,GheitaTA.Therapeutic potentialofhydroxychloroquineonserumB-cellactivating factorbelongingtothetumornecrosisfactorfamily(BAFF)in rheumatoidarthritispatients.BulletinofFacultyof
Pharmacy,CairoUniversity;2014.
30.MouraRA,CascãoR,PerpétuoI,CanhãoH,Vieira-SousaE, MourãoAF,etal.Cytokinepatterninveryearlyrheumatoid arthritisfavoursB-cellactivationandsurvival.Rheumatology. 2010:keq338.
31.Palomino-MoralesR,Gonzalez-JuanateyC,
Vazquez-RodriguezTR,RodriguezL,Miranda-FilloyJA, Fernandez-GutierrezB,etal.ResearcharticleA1298C polymorphismintheMTHFRgenepredisposesto cardiovascularriskinrheumatoidarthritis.HeartFail. 2010;5:2.3.
32.HughesLB,BeasleyTM,PatelH,TiwariHK,MorganSL, BaggottJE,etal.Racialorethnicdifferencesinallele frequenciesofsingle-nucleotidepolymorphismsinthe methylenetetrahydrofolatereductasegeneandtheir influenceonresponsetomethotrexateinrheumatoid arthritis.AnnRheumDis.2006;65:1213–8.
33.RubiniM,PadovanM,BaricordiO,FotinidiM,GovoniM, TrottaF.Thec.1298A>Cpolymorphisminthe
methylenetetrahydrofolatereductasegeneisassociatedwith rheumatoidarthritissusceptibilityinItalianpatients.Clin ExpRheumatol.2008;26:163.
34.AlayliG,KaraN,TanderB,CanturkF,GunesS,BagciH. Associationoftransforminggrowthfactorbeta1gene polymorphismwithrheumatoidarthritisinaTurkish population.JointBoneSpine.2009;76:20–3.
35.ZhangL,YanJ-W,WangY-X,WanY-N,LiJ-P,LiuP,etal. AssociationofTGF-1+869C/Tpromoterpolymorphismwith susceptibilitytoautoimmunediseases:ameta-analysis.Mol BiolRep.2013;40:4811–7.
36.ChangW-W,SuH,HeL,ZhaoK-F,WuJ-L,XuZ-W. Associationbetweentransforminggrowthfactor-1T869C polymorphismandrheumatoidarthritis:ameta-analysis. Rheumatology.2010;49:652–6.
37.HusseinYM,MohamedRH,El-ShahawyEE,AlzahraniSS. InteractionbetweenTGF-1(869C/T)polymorphismand biochemicalriskfactorforpredictionofdiseaseprogression inrheumatoidarthritis.Gene.2014;536:393–7.
38.KarrayEF,BendhifallahI,BenabdelghaniK,HamzaouiK, ZakraouiL.Tumornecrosisfactorgenepolymorphismsand susceptibilitytorheumatoidarthritisinregionalTunisian population.JInfectDisImmun.2011;3:30–5.