rev bras ortop.2015;50(3):270–273
w w w . r b o . o r g . b r
Original
Article
Safety
zone
for
surgical
access
in
the
middle
third
of
the
clavicle:
study
on
cadavers
夽
Fabiano
Rebouc¸as
Ribeiro,
Fernanda
de
Marchi
Bosi
Porto
∗,
Marcio
Vieira
Sanches
Silva,
Antonio
Carlos
Tenor
Junior,
Miguel
Pereira
da
Costa,
Cantidio
Filardi
HospitaldoServidorPúblicoEstadualdeSãoPaulo,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received3February2014 Accepted26May2014 Availableonline17June2015
Keywords:
Clavicle/surgery Clavicle/anatomy Cadaver
a
b
s
t
r
a
c
t
Objective:Theaimofthisstudywastoestablishaneurovascularsafetyzoneforsurgical accessinthemiddlethirdoftheclavicle,bymeansofdissectiononcadavers.
Methods:Twentyshouldersweredissectedin10cadavers,withdeepdissectionofthemiddle thirdoftheclavicle.Thefollowingstructureswereidentified:subclavianvein,uppertrunk ofthebrachialplexus(anteriorandposteriordivisions)andsuprascapularnerve.These structuresweremarkedoutinordertomeasuretheirdistancesfromthemostproximal pointofthemiddlethirdoftheclavicle.
Results:Themeandistancesfromthemiddlethirdoftheclavicletothesuprascapularnerve, subclavianvein,uppertrunk,anteriordivisionoftheuppertrunkandposteriordivisionof theuppertrunkwererespectively,fortherightside:15.92cm,10.77cm,23.68cm,14.60cm and15.42cm;andfortheleftside:12.69cm;9.82cm;22.19cm;12.16cmand13.46cm.
Conclusion:Therewasastatisticaldifferenceinthedistancestothesuprascapularnerve andanteriordivisionoftheuppertrunk,incomparingbetweentherightandleftsides.The closestneurovascularstructurestothemiddlethirdoftheclaviclewerethesuprascapular nerveandsubclavianvein.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Zona
de
seguranc¸a
no
acesso
cirúrgico
do
terc¸o
médio
da
clavícula:
estudo
em
cadáveres
Palavras-chave:
Clavícula/cirurgia Clavícula/anatomia Cadáver
r
e
s
u
m
o
Objetivo:Estabelecerumazonadeseguranc¸aneurovascularnoacessocirúrgicodoterc¸o médiodaclavículapordissecc¸ãoemcadáveres.
Métodos:Foramdissecados20ombrosde10cadáveres,foifeitaadissecc¸ãoprofundadoterc¸o médiodaclavículaeidentificaram-seasseguintesestruturas:veiasubclávia,troncosuperior doplexobraquial(divisãoanterioreposterior)enervosupraescapular.Essasestruturas foramdemarcadasparamensurac¸ãodesuasdistânciasatéospontosmaispróximosdo terc¸omédiodaclavícula.
夽
WorkdevelopedintheHospitaldoServidorPúblicoEstadualdeSãoPaulo,SãoPaulo,SP,Brazil.
∗ Correspondingauthor.
E-mails:[email protected],[email protected](F.deMarchiBosiPorto).
http://dx.doi.org/10.1016/j.rboe.2015.06.005
rev bras ortop.2 0 1 5;50(3):270–273
271
Resultados: Adistânciamédiadoterc¸omédiodaclavículaaonervosupraescapular,àveia subclávia,aotroncosuperior,àdivisãoanteriordotroncosuperioreàdivisãoposteriordo troncosuperiorfoi,respectivamente,doladodireito:15,92cm;10,77cm;23,68cm;14,60cm e15,42cm;doladoesquerdo:12,69cm;9,82cm;22,19cm;12,16cme13,46cm.
Conclusão: Houve diferenc¸aestatística entreasdistânciasdonervo supraescapularea divisão anterior do troncosuperior comparativaentre os lados direito e esquerdo. As estruturas neurovasculares maispróximas ao terc¸o médioda clavícula foram onervo supraescapulareaveiasubclávia.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Theclaviclehasimportantanatomicalrelationshipswiththe subclavianartery,subclavianveinandbrachialplexus, espe-ciallyinitsmiddlethird,wherethecurvatureisthereference pointusedforaccessingthesestructures.Incasesoftrauma and/orsurgeryinthemiddlethirdoftheclavicle,and espe-ciallyissituationsoffractures thatneedtobereducedand fixed bymeans ofopen surgery, Using synthesismaterial, thesestructuresmaybecomeinjuredbecauseoftheir anatom-icalproximity.1,2
ThebrachialplexusisformedbytherootsofC5,C6,C7, C8andT1.Itoriginatesfromthecervicalspine,headstoward theupperlimbsandpasses betweenthemiddle and ante-riorscalenemuscles.TherootsofC5andC6formtheupper trunk, from which the suprascapular nerve emerges. Each trunkdivides into anterior and posterior portions when it passesbelowtheclavicle.3
Theright subclavian artery is a branch ofthe brachio-cephalictrunkandthe leftsubclavianarteryisabranchof theaortic arch.Thereference anatomicalstructureforthe subclavianarteryistheanteriorscalenemuscle,andthiscan befoundattheposteromedialborderofthismuscleoratits lateralborder.Thesubclavianvein isa continuationofthe axillaryveinandextendsfromtheborderofthefirstribtothe medialborderoftheanteriorscalenemuscle,whereitjoins theinternaljugularveintoformthebrachiocephalicvein.The clavicleandthesubclavianmusclearelocatedanteriorlytothe subclavianvein.1
Theaimof this study was toestablish a neurovascular safetyzoneatthesurgicalaccesstothemiddlethirdofthe clavicle,bymeansofdissectionincadavers.
Methods
Ten recently chilled cadavers were selected. Three were femaleandsevenweremale.Theirmeanagewas63.6years (range:55–73),mean height1.67m(1.58–1.73),mean weight 62kg(40.4–77)andmeanBMI22.1kg/m2(16.1–25.65).Theydid
notpresentanycongenitalabnormalities,signsoftraumaor previoussurgeryintheshouldersstudied.Allthedissections were performed bythe same group ofresearchers. A pilot studywas initiallyconductedonthefour shouldersoftwo
cadavers,beforedata-gatheringwasstarted,inordertostudy andgainbetterknowledgeofthelocalanatomy(Table1).
The procedures were performed with the cadaver in a standardizedhorizontaldorsaldecubitusposition,withapad undertheipsilateral scapulaand theupperlimbinneutral position.Usingasurgicalpen,thesuperficialanatomyofthe clavicleandtheacromioclavicularandsternoclavicularjoints wasmarkedoutontheskin.Atransverseincisionwasmadein theskinalongtheentirelengthoftheclavicleandthemuscle layersweredissected,withexposureofthesubclavianmuscle (originandinsertion).Itsrelationshipwiththemiddlethirdof theclaviclewasdemonstratedusingmarkersanteroinferiorly (Fig.1).
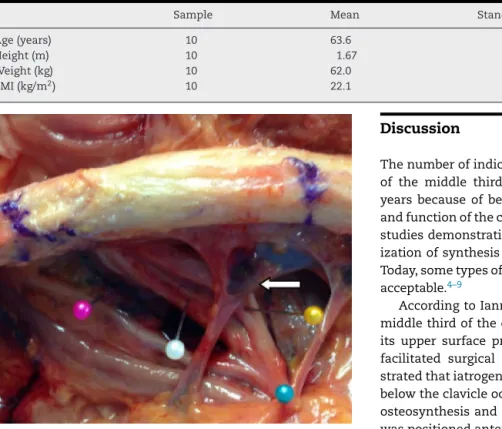
Afterexposureofthemuscle,theclaviclewasdividedinto threethirdsand deeperdissectionofthemiddle thirdwas performed. In this, the following neurovascular structures wereidentified:subclavianvein,uppertrunkofthebrachial plexus(anterior andposterior divisions)and suprascapular nerve.Thesestructuresweredemarcatedusingcolored mark-ersandthedistancestotheclosestpointofthemiddlethird oftheclaviclewasrecordedusingaKingtools®150mmdigital
pachymeter(Fig.2).
Forthestatisticalanalysis,thepairedWilcoxontestwas used.Thesignificanceleveladoptedwas5%andthesoftware usedfortheanalysiswasSASversion9.2.
Results
Themeandistancesfromthemiddlethirdoftheclavicletothe suprascapularnerve, subclavianvein,uppertrunk,anterior
272
rev bras ortop.2 0 1 5;50(3):270–273Table1–Descriptionofthesamples,ages,heights,weightsandBMI.
Sample Mean Standarddeviation Median
Age(years) 10 63.6 5.5 62.5
Height(m) 10 1.67 0.06 1.68
Weight(kg) 10 62.0 11.7 66.0
BMI(kg/m2) 10 22.1 3.5 22.9
Fig.2–Pinkmarker:suprascapularnerve;greenmarker: uppertrunk;whitemarker:posteriordivisionoftheupper trunk;yellowmarker:anteriordivisionoftheuppertrunk; whitearrow:subclavianvein.
divisionoftheuppertrunkandposteriordivisionoftheupper trunkontherightsidewere,respectively:15.92cm;10.77cm; 23.68cm;14.60cm;and15.42cm;andontheleftside:12.69cm; 9.82cm;22.19cm;12.16cm;and13.46cm.
Table2presentstheresultsfromthemeasurementsmade
betweenthemiddlethirdoftheclavicleandtheneurovascular structuresstudied.
Discussion
Thenumberofindicationsforsurgicaltreatmentoffractures of the middle third ofthe clavicle has increasedover the years becauseofbetterunderstanding ofthe biomechanics andfunctionoftheclavicle,thegreaternumberofprospective studiesdemonstratingcomparativeresultsandthe modern-izationofsynthesismaterialsforfixationofthesefractures. Today,sometypesofshorteninganddeformitiesarenolonger acceptable.4–9
AccordingtoIannottietal.6treatmentoffracturesofthe
middlethirdoftheclaviclethroughplacementofaplateon its uppersurface presentedbiomechanical advantagesand facilitated surgical access. However, Kloen et al.7
demon-stratedthatiatrogeniclesionsoftheneurovascularstructures belowtheclavicleoccurredmorefrequentlyinthesetypesof osteosynthesisandthattheriskdiminishedwhentheplate waspositionedanteroinferiorly.6,7
Labrocini etal.10 demonstratedthatthe branchesofthe
suprascapular nerve, which are responsible for the sensi-tivity on the clavicle, and the anteromedial region of the shoulderandproximalregionofthechestarevulnerablein casesoffracturesoftheclavicleandtheirsurgicaltreatment. According toSinhaetal.4 thestructuresatgreatestriskof
injuryduringosteosynthesisofthemiddlethirdofthe clav-icle are the subclavianvein,subclavian artery,the brachial plexusandthepulmonarypleura.Accordingtotheirstudy, thesubclavianveinwasclosertothemiddlethirdofthe clav-icle thanwas thebrachialplexus,withamean distanceof 12.45mm. In ourstudy, theright subclavian veinwas ata meandistanceof10.77mmandtheleftat9.82mmfromthe
Table2–Means,standarddeviations,mediansandpvaluesofthedistancesbetweentheanatomicalstructuresandthe
middlethirdoftheclavicle.
Sample Mean Standarddeviation Median pvalue
Rightsuprascapularnerve 10 15.92 5.32 15.53
Leftsuprascapularnerve 10 12.69 13.02
Difference 10 3.23 3.75 2.91 0.0273a
Rightsubclavianvein 10 10.77 3.23 10.49
Leftsubclavianvein 10 9.82 4.04 8.75
Difference 10 0.95 2.27 1.39 0.2754
Rightuppertrunk 10 23.68 6.04 22.38
Leftuppertrunk 10 22.19 6.41 20.10
Difference 10 1.50 2.61 1.74 0.1309
Rightanteriordivision 10 14.60 5.76 13.64
Leftanteriordivision 10 12.16 4.00 12.67
Difference 10 2.44 2.96 2.18 0.0371a
Rightposteriordivision 10 15.42 5.16 15.39
Leftposteriordivision 10 13.46 3.82 13.17
Difference 10 1.96 3.30 2.65 0.1055
rev bras ortop.2 0 1 5;50(3):270–273
273
middlethirdoftheclavicleandwasalsotheclosestvascular structure.4,10
AccordingtoMouzopoulosetal.8theassociationbetween
fracturesoftheclavicleandinjuriestothebrachialplexusis wellknownandusuallyoccursduetohigh-energy supraclav-iculartraction. Fracturesoftheclavicleareassociatedwith theseeventsbutarenotthecausalfactor.Inanotherstudy, byDellaSantaetal.9itwasdemonstratedthatdirecttrauma
ofthe brachial plexus caused byfragments of the clavicle occurredatlowfrequency(1%).8,9
Jeyaseelanetal.11reportedthatinvolvementofthe
supras-capularnerveisacommonfindinginfracturesoftheclavicle, becausethis is the structureofthe brachial plexusthat is closesttothemiddlethirdoftheclavicle.Shorteningofthe clavicleandmobilizationofthefragmentsofthefracture dur-ingfixationmaycausecompressionofthebrachialplexus,due tothedecreasedinfraclavicularspace.Inconservative treat-ment,thepresenceofthebonecallusmayalsobethecause oflesionsofthesuprascapularnerve,duetocompression.In ourstudy,thebrachialplexusstructurethatwasclosesttothe middlethirdoftheclaviclewasthesuprascapularnerve.11
Therefore,accordingtotheliteratureconsulted, periclavic-ularneurovascularlesionsaremoreassociatedwithsurgical iatrogeniclesionsthanwiththetraumaitself.Inourstudy, theneurovascular structuresclosest tothe middle thirdof theclavicularandthereforemostsusceptibletoinjuryinthis region were the suprascapular nerve and subclavian vein, respectively.Duringourdissections,itwasalsoobservedthat thesubclavianmuscleprovidedanterosuperiorprotectionfor the adjacent neurovascular structuresand that it could be usedasananatomicalreferencepointfordelimitinga“safety zone”.
Conclusion
Therewasastatisticaldifference inthedistancesfromthe suprascapularnerveand theanterior divisionofthe upper trunk,comparatively between the right and left. The neu-rovascularstructuresclosesttothemiddlethirdoftheclavicle werethesuprascapularnerveandsubclavianvein.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.StandringS.Gray’sanatomy:theanatomicalbasisofclinical
practice.40thed.NewYork:ChurchillLivingstone;
2008.
2.BasamaniaCJ,RockwoodCAJr.Fracturesoftheclavicle.In:
RockwoodCAJr,MatsenFA3rd,WirthMA,LippittSB,editors.
Theshoulder.4thed.Philadelphia:Saunders;2009.
p.617–770.
3.ShinAY,SpinnerRJ,SteinmannSP,BishopAT.Adult
traumaticbrachialplexusinjuries.JAmAcadOrthopSurg.
2005;13(6):382–96.
4.SinhaA,EdwinJ,SreeharshaB,BhalaikV,BrownsonP.A
radiologicalstudytodefinesafezonesfordrillingduring
platingofclaviclefractures.JBoneJointSurgBr.
2011;93(9):1247–52.
5.JerayKJ.Acutemidshaftclavicularfracture.JAmAcadOrthop
Surg.2007;15(4):239–48.
6.IannottiMR,CrosbyLA,StaffordP,GraysonG,GouletR.
Effectsofplatelocationandselectiononthestabilityof
midshaftclavicleosteotomies:abiomechanicalstudy.J
ShoulderElbowSurg.2002;11(5):457–62.
7.KloenP,WernerCM,StufkensSA,HelfetDL.Anteroinferior
platingofmidshaftclaviclenonunionsandfractures.Oper
OrthopTraumatol.2009;21(2):170–9.
8.MouzopoulosG,MorakisE,StamatakosM,TzurbakisM.
Complicationsassociatedwithclavicularfracture.Orthop
Nurs.2009;28(5):217–24.
9.DellaSantaD,NarakasA,BonnardC.Latelesionsofthe
brachialplexusafterfractureoftheclavicle.AnnChirMain
MembSuper.1991;10(6):531–40.
10.LabroniciPJ,SegallFS,MartinsBA,FrancoJS,LabroniciGJ,
SilvaBA,etal.Fraturadaclavícula–incidênciadelesãodo
nervosupraclavicular.RevBrasOrtop.2013;48(4):
317–21.
11.JeyaseelanL,SinghVK,GhoshS,SinisiM,FoxM.Iatropathic
brachialplexusinjury:acomplicationofdelayedfixationof