w w w . r b o . o r g . b r
Original
Article
Arthroscopic
treatment
for
chronic
lateral
epicondylitis
夽
Bernardo
Barcellos
Terra
∗,
Leandro
Marano
Rodrigues,
Anis
Nahssen
Filho,
Gustavo
Dalla
Bernardina
de
Almeida,
José
Maria
Cavatte,
Anderson
De
Nadai
SantaCasadeMisericórdiadeVitória,Vitória,ES,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received28June2014 Accepted15September2014 Availableonline9July2015
Keywords:
Tenniselbow/complications Tenniselbow/surgery Tenniselbow/therapy Arthroscopy
a
b
s
t
r
a
c
t
Objective:Toreporttheclinicalandfunctionalresultsfromarthroscopicreleaseoftheshort radialextensorofthecarpus(SREC)inpatientswithchroniclateralepicondylitisthatwas refractorytoconservativetreatment.
Methods:Overthe period fromJanuary2012 toNovember2013, 15 patientsunderwent arthroscopic treatment. Thesurgical technique usedwas theone described byRomeo andCohen,basedonanatomicalstudiesoncadavers.Theinclusioncriteriawerethatthe patientsneededtopresentlateralepicondylitisandthatconservativetreatment(analgesics, anti-inflammatoryagents,corticoidinfiltrationorphysiotherapy)hadfailedoveraperiod ofmorethansixmonths.Thepatientswereevaluatedbasedontheelbowfunctionalscore oftheMayoClinic,Nirschl’sstagingsystemandavisualanalogscale(VAS)forpain.
Results:Atotalof15patients(9menand6women)wereincluded.ThemeanMayoelbow functionalscoreaftertheoperationwas95(rangingfrom90to100).ThepainVASimproved fromameanof9.2beforetheoperationto0.64aftertheoperation.OnNirschl’sscale,the patientspresentedanimprovementfromameanof6.5beforetheoperationto approxi-matelyone.Thereweresignificantdifferencesfrombeforetoafterthesurgeryforthethree functionalscoresused(p<0.01).NocorrelationswereobservedusingtheSpearmantest betweentheresultsandage,gender,lengthoftimewithsymptomsbeforetheoperationor injurymechanism(p>0.05).
Conclusion: Arthroscopictreatmentforlateralepicondylitiswasshowntobeasafeand effec-tivetherapeuticoptionwhenappropriatelyindicatedandperformed,inrefractorycasesof chroniclateralepicondylitis.Italsoallowedexcellentviewingofthejointspacefor diagnos-ingandtreatingassociatedpathologicalconditions,withaminimallyinvasiveprocedure.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽
WorkperformedwithintheShoulderandElbowGroup,DepartmentofOrthopedicsandTraumatology,SantaCasadeMisericórdiade Vitória,Vitória,ES,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](B.B.Terra). http://dx.doi.org/10.1016/j.rboe.2015.06.015
Palavras-chave:
Cotovelode
tenista/complicac¸ões Cotovelodetenista/cirurgia Cotovelodetenista/terapia Artroscopia
Objetivo: Relatarosresultadosclínicosefuncionaisdaliberac¸ãoartroscópicadoextensor radialcurtodocarpo(ECRB)nospacientescomepicondilitelateralcrônicarefratáriaao tratamentoconservador.
Métodos: Noperíodocompreendidoentrejaneirode2012enovembrode2013,15pacientes foramsubmetidosaotratamentoartroscópico.Atécnicacirúrgicausadaéadescritapor Romeo eCohen,baseadaem estudosanatômicosem cadáver.Os critériosde inclusão forampacientescomepicondilitelateralnosquaisotratamentoconservador(analgésicos, antiinflamatórios,infiltrac¸ãode corticoides,fisioterapia)falhoupor maisdeseismeses. OspacientesforamavaliadoscombasenoescorefuncionaldecotovelodaClinicaMayo, SistemadeEstágiodeNirschleescalavisualanalógicadedor.
Resultados: Foramincluídos15pacientes,novehomenseseismulheres.Amédiadoescore funcionaldecotovelodeMayopós-operatóriofoide95(de90a100).AEVSdadorteveuma melhoriamédiade9,2nopré-operatóriopara0,64nopós-operatório.PelaescaladeNirschl ospacientesapresentaramumamelhoriamédiade6,5nopré-operatóriopara aproximada-menteum.Foiobservadadiferenc¸asignificanteentrepréepós-cirúrgiconostrêsescores funcionaisusados(p<0,01).Nãoforamobservadascorrelac¸õespelotestedeSpearmanentre idade,gênero,tempodesintomaspré-operatório,mecanismodelesãocomosresultados (p>0,05).
Conclusão:Otratamentoartroscópicodaepicondilitelateralmostra-secomoumaopc¸ão ter-apêuticaseguraeeficazquandoindicadoefeitodeformaadequadanoscasosrefratáriosde epicondilitelateralcrônicaepermiteaindaumaexcelentevisualizac¸ãodoespac¸oarticular paradiagnósticoetratamentodepatologiasassociadascomumprocedimento minima-menteinvasivo.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Lateralepicondylitis,alsoknownastenniselbow,isadisorder withanestimatedprevalenceof1–3%,peakingespecially dur-ingthefifthdecadeoflife,andwithgreateroccurrenceamong men,withapproximateproportionsof3:1.Thisconditionis oneofthemaincausesofpaininthe elbowand isrelated tosportssuchastennisandtomanualworkactivities. More-over,lateralepicondylitisoftenhasagreatfinancialimpacton society,withregardtobothworkleaveandtreatment.
Thepathologyofthisconditionisasourceofcontroversy, althoughtherearedescriptionsintheliteraturethatdateback tothe1970s.Mostcasesarebelievedtobecausedbya muscu-lotendinouslesionattheoriginoftheproximalextensorsof thelateralepicondyle,especiallyoftheshortradialextensor ofthecarpus.1–3
Theliteratureisvastregardingtypesoftreatment,from relativeresttosurgicaltreatment.However,controversystill exists regarding the best form of treatment. Conservative treatmentpresentsexcellentresults,althoughsurgical treat-mentbecomesanoptionwhenitfails(approximately12%) andinrefractorychroniccases.4–7
Arthroscopic treatment has recently been described as havingthe advantagesof allowingviewing ofconcomitant intra-articularlesions,notviolating the aponeurosisofthe extensorsandhavingashorterrehabilitationperiodandlower
complicationrate.8,9 Theobjectiveofthepresentstudywas toreporttheclinicalandfunctionalresultsfromarthroscopic release oftheshortradialextensorofthecarpus (SREC)in patientswithchroniclateralepicondylitisthatwasrefractory toconservativetreatment.
Methods
BetweenJanuary2012andNovember2013,15patients under-went arthroscopic treatmentforlateral epicondylitisofthe elbowatthe ShoulderandElbowGroupofourDepartment ofOrthopedicsandTraumatology.
Theinclusion criterion was thatthe patients neededto presentlateralepicondylitisforwhichconservativetreatment (analgesics,anti-inflammatorydrugs,corticoidinfiltrationor physicaltherapy)hadfailedoveraperiodofmorethansix months.Thediagnosiswasmadebasedontheclinicalhistory, physicalexaminationandmagneticresonanceexamination (Figs.1and 2).Theexclusioncriteriawereprevioussurgery or fractures on the ipsilateral elbowand presenceof con-comitant disorders,such aslateral compartmentarthrosis, posterior interosseoussyndrome, osteochondritisdissecans ofthecapitellum,instabilityandrheumatologicaldiseases.
Fig.1–Magneticresonanceimagingofcoronalsection showingalesionoftheshortradialextensortendon.
oftheMayoClinic,Nirschlstagingsystemandavisual ana-logscaleofpain.Thevisualanalogscaleofpainconsistedof arulermeasuring10cminlength,onwhichoneend repre-sentedabsenceofpainandtheotheraveryintensepain.The Nirschlsystemconsistedofsevenphasesinincreasingorder ofpainintensity,goingfromPhase1(slightpainwithexercise thatwasresolvedwithin24h)toPhase7(constantpainwhen restingthatdisruptedsleep).Thescoreswereobtainedbefore
Fig.2–Magneticresonanceimagingofcoronalsection showingalesionwithtearingoftheshortradialextensor tendon.
Fig.3–Arthroscopicportalsdrawnontherightelbow.
surgeryandduringthepostoperativeperiodaftertwoandsix weeks,andaftersixmonths.
Surgicaltechnique
The surgical technique used was described byCohen and Romeo,10basedonanatomicalstudiesoncadavers.
Positioning
Thepatientwaspositionedinventraldecubituswitha sup-portfortheupperlimbthatallowedarangeofmotionof120 degrees,fromflexiontocompleteextension.Asterilemanual tourniquetwasusedatthelevelofthemiddlethirdofthearm. The anatomical references (medial and lateral epicondyle, radialhead,olecranonandulnarnerve)andarthroscopic por-tals (proximalanteromedialandanterolateraland,insome cases,thestandardposteriorandposterolateral)weremarked ontheskin,asillustratedinFigs.3and4.
Approximately 20mlof sterile0.9% saline solution was injectedthroughthesoftspotportaldelineatedbytheradial head,olecranonandlateralepicondyle.Throughthis,ablunt trocarwasinsertedthroughtheanteromedialportalusingthe cannulaofthearthroscope.Anopticaldevicewitha30◦angle
Fig.4–Opticaldevicepositionedintheproximal
anteromedialportalandshaverpositionedintheproximal anterolateralportal.
locationsoftheposteriorinterosseousnerveandshortradial extensorofthecarpus(whichoriginatesneartothelevelof thejointsurfaceofthecapitellum)aretakenintoaccount.The debridedareaofthelateralcondyleistrapezium-shapedwith approximatedimensionsof13mm×7mm,slightlymore dis-talandanteriortothesiteoftheapexofthelateralepicondyle. Thedimensionsofthetipoftheshaver(4.5mm)canhelpwith thesemeasurements.7
Thecapsuleispartiallyresectedandopenedusinga4.5mm soft-tissueshaverthatexposestheoriginoftheshort exten-sor,whichisextra-articularandshouldberesectedasfaras theupperaspectofthecapitellum.Themusclefibersofthe long radialextensor are thus exposed (Figs.5 and6). Care needstobetakenregardingthe fibersofthe lateral collat-eralligament,whichmarktheposteriormarginofthearea thatshouldberesected,andalsoregardingthefibersofthe commonextensorofthefingers,whichissuperficialtothe shortradialextensor.Afterreleasingtheshortradialextensor, microperforationswerecreatedusingaSteinmanwire(Fig.7). During the postoperativeperiod, abracewas placedon theelbowandwasmaintainedforfivedays.Passiverangeof motionexerciseswerestartedassoonasthepatient’sstateof painallowedthis.Isometricstretchingexerciseswerestarted assoon asacomplete range ofmotionhadbeen acquired andresistanceexerciseswerestartedfourtosixweeksafter
Fig.5–Soft-tissueshaverreleasingtheshortradial extensor.
Fig.6–Soft-tissueshaverreleasingtheshortradial extensor.Notethemusclefibersofthelongradialextensor.
theoperation.Thepatientsreturntotheirphysicalactivities withoutrestrictions10weeksaftertheoperation.
Descriptiveanalysiswascarriedoutonthenumericaland categorical variables (Tables 1 and 2). Nonparametric tests wereusedinthedataanalysisbecausethedatadidnotfollow normaldistribution.Thepreandpostoperativeresultsfrom theVAS,MayoandNirschlscaleswerecomparedusingthe Mann–Whitneynonparametrictest.Therelationshipsofage andtimeofinjurywiththeresults(postoperativeMayoresults) wereassessedusingSpearman’s correlationtest.Difference betweengendersandtraumamechanismsinrelationtothe results(postoperativeMayoscore)wereinvestigatedthrough theMann–Whitneytest.Thevalueofpwastakentobe0.05 forallstatisticalinferences.ThesoftwareusedwasSPSSfor Windowsversion20.0.
Results
Fifteenpatients(9menand6women)wereincludedinthe present study.Themeanage ofthepatientson thedayof surgerywas38±8.7years.Thedominantlimbwasinvolved inalmost75%ofthecases.
Table1–Descriptiveanalysis.
N Mean SD Median Min Max
Age
General 15 38.3 8.7 38.5 23 52
Male 9 38 9.8 37.5 27 52
Female 6 37.6 8.0 38.5 23 45
Timeofinjury
General 15 6.93 0.9 7 6 9
Male 9 6.81 1.1 6.5 6 9
Female 6 7.0 0.8 7 6 8
PreoperativeVAS
General 15 9.21 0.6 9 8 10
Male 9 9.13 0.6 9 8 10
Female 6 8.48 0.8 9.5 8 10
PostoperativeVAS
General 15 0.64 0.7 0.5 0 2
Male 9 0.63 0.7 0.5 0 2
Female 6 0.67 0.8 0.5 0 2
PreoperativeMayo
General 15 60.00 4.8 60 50 65
Male 9 61.25 4.4 62.5 55 65
Female 6 58.33 5.1 60 50 65
PostoperativeMayo
General 15 95.71 3.8 95 90 100
Male 9 96.25 3.5 95 90 100
Female 6 95 4.4 95 90 100
PreoperativeNirschl
General 15 6.5 0.5 6.5 6 7
Male 9 6.5 0.5 6.5 6 7
Female 6 6.5 0.5 6.5 6 7
PostoperativeNirschl
General 15 1.07 0.2 1 1 2
Male 9 1.13 0.3 1 1 2
Female 6 1 0 1 1 1
Flexiononoperatedside
General 15 149 11.2 152 120 160
Male 9 148 7.5 148 138 160
Female 6 151 15.5 157 120 160
Flexiononnon-operatedside
General 15 138.9 8.2 139 130 160
Male 9 139 5.3 139 134 150
Female 6 138 11.6 135 130 160
Extensiononoperatedside
General 15 −2 1.5 −2 0 −4
Male 9 −1.75 1.2 −2 0 −4
Female 6 −2.3 1.9 −3 0 −4
Extensiononoperatedside
General 15 0 1.3 0 −2 2
Male 9 −0.25 1.28 0 −2 2
Female 6 0.33 1.5 0 −2 2
Atotalof60%ofthepatientsindicatedthatthecauseof theirinjurywasactivitiesthatwererequiredintheir profes-sions.Theothercausesreportedincludedrepeatedoverload in40%,tennisin30%andatraumaticeventin30%.
Thepatientsunderwentsurgeryafterameantimeperiod
ofseven months sincethe beginning of symptoms. Three
patients underwent application ofcorticoid locally, with a
maximumoftwodoses.
The mean time taken for the surgical procedure was
20min.
ThepostoperativemeanMayoelbowfunctionalscorewas
95(range:90–100).TheVASpainscoreimprovedfroma pre-operativemeanof9.2toapostoperativemeanof0.64.Onthe Nirschlscale,thepatientspresentedanimprovementfroma
mean of6.5beforesurgerytoapproximately 1.0,andsome
Gender
Male 9 60
Female 6 40
Useofcorticoid
Yes 3 20
No 12 80
Sideofinjury
Dominant 11 73.3
Non-dominant 4 26.6
Traumamechanism
Profession 9 60
Sport 6 40
Table3–Comparisonofbeforeandafteroperation, accordingtoVAS,MayoandNirschlscores.
N Mean SD Median Min Max pvalue
VAS
Pre 15 9.21 0.6 9 8 10 0.000a
Post 15 0.64 0.7 0.5 0 2
Mayo
Pre 15 60.00 4.8 60 50 65 0.001a Post 15 95.71 3.8 95 90 100
Nirschl
Pre 15 6.5 0.5 6.5 6 7 0.001a
Post 15 1.07 0.2 1 1 2
a pvalue<0.01.
Table4–Relationshipbetweenageandtimeofinjury andtheresults(postoperativeMayoscore).
Correlationcoefficienta pvalue
Age 0.21 0.44
Timeofinjury 0.38 0.15
a Spearman’scorrelationtest.
differencewasobservedfrombeforetoaftertheoperationfor allthreefunctionalscoresthatwereused(p<0.01)(Table3).
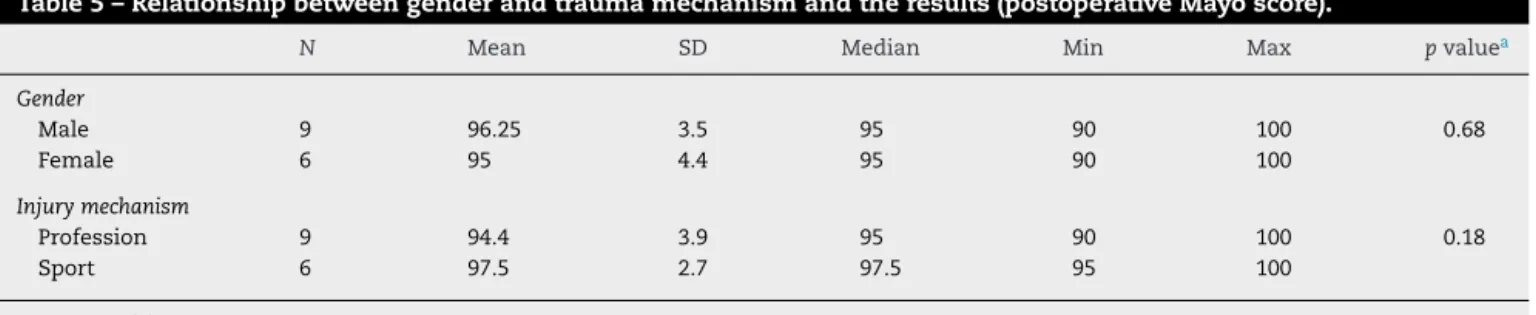
Nocorrelations were observedthrough Spearman’s test between age and the results (p=0.44), or any correlation betweenthetimeofinjuryandtheresults(p=0.15).The cor-relationcoefficientswerepositive,whichindicatesthatthere wasaproportionalrelationshipbetweenthetwovariables,e.g. thegreatertheage,thehigherthepostoperativeMayovalue was;andthegreaterthetimesincetheinjury,thehigherthe postoperativeMayovalueagainwas(Table4).Nosignificant differencewasobservedbetweenthegendersinrelationto theresults(postoperativeMayoscore)(p=0.68),or between thetraumamechanismandtheresults(postoperativeMayo score)(p=0.18)(Table5).
Thephysicalexaminationshowedameanextensionof−2◦
(range:−4to0)andflexionofapproximately150◦(range:120◦
to160◦).Noneofthepatientspresentedadifferenceof15◦or
moreinrangeofmotionbetweenonesideandtheother. Allpatientsreturnedtoworkonaveragesixweeksafter surgery.Amongthe15patients,14werecompletelysatisfied
Amongthe arthroscopicfindings,sixpatientspresented synovitisandtwopresentedfreebodies.
Complicationssuchastemporaryparesthesiaofthe fore-armwereobservedinonlyonecase.Anesthesiaintheulnar regionandposteriorinterosseousdeficitwerenotreported. Noothercomplicationswereobserved.
Discussion
Lateralepicondylitisisoneofthemaincausesofelbowpain, butcontroversyexistsregardingitsphysiopathologyand eti-ology. The most accepted theory proposes that micro and macrolesionsoccurattheoriginoftheextensors(especially the SREC) as an incomplete response to regeneration and thencauseaconditionoftendinosis.3,7,11Thisdemonstrates that the clinicalcondition isduetoavascular and fibrotic response(angiofibroblastic),andnotduetoaninflammatory process.Treatmentinmostcasesisconservativeandonlya small portion ofrecalcitrant casesare referred forsurgical treatment.12
Theliteraturedemonstratingdifferenttypesoftherapyfor treatingepicondylitisisvast,rangingfromclinicaland phys-iotherapeutictreatments,includingshockwaves,platelet-rich plasmaandcorticoid,tosurgery,whichcanbeopen, percuta-neousorarthroscopic.Ahmadetal.demonstratedtheuseof platelet-richplasma(PRP).13 Assendelftetal.14 conducteda systematicreviewthatcomparedthevalidityandresultsof randomizedclinicaltrialswithcontrolgroupsregardingthe useofcorticoidfortreatinglateralepicondylitis.Theseauthors reportedthattherewasashort-termbeneficialeffect(twoto sixweeks),but infollow-upsofmorethansixweeks,there werenostatisticallysignificantdifferencesbetweentheuse ofcorticoidandotherformsoftreatment,includingplacebo. Noconclusioncanbereachedregardingthetypeofcorticoid, dose,dosageintervalandvolumeinjected.
In a systematicreviewwith nine studies on the use of PRP for treating lateral epicondylitis, Ahmad et al.13 con-cludedthattheevidenceregardingPRPusewaslimited.Future investigationsare neededinordertobetterunderstandthe concentrationandmannerofpreparation,soastofacilitate thebestpossibleresult.Gosensetal.15comparedtheuseof PRP withcorticoid and found significantlysuperior results from thePRPgroupinrelationtotheDASHscore,overone andtwoyearsoffollow-up.
Miyazakietal.16reportedtheresultsfrom20patients oper-atedover aneight-year periodanddemonstrated that 65% hadexcellentoutcomes,accordingtotheBrucescale.There wasonecaseofreflexsympatheticdystrophy.Inthepresent study,therewasonecaseofparesthesiaofthelateralportion oftheforearm.Weusedasimilarsurgicaltechnique,although insteadofcarryingoutdecorticationofthelateralepicondyle withadrillbit,weusedaSteinmanwiretocreate microper-forationsinthelateralepicondyle.
Table5–Relationshipbetweengenderandtraumamechanismandtheresults(postoperativeMayoscore).
N Mean SD Median Min Max pvaluea
Gender
Male 9 96.25 3.5 95 90 100 0.68
Female 6 95 4.4 95 90 100
Injurymechanism
Profession 9 94.4 3.9 95 90 100 0.18
Sport 6 97.5 2.7 97.5 95 100
a Mann–Whitneytest.
withafollow-upof3.5years.Inthepresentstudy,wefound that95%oftheresultswereexcellent.Asinglefemalecase wasconsideredtohaveafairresult, with72 pointsonthe MayoClinicscale.
The results from the surgical treatment of lateral epi-condylitisarenotuniform,asalsoreportedbyotherstudies. Verhaaretal.17 reportedthat66%oftheirresultswere sat-isfactory,inoneoftheonlyprospectivestudiesonsurgical treatmentusingtheopentechniqueoverafollow-upperiod ofone year. In their study, onlyone third of the patients returned towork. Nirschl and Pettrone7 reported that 85% ofthe patients treated using the open technique achieved complete improvement of their symptoms. Baumgard and Schwartz18treated35patientsusingthepercutaneousrelease techniqueandobtainedexcellentresultsin91%.Inthepresent study,100%ofthepatientsreturnedtoworkwithinsixweeks andonlyonepatientwouldnotgothroughsurgeryagainif necessary.
Arthroscopic treatment with SREC release is an option forlateral epicondylitis. Owenet al.19 reported their surgi-calresultsfrom16patientsrelatingtoarthroscopicrelease, whoallachievedgoodresultsandreturnedtoworkwithno restrictionswithinsixdays.Inastudyon42patients,Baker etal.4reportedthat95%showedgoodresults,throughonly 62% patientswere practically pain-freeand 10% continued topresentapainfulconditionduringdailyactivities,similar totheresultsfromopenrelease.6,18,20,21Inthepresentstudy, amongthe15patientswhounderwentsurgery,90%were prac-ticallypain-freeoverthesix-weekfollowup.
Controversysurroundsthephysiopathologyof epicondyli-tis.Someauthorsreportthatitisanextra-articulardisorder. However, no studies have shown any difference in results between arthroscopic and open surgery.4 In the technique usedinthepresentstudy,capsulotomywasperformedinthe lateralregion,followedbyremovaloftheSRECfromits inser-tion,which isastructureadjacenttothejointcapsuleand thusdoes notaffect nearbystructures.Webelievethatthe arthroscopictechniqueenablesviewingofassociated intra-articularlesions,whichmayreachupto60%ofthecases.22 Moreover,thisallowsearlierrecovery,sinceitdoesnotviolate theaponeurosisoftheextensorsand doesnotcause dein-sertionofotherstructuresthathavenotbeenaffectedinthe angiofibroblasticprocess.
Conclusion
Arthroscopictreatmentforlateralepicondylitisisasafeand efficienttherapeuticoptionwhenindicatedandimplemented
appropriatelyinrefractorycasesofchroniclateral epicondyli-tis.Thistechniquealsoallowsexcellentviewingofthejoint space, in order to diagnose and treat associated disorders usingaminimallyinvasiveprocedure.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.EdwardsSG,CalandruccioJH.Autologousbloodinjectionsfor refractorylateralepicondylitis.JHandSurgAm.
2003;28(2):272–8.
2.LeadbetterWB.Cell-matrixresponseintendoninjury.Clin SportsMed.1992;11(3):533–78.
3.ReganW,WoldLE,CoonradR,MorreyBF.Microscopic histopathologyofchronicrefractorylateralepicondylitis.Am JSportsMed.1992;20(6):746–9.
4.BakerCLJr,MurphyKP,GottlobCA,CurdDT.Arthroscopic classificationandtreatmentoflateralepicondylitis:two-year clinicalresults.JShoulderElbowSurg.2000;9(6):475–82. 5.BoydHB,McLeodACJr.Tenniselbow.JBoneJointSurgAm.
1973;55(6):1183–7.
6.CoonradRW,HooperWR.Tenniselbow:itscourse,natural history,conservativeandsurgicalmanagement.JBoneJoint SurgAm.1973;55(6):1177–82.
7.NirschlRP,PettroneFA.TenniselbowThesurgicaltreatment oflateralepicondylitis.JBoneJointSurgAm.
1979;61(6A):832–9.
8.HagbergS.Newsurgicalapproachtolateralepicondylitisof thehumerus.Lancet.1972;1(7747):441–2.
9.StovellPB,BeinfieldMS.Treatmentofresistantlateral epicondylitisoftheelbowbylengtheningoftheextensor carpiradialisbrevistendon.SurgGynecolObstet. 1979;149(4):526–8.
10.CohenMS,RomeoAA.Openandarthroscopicmanagement oflateralepicondylitisintheathlete.HandClin.
2009;25(3):331–8.
11.GoldieI.Epicondylitislateralishumeri(Epicondylalgiaor tenniselbow).Apathogeneticalstudy.ActaChirScandSuppl. 1964;57Suppl3391+.
12.LechO,PiluskiPCF,SeveroAL.Epicondilitelateraldocotovelo. RevBrasOrtop.2003;38(8):421–35.
13.AhmadZ,BrooksR,KangSN,WeaverH,NunneyI,
Tytherleigh-StrongG,etal.Theeffectofplatelet-richplasma onclinicaloutcomesinlateralepicondylitis.Arthroscopy. 2013;29(11):1851–62.
randomizedcontrolledtrialwith2-yearfollow-up.AmJ SportsMed.2011;39(6):1200–8.
16.MiyazakiAN,FregonezeM,SantosPD,SilvaLA,PiresDC,Neto JM,etal.Avaliac¸ãodosresultadosdotratamentoartroscópico daepicondilitelateral.RevBrasOrtop.2010;45(2):136–40. 17.VerhaarJ,WalenkampG,KesterA,VanMamerenH,Vander
LindenT.LateralextensorreleasefortenniselbowA prospectivelong-termfollow-upstudy.JBoneJointSurgAm. 1993;75(7):1034–43.
18.BaumgardSH,SchwartzDR.Percutaneousreleaseofthe epicondylarmusclesforhumeralepicondylitis.AmJSports Med.1982;10(4):233–6.
20.GardnerRC.Tenniselbow:diagnosis,pathologyand treatment:nineseverecasestreatedbyanewreconstructive operation.ClinOrthopRelatRes.1970;72:
248–53.
21.PoschJN,GoldbergVM,LarreyR.Extensorfasciotomyfor tenniselbow:along-termfollow-upstudy.ClinOrthopRelat Res.1978;1978(135):179–82.