www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Role
of
cervical
vestibular
evoked
myogenic
potentials
(cVEMP)
and
auditory
brainstem
response
(ABR)
in
the
evaluation
of
vestibular
schwannoma
夽
Deepa
Aniket
Valame
∗,
Geeta
Bharat
Gore
T.N.MedicalCollege&BYLNairHospital,DepartmentofAudiologyandSpeechTherapy,Mumbai,India
Received19October2015;accepted8April2016 Availableonline28April2016
KEYWORDS
Cervicalvestibular evokedmyogenic potentials; Auditorybrainstem response;
Contralateraleffect; Neurofibromatosis
Abstract
Introduction:Cervicalvestibularevokedmyogenicpotentials(cVEMP)canassesstheintegrity oftheinferiorvestibularnervetherebypromisingtobeausefultoolintheaudiologicaltest batterytodiagnosevestibularschwannoma.
Objective:ToascertaintheutilityofcVEMPindiagnosisofvestibularschwannomain conjunc-tion withthe ABRandto evaluatewhether thesize oflesionhasany effectonthecVEMP measures.
Methods:Case-filesof15knowncasesofvestibularschwannomawhosepuretoneaudiometry, auditorybrainstemresponse(ABR),cVEMPandradiologicalinvestigationfindingswere avail-able,wereincludedinthestudy.Patientswerecategorisedaslargeorsmalltumoursbasedon thesize.Theabsoluteandinter-peaklatenciesofABR,amplitudesofwavesVandI,and inter-aurallatencydifferenceofwaveVofABR;andlatencyofP1andN1ofcVEMPandamplitude ofP1---N1complexwereconsideredinthestudy.
Results:Therewereeightlargeandnine smalltumours.Allthepatientswithlargetumours showedsignificantseverityofhearinglosswhereasonlythreeoutofninepatientswithsmall tumours showed severeto profound deafnessintheaffected ear.The rest showed hearing statusrangingfromnormalhearingsensitivitytomoderatehearingloss.Mostofthepatients withlargetumoursshowedcompleteabsenceofABRintheaffectedearswithnoidentifiable wave-peaks.ABRinsmalltumoursexhibiteddelayedIII---IanddelayedV---Iinterpeaklatency interval(IPL).Four outoffivepatientswith largeunilateral tumoursrevealed contralateral effectsofreducedamplitudeorabsenceofcVEMP.Onthecontrary,sixoutofeightunilateral smalltumoursshowedanormalcVEMPresponseinthecontralateralear.Boththepatientswith NF2inthepresentstudydemonstratedcVEMPabnormalities.
Conclusion:ABRandcVEMP,whenusedincombination,canbeofimmenseuseinidentification ofneuro-otologicconditionssuchasvestibular schwannomaandbilateraltumoursinNF2.In
夽 Pleasecitethisarticleas:ValameDA,GoreGB.Roleofcervicalvestibularevokedmyogenicpotentials(cVEMP)andauditorybrainstem
response(ABR)intheevaluationofvestibularschwannoma.BrazJOtorhinolaryngol.2017;83:324---9.
∗Correspondingauthor.
E-mail:[email protected](D.A.Valame).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.
http://dx.doi.org/10.1016/j.bjorl.2016.04.003
theevaluationofunilateralvestibularschwannoma,abnormalcontralateralfindingsofcVEMP andABRarestronglyindicativeofthetumoursize>2.5cm.Inunilateralseveretoprofound losswhereinABRinpoorerearcannotgiveinformationofsite-of-lesion,cVEMPcanhelpinthe differentiation.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http:// creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE
Potenciaisevocados miogênicos
vestibulares cervicais; Respostaauditiva evocadadotronco cerebral;
Efeitocontralateral; Neurofibromatose
Papeldospotenciaisevocadosmiogênicosvestibularescervicais(cVEMP)epotencial evocadoauditivodetroncoencefálico(PEATE)naavaliac¸ãodoschwannoma
vestibular
Resumo
Introduc¸ão: Ospotenciaisevocadosmiogênicosvestibularescervicais(cVEMP)podemavaliara integridadedonervovestibularinferior,prometendoassimserumaferramentaútilnabateria detestesaudiológicosparaodiagnósticodeschwannomavestibular.
Objetivo: DeterminarautilidadedecVEMPnodiagnósticodeschwannomavestibularem con-juntocomPEATEeavaliarseotamanhodalesãotemqualquerefeitosobreasmedidasdocVEMP. Método: Quinze casos conhecidosde schwannoma vestibular cujosachados de audiometria tonal pura, Potencialevocadoauditivo de troncoencefálico(PEATE), cVEMP einvestigac¸ão radiológicaestavam disponíveis foramincluídosnoestudo.Ospacientesforamclassificados comoportadoresdetumoresgrandesoupequenos.AslatênciasabsolutaseinterpicodePEATE asamplitudesdas ondasV eIeadiferenc¸ade latênciainteraural daondaV daPEATE ea latênciadeP1eN1decVEMPeamplitudedocomplexoP1-N1foramconsideradasnoestudo. Resultados: Havia oito tumores grandes enove pequenos. Todosos pacientescomtumores grandes apresentavam perda auditiva grave enquanto apenas três dos nove pacientes com pequenostumoresapresentaramsurdezgraveaprofundanaorelhaacometida.Orestante apre-sentouaudic¸ãoquevarioudenormalaperdaauditivamoderada.Amaioriadospacientescom tumoresgrandesdemonstrouausênciacompletadePEATEnasorelhasacometidassempicosde ondaidentificáveis.OPEATEemtumorespequenosapresentouIntervalodeLatênciaInterpico (ILI)tardiaIII-IetardiaV-I.Quatroemcadacincopacientescomtumoresgrandesunilaterais revelaramefeitoscontralateraisdeamplitudereduzidaouausênciadecVEMP.Ao contrário, seisdosoitotumorespequenosunilateraisapresentaramrespostadecVEMPnormalnaorelha contralateral.AmbosospacientescomNF2nopresenteestudodemonstraramanormalidades nacVEMP.
Conclusão:PEATEecVEMP,quandoutilizadasemcombinac¸ão,podemserúteisnaidentificac¸ão decondic¸õesneuro-otológicascomoschwannomavestibularetumoresbilateraisemNF2.Na avaliac¸ãodeschwannoma vestibularunilateral,achadoscontralateraisanormaisdecVEMPe PEATEsãofortementeindicativosdetumor>2,5cm.Naperdaunilateralgraveaprofunda,na qual oPEATEnaorelhamaisprejudicadanão forneceinformac¸ões dolocaldalesão,cVEMP podeajudarnadiferenciac¸ão.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http:// creativecommons.org/licenses/by/4.0/).
Introduction
Vestibular schwannomas are benign intracranial tumours
arising from the schwann cells of the vestibulocochlear
nerve.Most of thesetumours arise fromthe inferior
ves-tibular branch and more than90% are unilateral sporadic
tumours while the rest arebilateral schwannomas due to
NeurofibromatosistypeII(NF2).1Thegoldstandardforthe
identificationofthesetumoursisthegadoliniumenhanced
MRI which can identify even small tumours few
millime-tresin size.Theaudiological batterythatwasfoundmost
sensitiveintheidentificationofthesetumoursusingclinical
decision analysis method includes the auditory Brainstem
ResponseAudiometry(ABR)andAcoustic ReflexCombined
(ARC),i.e.acousticreflexthresholdandreflexdecaytests
incombination.2 However,the audiologicalbattery hasits
ownlimitations.ThesensitivityofABRdecreasesasthesize
ofthetumourislessthanonecm.FurtherclickevokedABR
maymissout thetumours arisingfromthelow frequency
fibresofthevestibulocochlearnervetherebydecreasingits
sensitivity.3 Also, the audiological tests are not useful if
Withthe adventofMRI,thus theaudiologicaltest battery
is not deemed veryuseful in the evaluation of vestibular
schwannoma.Onerecentadditiontothearmamentariumof
anaudiologist inthelastdecadeis thecervicalVestibular
EvokedMyogenicResponse(cVEMP).
cVEMPareshortlatencyelectromyogenicresponsesthat
are recorded from contracted sternocleidomastoid (SCM)
muscleinresponsetoveryloudtransientstimuli.Theseare
thoughttoreflectmomentaryinhibitionofthecontraction
ofSCM due toloudsounds and aremediatedby
saccullo-colic pathway.4 The outcome measures of cVEMPi.e. the
latencyofP1andN1waves, amplitudeofP1---N1 complex
andinter-auralamplituderatio(IAR)arethoughttoreflect
thefunctioningofsaccule and/orinferiorbranchof
vesti-bularnervealthoughpresentlythetestcannotdifferentially
diagnosebetweenlesionsofthesetwosites.Astheinferior
vestibularnerveisinvolvedinneurallesionssuchas
vesti-bularschwannoma,cVEMPcanbeausefultoolinthetest
battery.Further,theproposed pathwayof cVEMPinvolves
neural impulses from the inferior vestibular nerve
reach-ing the inferior vestibular nucleus in the brainstem. The
descendingarcissupposedlyviathemedialvestibulospinal
tracts (MVST) that supply the spinal accessory nerve to
theeffector muscle SCM.5 Thuslesions or tumoursof the
lower brainstem can affect the cVEMP pathway either in
itsascendingpath(inferiorvestibularnerve)ordescending
path(MVST).InconjunctionwiththeABRthatreflectsthe
synchronousdischargeofonset-sensitiveneurons fromthe
cochlearnervetotheneuronsinupperbrainstem,cVEMPhas
apromisingroleintheevaluationfordiagnosisofvestibular
schwannoma.
Although the lastdecade has seen a surge of research
papersintheclinicalapplicationofcVEMPindifferent
clin-ical conditions, the role of this test in the test battery
foridentification ofvestibularschwannomais notas
well-studied asthe ABR or immittance testing. Further,if the
size of the vestibular schwannoma has any effect onthe
cVEMPhasnotbeenexplored.Henceclinicalstudiesacross
variousclinics involving measurement of cVEMPin known
casesofvestibularschwannomawillhelpustobetter
under-standwhatwillbetheroleofthisquick,non-invasivetool
thatcanbeperformedonstandardauditoryevoked
poten-tial equipment,in the audio-vestibulardiagnosis of these
lesions.
To thisend, this observationalstudy wasconducted to
ascertain the utility of cVEMP in diagnosis of vestibular
schwannomainconjunctionwiththeABR.Further,
descrip-tivestatisticswasusedtoevaluatewhetherthesizeoflesion
hasanyeffectonthecVEMPmeasures.
Methods
The study wasapproved by theethical committee setup
by the university and methodology was in strict
adher-encetotheapprovedprotocol. Known casesof vestibular
schwannomathathadreportedforaudiologicalevaluation
were tested using the ABR and cVEMP. Fifteen diagnosed
cases of vestibular schwannoma (17 ears) in the period
fromMay 2012toMay2014,whose puretoneaudiometry,
ABR, cVEMP and radiological investigation findings were
available,wereincludedinthestudy.Thirteenpatientshad
unilateral sporadic schwannoma while two were
Neurofi-bromatosis type II (NF2) patients with bilateral tumours.
Patients with conductive pathology were excluded. Each
patient’spuretoneaudiogram(PTA),clickevokedABRand
cVEMPresultsweredocumented.PTAwascarriedoutusing
InteracousticsAC40dualchannelaudiometerwithTDH-39
earphones housed in MX 41-AR cushions. ABR and cVEMP
were recorded using IHS Smart EP (Florida, USA). ABR
wasrecordedusing100Sclickspresented viainsertsand
responseswererecordedfromthenon-invertingelectrode
ontheforehead,invertingelectrodesonthemastoidsand
the palm serving as the ground. cVEMP was monaurally
recordedfromelectrodeplacedovercontractedSCMusing
500Hz tone burst of rarefaction polarity presented at
80dBnHL at a repetition rate of 5/s. The response was
filtered from10 to1000Hzandamplified5000times. Two
runs of two hundred sweeps were recorded. cVEMP was
carried out in sittingposition. Unilateral SCM contraction
was achieved by head rotation to the side contralateral
to acoustic stimulation. Participants were instructed to
bend downtheir heads by 30degrees and then turn their
headcompletelytoonesidetherebymaintainingsustained
contractionofSCM.Shouldermovementswerediscouraged.
Patientsweregivenabreakaftereveryruntoavoidmuscle
fatigue. Two runs were recorded to ensure for intra-test
reliability.
Theabsoluteandinter-peaklatenciesofABR,amplitudes
ofwavesVandIandinter-aurallatencydifferenceofwave
VofABR;andlatencyofP1andN1ofcVEMPandamplitude
ofP1---N1complexwereconsideredinthestudy.
Results
TheutilityofcVEMPindicesinconjunctionwithABRindices
in17earswithvestibularschwannomaisdiscussedto
high-lighttheroleofthistestinthetestbattery.Ofthefifteen
casesreviewed,thirteenhadunilateralsporadicvestibular
schwannomawhiletwohadNeurofibromatosistype2(NF2).
Thelesionwasseenontheleftearin6casesandrightear
in7 caseswhilebilateral lesionswereseenin the2cases
withNF2.Theageofthepatientsrangedfrom19yearsto
68yearswithameanageof43.6years.
Ninetumourswereclassifiedassmallandeightaslarge
basedontheir sizeasestimatedfromMRI scans.Tumours
≥2.5cm were defined as large in this study while those
<2.5cmweredefinedassmall.Thetumoursizevariedfrom
5.4mmto5.0cm.
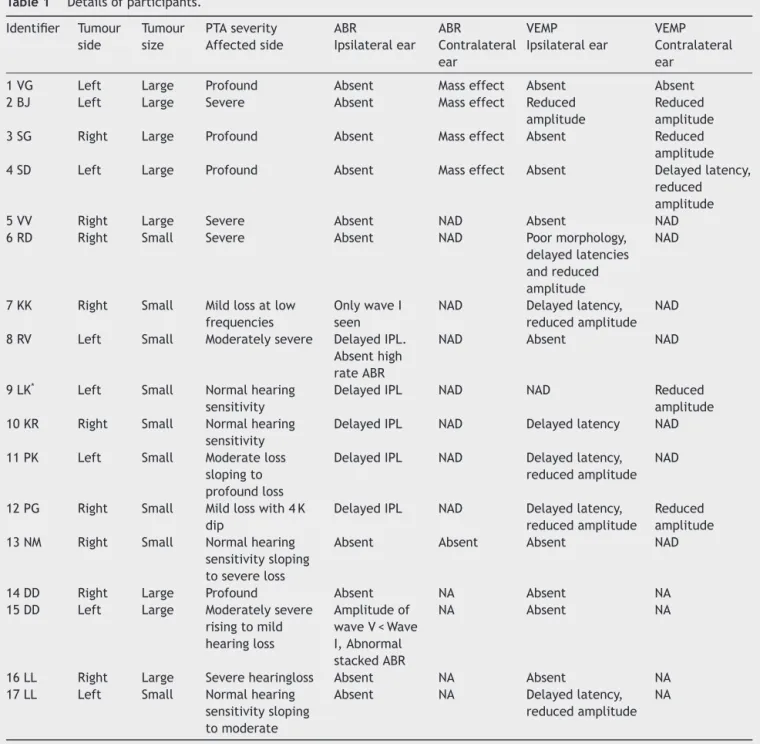
Table1showstheseverityofloss,presence/absenceof
ABR abnormality in ipsilateral and contralateral ear and
presence/absenceof cVEMPabnormality inipsilateraland
contralateralearinthesepatientswithunilateralvestibular
schwannomas.
Theabovedatarevealsthatallthe patientswithlarge
tumours (100%, n=8 ears) showed significant severity of
hearinglosswhereasonlythreeoutof 9(33.33%)patients
with small tumours showed severe to profound deafness
in the affected ear. The rest showed hearing status
ran-ging fromnormal hearing sensitivity to moderate hearing
loss.Thusthesizeofthetumourdoesappeartoaffectthe
severity of hearing loss. This is consistent with the
Table1 Detailsofparticipants.
Identifier Tumour side
Tumour size
PTAseverity Affectedside
ABR
Ipsilateralear ABR
Contralateral ear
VEMP Ipsilateralear
VEMP Contralateral ear
1VG Left Large Profound Absent Masseffect Absent Absent
2BJ Left Large Severe Absent Masseffect Reduced
amplitude
Reduced amplitude
3SG Right Large Profound Absent Masseffect Absent Reduced
amplitude
4SD Left Large Profound Absent Masseffect Absent Delayedlatency,
reduced amplitude
5VV Right Large Severe Absent NAD Absent NAD
6RD Right Small Severe Absent NAD Poormorphology,
delayedlatencies andreduced amplitude
NAD
7KK Right Small Mildlossatlow frequencies
OnlywaveI seen
NAD Delayedlatency, reducedamplitude
NAD
8RV Left Small Moderatelysevere DelayedIPL. Absenthigh rateABR
NAD Absent NAD
9LK* Left Small Normalhearing
sensitivity
DelayedIPL NAD NAD Reduced
amplitude 10KR Right Small Normalhearing
sensitivity
DelayedIPL NAD Delayedlatency NAD
11PK Left Small Moderateloss slopingto profoundloss
DelayedIPL NAD Delayedlatency, reducedamplitude
NAD
12PG Right Small Mildlosswith4K dip
DelayedIPL NAD Delayedlatency, reducedamplitude
Reduced amplitude 13NM Right Small Normalhearing
sensitivitysloping tosevereloss
Absent Absent Absent NAD
14DD Right Large Profound Absent NA Absent NA
15DD Left Large Moderatelysevere risingtomild hearingloss
Amplitudeof waveV<Wave I,Abnormal stackedABR
NA Absent NA
16LL Right Large Severehearingloss Absent NA Absent NA
17LL Left Small Normalhearing sensitivitysloping tomoderate
Absent NA Delayedlatency,
reducedamplitude NA
NA,Notapplicableasthepatientshavebilateraltumours(NF2).
correlationbetweentumoursizeanddeteriorationofpure tonethresholds.6
Most of the patients withlarge tumours (87.5%, n=7)
showedcompleteabsenceofABRintheaffectedearswith
noidentifiablewave-peaks.Theonlyear(DD,leftear)
clas-sifiedtohave a largetumourbut withABR present wasa
tumourofsize2.8×2.3cm,thusitwasborderlinelarge.On
thecontrary,absenceofABRwasnotedonlyin33.33%(n=3)
patients withsmall tumours of which one showed wave I
wasspared.Eggermont,Don&Brackmannalsoreportthat
only fouroftheir forty threepatientswithsmall tumours
showedabsenceofABR.7 ThusabsenceofABR israrebut
possible even in few smalltumours considering that
fac-torslikesiteoftumour,itsconsistencyandvascularitymay
all affect results. The rest of ABRs in small tumours of
thepresent studywerecharacterised bydelayed III---Iand
delayed V---I interpeak latency interval (IPL). Onepatient
showedabsenceofpeakswhenhighstimulusrepetitionrate
wasused.Theseindiceshaveshowntobediagnosticin
iden-tifyingtumoursinthepreviousstudiestoo.6,7
AlllargetumoursaffectedtheABR ofcontralateralear
in terms of reduced amplitude of latter waves, delayed
latencies of latter waves and absence of wave V in one
patient.Musiek andKiebbe8reportedcontralateral
abnor-malitiesofABRinmorethan70%ofpatientswithtumours
>3cm and the most useful indicator was delayed V---III
interpeaklatency interval(IPL).Shihetal.6studiedthirty
thatprolongedV---IIIIPLandwaveVlatencyincontralateral
ear, with prolonged III---I IPL in ipsilateral ear should be
interpreted as a tumour >2cm. They strongly advocated
that when ipsilateral as well as contralateral abnormal
parameters are considered for diagnosis, the predictive
valueofABR inidentificationof tumouraswellasitssize
increases. This is typically attributed to the mass effect
ofthelesionthatpushesorrotatesthebrainstemtowards
the opposite side causing compression of the generators
of thelatter wave peaks of the ABR on thecontralateral
side. However other investigators refute this finding as
largemeningiomaswithsimilarbrainstemshiftdonotlead
toequivalentabnormalityonABR.MusiekandKiebbe8say
that compression of ipsilateral lateral lemniscus nuclei
cause desynchronization of fibres responsible for wave V.
Thecontralateralfibres alsoshowdesynchronizationafter
theirdecussationleadingtocontralateraleffectonABR.
Exceptonepatient(LM)withasmalltumour,allpatients
(88.88%)inthepresentstudyrevealedabnormalityofcVEMP
on the affected side irrespective of the size of tumour
or severity of hearing loss. Seven out of eight ears with
large tumours (87.5%) led tocomplete absenceof cVEMP
waveformwhereasoneshowedseverelydiminished
ampli-tude.ThecVEMPwasabsentintwosmalltumours(22.2%),
showed delayed latency in one patient (11.1%) and both
delayedlatencyandreducedamplitudeinfivesmalltumours
(55.5%). This is in accord with the findings of Murofuschi
et al.9 who reviewed charts of 62 patients with
acous-ticneuromasandreportedabsenceofcVEMPordecreased
amplitudein77%patients.Chenetal.10 alsoreportedthat
eightofhisninepatientswithcerebellopontineangle(CPA)
tumours showed affected cVEMP. They also stated that
beforesurgery,cVEMPtestcanbeusedtopredictthenerve
oforiginandtoformulatethebestsurgicalapproach.After
surgery, thetest can be usedtodefine the natureof the
tumour(compressingorinfiltratingthenerve)anddisclose
theresidualfunctionofthe inferiorvestibularnerve.One
patientinthepresentstudywithasmalltumour(LM)
con-sistentlyshowedarobustwaveformontheaffectedearand
absentresponseintheoppositeear.Thisfindingcannotbe
explained.
Discussion
Oneofthe aimsof thepresent study wastodetermineif
largevestibularschwannomacausedcVEMPtobeabnormal
when the opposite or unaffected ear was tested. As the
descending pathway of cVEMP courses through the lower
brainstem,itis possiblethat largetumours thathave
dis-placed/compressedthebrainstemtotheoppositesidewill
showabnormalitiesintheresponseincontralateralear,as
evident on the ABR. It was observed that four out of 5
patients(80%)withlargeunilateral tumoursrevealed
con-tralateraleareffectsof reducedamplitude or absenceof
cVEMP. On the contrary six out of eight unilateral small
tumours(75%)showedanormalcVEMPresponsewhenthe
contralateralearwastested/stimulated.Onepatient(PG)
showedacontralateraleffectpresentwhereasasmentioned
previously LM showed paradoxical results of absent
con-tralateral and normal ipsilateral cVEMP response (4 ears
withofthetwoNF2patientshavenotbeenconsideredhere
as contralateral effects cannot be estimated in bilateral
tumours).
Thehighproportionoflargetumoursshowingabnormal
responsewhentheoppositeearwastestedcouldbedueto
themass effectofthelesion onthecontralateralinferior
vestibularnucleiorthedescendingMVSTinthebrainstem.
To the best of the researcher’s knowledge there are no
previous reports of this finding. Thusthis study highlights
an important use of the cVEMP in conjunction withABR:
notonlydetect acoustictumoursbutalsotoestimatethe
approximate size based on the findings in the
contralat-eralear.Presenceofbilateralabnormalities onthecVEMP
(absenceof response or reducedamplitude) and bilateral
ABRabnormalities(especiallyprolongedV---IIIIPLorabsent
waveV)incaseofunilateralhearingcomplaintsisstrongly
suggestiveofvestibularschwannoma>2.5cmbasedonthis
study.This needs tobe corroboratedbased onfindings in
largernumberofcases.
Itohetal.reportofaninterestingapplicationofthe
com-bineduseofABRandcVEMPtodifferentiatebetweenupper
brainstemvs.lowerbrainstemlesionsbasedontheirstudy
ofthirteenpatients.11Patientswithupperbrainstemlesions
showedcVEMPsparedbutABRabnormalwhereasthosewith
lowerbrainstemlesionsshowedabnormalitiesonboth the
measures.
cVEMPis especiallyausefultoolindifferential
diagno-sis of site of lesion when the affected ear has a severe
toprofound severity of hearingloss wherein the ABR and
acousticreflextestingarerenderedtobeofnouseasthey
need residual hearing for their diagnostic utility. Absent
ABR in a severe to profound loss leads to confounding
results as the response could be absent either owing to
the retrocochlear lesion or due to severity of cochlear
loss.SincecVEMPdoesnotneedresidualhearingasa
pre-requisite for its elicitation, cVEMP findings in such cases
canbecrucialtoidentificationofretrocochlearpathology.
If a patient with unilateral severe or profound SNHL and
absentABRshows normalcVEMPresponsewecanruleout
the involvement of inferior vestibular nerve which is the
siteofvestibularschwannoma.HoweverifcVEMPisabsent
too, radiologicalinvestigations andmedical diagnosesare
warranted.
NF2
BothpatientswithNF2(DD,LL)showedbilateralvestibular
schwannomawithoneearshowinglargertumourthanthe
other. DD had a 4.8×2.8cm tumour in the right ear and
a2.8×2.3cmtumourin theleftear.Her ABRwasgrossly
abnormalwithnoidentifiable waveformson theright ear
and a near-normal ABR in the leftear with absolute and
inter-peaklatencieswithinnormallimitsbut amplitudeof
wave V<Wave I. She was then taken up for tone-burst
evokedstackedABRintheleftear.Inthisprocedure,a
mod-ified versionof thederived-band procedure given by Don
et al.;ABR waselicited in response totone-burst stimuli
of frequencies 500Hz, 1000Hz, 2000Hz and 4000Hz at
80dBnHL.ThewaveformswerealignedforwavepeakVand
stackedtogetastackedABR.Theamplitudeofthestacked
ABR was0.7Vwhichwassignificantlyreducedcompared
absentintherightearandreducedinamplitudeintheleft
earwithsmallertumour.
LLwasreferredfromanothercentreforABRandcVEMP.
His MRI revealed a large lesion on the left side with a
masseffectontherightside.Ourtesting,however,showed
absenceofcVEMPontherightsideanddelayedlatencywith
reducedamplitudeintheleftear.ABRwasbilaterallyabsent
inthispatient.Thisimmediatelywarnedusaboutthe
prob-ableright-leftconfusionontheMRI.Onfurtherevaluations
it wasconfirmedthat thepatient wasacase of NF2with
bilateraltumours,rightbeinglargerthantheleft.
BoththepatientswithNF2inthepresentstudy
demon-stratedcVEMPabnormalities.Contrarytothis,Wangetal.,12
reportedthatNF2tumoursmorecommonlyoriginatedfrom
the superior vestibular nerve than the inferior vestibular
nerve and infiltrated the cochlear nerve more than the
inferiorvestibularnerve.Onlyoneof theirsevenpatients
demonstratedabnormalcVEMPasopposedto77%of14ears
thatdisplayedabnormalcaloricresponsemediatedby the
superiorvestibularnerve.
Conclusions
ABR and cVEMP, when used in combination, can be of
immenseusein identificationof neuro-otologicconditions
such as vestibular schwannoma and bilateral tumours in
NF2. In the evaluation of unilateral vestibular
schwan-noma, abnormal contralateral findings of cVEMP and ABR
arestronglyindicative ofthetumoursize>2.5cm.In
uni-lateralsevere toprofoundloss wherein ABRin poorerear
cannotgiveinformationofsite-of-lesion,cVEMPcanhelpin
thedifferentiation.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.MartinMB,HirschBE.Imagingofhearingloss.OtolaryngolClin NorthAm.2008;41:157---8.
2.TurnerRG,ShepardNT,FrazerGJ.Clinicalperformanceof audi-ologicalandrelateddiagnostictests.EarHear.1984;5:187---94. 3.Don M, Masuda A, Nelson R, Brackmann D. Successful detectionofsmallacoustictumorsusingthestacked derived-band auditory brain stem response amplitude. Am J Otol. 1997;18:608---21.
4.Colebatch JC, Halmagyi GM, Skuse NF. Myogenic potentials generated bya click-evoked vestibulocollic reflex. J Neurol NeurosurgPsychiatry.1994;7:190---7.
5.AkinFW,MurnaneOD.Vestibular-evokedmyogenicpotentials: preliminaryreport.JAmAcadAudiol.2001;12:445---52. 6.ShihC,TsengFY,YehTH,HsuCJ,ChenYS.Ipsilateraland
con-tralateralacousticbrainstemresponseabnormalitiesinpatients with vestibular schwannoma. Otolaryngol Head Neck Surg. 2009;141:695---700.
7.EggermontJJ,DonM,BrackmannDE.Electrocochleographyand auditorybrainstemelectricresponsesinpatientswithpontine angletumors.AnnOtolRhinolLaryngol.1980;89:1---19. 8.MusiekFE,KiebbeK.Auditorybrainstemresponsewaveiv---v
abnormalities from the ear opposite large cerebellopontine lesions.AmJOtolaryngol.1986;7:253---7.
9.Murofuschi T, Shimizu K, Takegoshi H, ChengPW. Diagnostic valueofprolongedlatenciesinthevestibularevokedmyogenic potential.ArchOtolaryngolHeadNeckSurg.2001;127:1069---72. 10.Cheng WC, Young YH, Tseng HM. Preoperative versus postoperative role of cervical vestibular evoked myogenic potentials in cerebellopontine angle tumour. Laryngoscope. 2002;112:267---71.
11.ItohA,KimYS,YoshiokaK,KanayaM,EnomotoH,HiralwaF, etal.Clinicalstudyofvestibular-evokedmyogenicpotentials and auditorybrainstemresponses inpatientswithbrainstem lesions.ActaOtolaryngol.2001;545:116---9.