BrazJOtorhinolaryngol.2016;82(6):722---736
www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
REVIEW
ARTICLE
Study
of
cochlear
microphonic
potentials
in
auditory
neuropathy
夽
Ilka
do
Amaral
Soares
a,b,∗,
Pedro
de
Lemos
Menezes
b,c,
Aline
Tenório
Lins
Carnaúba
a,
Kelly
Cristina
Lira
de
Andrade
a,
Otávio
Gomes
Lins
d,eaUniversidadeFederaldeSãoPaulo(UNIFESP),CiênciasMédicas,SãoPaulo,SP,Brazil
bUniversidadeEstadualdeCiênciasdaSaúdedeAlagoas,Maceió,AL,Brazil
cUniversidadedeSãoPaulo(USP),SãoPaulo,SP,Brazil
dUniversidadeFederaldeSãoPaulo(UNIFESP),SãoPaulo,SP,Brazil
eUniversidadeFederaldePernambuco(UFPE),Recife,PE,Brazil
Received20August2015;accepted29November2015 Availableonline27April2016
KEYWORDS
Cochlear microphonic;
Cochlearmicrophonic potential;
Hearingloss
Abstract
Introduction:AuditoryNeuropathy/Dyssynchronyisadisordercharacterizedbythepresenceof
OtoacousticEmissionsandCochlearMicrophonicPotentials,anabsenceorseverealterationof BrainstemEvokedAuditoryPotential,auditorythresholdsincompatiblewithspeechthresholds andalteredacousticreflexes.ThestudyoftheCochlearMicrophonicPotentialappearstobe themostimportanttoolforanaccuratediagnosisofthispathology.
Objective:Determine the characteristics of the Cochlear Microphonic in Auditory
Neurop-athy/Dyssynchronyusinganintegrativereview.
Methods:BibliographicsurveyofPubmedandBiremeplatformsandMedLine,LILACSand
Sci-ELOdata banks,withstandardized searchesuptoJuly2014, usingkeywords.Criteria were establishedfortheselectionandassessmentofthescientificstudiessurveyed,consideringthe followingaspects:author,year/place,degreeofrecommendation/levelofscientificevidence, objective,sample,agerange,meanage,tests,resultsandconclusion.
Results:Ofthe1959articlesfound,1914wereexcludedforthetitle,20fortheabstract,9for
thetextofthearticle,2forbeingrepeatedand14wereselectedforthestudy.
Conclusion:ThepresenceoftheCochlearMicrophonicisadeterminingfindinginthe
differ-entialdiagnosisofAuditoryNeuropathy/Dyssynchrony.Theprotocolforthedeterminationof CochlearMicrophonicmustincludetheuseofinsertearphones,reversepolarityandblocking
夽 Pleasecitethisarticleas:SoaresIA,MenezesPL,CarnaúbaAT,deAndradeKC,LinsOG.Studyofcochlearmicrophonicpotentialsin auditoryneuropathy.BrazJOtorhinolaryngol.2016;82:722---36.
∗Correspondingauthor.
E-mail:[email protected](I.A.Soares).
http://dx.doi.org/10.1016/j.bjorl.2015.11.022
thestimulustubetoeliminateelectricalartifactinterference.TheamplitudeoftheCochlear Microphonic inAuditoryNeuropathy/Dyssynchrony shows nosignificantdifferencefrom that ofnormalindividuals.ThedurationoftheCochlearMicrophonicislongerinindividualswith AuditoryNeuropathy/Dyssynchrony.
© 2016 Publishedby Elsevier Editora Ltda. onbehalf of Associac¸˜ao Brasileira de Otorrino-laringologiaeCirurgiaC´ervico-Facial.ThisisanopenaccessarticleundertheCCBYlicense (http://creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE
Microfonismococlear; Potencialmicrofônico coclear;
Perdaauditiva
Estudodomicrofonismococlearnaneuropatiaauditiva
Resumo
Introduc¸ão: ANeuropatia/DessincroniaAuditivaéumadoenc¸acaracterizadapelapresenc¸adas
EmissõesOtoacústicasedoMicrofonismoCoclear,comausênciaougravealterac¸ãodoPotencial EvocadoAuditivodeTroncoEncefálico,limiaresauditivosincompatíveiscomlimiaresvocaise reflexosacústicosalterados.OestudodoMicrofonismoCoclearpareceseraferramentamais importanteparaumdiagnósticoprecisodestapatologia.
Objetivo: Verificar por meio de uma revisão integrativa as características do Microfonismo
CoclearnaNeuropatia/DessincroniaAuditiva.
Método: LevantamentobibliográficonasplataformasPubmedeBiremeenasbasesdedados
MedLine,LILACSeSciELO,combuscaspadronizadasatéjulhode2014,utilizando-se palavras-chave. Para a selec¸ão e avaliac¸ão dos estudos científicos levantados, foram estabelecidos critérios,contemplandoosaspectos:autor,ano/local,grauderecomendac¸ão/nívelde evidên-ciacientífica,objetivo,amostra,faixaetária,médiadeidadeemanos,testes,resultadose conclusão.
Resultados: Dos1959artigosencontrados,1914foramexcluídospelotítulo,20peloresumo,
novepelaleituradoartigo,doiseramrepetidose14foramselecionadosparaoestudo.
Conclusão:Apresenc¸adoMicrofonismoCoclearéumachadodeterminantenodiagnóstico
dife-rencialdaNeuropatia/Dessincroniaauditiva.OprotocoloderegistrodoMicrofonismoCoclear devecontarcomousodefonesdeinserc¸ão,ainversãodapolaridadeeobloqueiodotubodo estímuloparaimpedirainterferênciadeartefatoelétrico.AamplitudedoMicrofonismoCoclear naNeuropatia/Dessincroniaauditivanãoapresentadiferenc¸asignificanteentreaamplitudedo Microfonismo Coclearem ouvintesnormais.A durac¸ãodoMicrofonismo Coclearémaiorem indivíduoscomNeuropatia/Dessincroniaauditiva.
© 2016Publicadopor ElsevierEditora Ltda.em nomede Associac¸˜ao Brasileira de Otorrino-laringologia eCirurgiaC´ervico-Facial.Este ´eumartigo Open Accesssob umalicenc¸a CCBY (http://creativecommons.org/licenses/by/4.0/).
Introduction
The termauditory neuropathy (AN) wasfirstusedin1996 to define a group of individuals withauditory symptoms, whohadincommonnormalcochlearfunctiondespitehaving abnormalcochlear nerve function.Moreover,they experi-enceddifficultyinunderstandingspeechespeciallyinnoisy environments, although in some cases they responded to sound stimuli.1 Today the most common denomination is
auditoryneuropathy/dyssynchrony(AN/AD).
In generalfindingsrevealthe absenceor severe abnor-mality of the Auditory Brainstem Response (ABR) with preservationoftheotoacousticemissions(OAE)and/orthe CochlearMicrophonic (CM), indicating disordered function oftheauditorynervewithnormalfunctionofthecochlear haircells(HC).1---4
It is often difficult to determine exactly the onset of AN/AD, but the disease can occur at all ages.4 Its
prevalence has been estimated at 11% in a group of 109
hearing-impairedchildrenwhofailedthenewbornhearing screening (NHS) and ABR.5 Another study reports a
simi-larprevalenceof8.44%in379childrenevaluatedwithABR alteration.4
The CM is a potential generated from the outer hair cells (OHC) and inner hair cells (IHC) of the cochlea and its absence is consistent with alterations in the function of thesecells.2,6 It is an electrical activity that precedes
thesynapsesoftheHCwiththeauditorynerveand, there-fore,whenrecorded,itappearsbeforewaveIonABRand maintains its latency even when the stimulus intensity is decreased.5
Therearestillnoavailabledata regardingCM parame-tersinindividualswithnormalhearingorwithhearingloss. However,recordingtheCMattractedrenewedinterestafter theidentificationoftheAN/AD,1astheassociationbetween
724 SoaresIAetal. Theliteraturerecommends thattestsof cochlear
func-tion, particularly CM, become part of the NHS (Newborn HearingScreening) protocol in allchildren withabsent or alteredABR,facilitatingthediagnosisofAN/AD.5
The aim of the study is to verify the character-istics of cochlear microphonism in Auditory Neurop-athy/Dyssynchronythroughanintegrativereview.
Methods
Themethodologicalprocesscharacterizedthepresentstudy asan integrativereview,togather datafromstudiesthat helptheunderstandingof thesubjectinasystematicand orderlymanner, thushelpingtoacquirefurtherknowledge onCochlearMicrophoniccharacteristicsinAuditory Neurop-athy/Dyssynchrony.
The integrativereview wascarriedout fromelectronic searchesin Pubmed andBireme platformsand in the fol-lowingdatabases:MedLine,LILACSandSciELO--- Regional. The data search wasstarted and concludedin July 2014. Studies published in English, Spanish or Portuguese were selectedfortheanalysis.Therewasnorestrictionregarding theyearofpublication,i.e.studiespublisheduptoJuly2014 wereanalyzed,andsubsequently,thearticleswereselected accordingtoinclusionandexclusioncriteria.
The search strategy was performed by crossing the descriptors (DeCS and MeSH), as well as the free terms, which are terms not found in MeSH and MeSH, but that arerelevanttothesearch.The descriptorsusedtolocate thestudieswereCochlearMicrophonicandCochlear Micro-phonic Potential and the free terms used were Auditory NeuropathyandAuditoryDyssynchrony.
Search
strategy
The search strategy was directed by a specific question: ‘‘WhatarethecharacteristicsoftheCochlearMicrophonic in Auditory Neuropathy/Dyssynchrony?’’. Aiming to iden-tify the relevant articles with the proposed question, a search strategy was developed, using the descriptors in groups, with at least two keywords. The descriptors used were: Cochlear Microphonic/Auditory Neurop-athy/Auditory Dyssynchrony/Cochlear Microphonic AND
Auditory Neuropathy OR Auditory Dyssynchrony/Cochlear Microphonic Potential/Auditory Neuropathy/Auditory Dyssynchrony/CochlearMicrophonicPotentialANDAuditory NeuropathyORAuditoryDyssynchrony.
Selection
criteria
Inclusioncriteria
Articleswith the following characteristics were included: originalarticle,casereportorliteraturereviewincludingas researchsubjectsindividualsdiagnosedwithauditory neu-ropathy.
Exclusioncriteria
Thearticlesthatdidnotdescribethefindingsofaudiological assessmentin individualswithAN/ADwereexcluded from thisreview.
Study
identification,
selection
and
inclusion
Thestudywasindependentlycarriedoutbytworesearchers andthepointsofconflictwerediscussed atspecific meet-ings. After applying the search strategy containing the defineddescriptors,articleselectionwasperformedinthree stages:
1. Identificationandreadingoftitlesindifferentelectronic databases.Articlesthatclearlydidnotmeetanyofthe inclusioncriteriaofthisstudywereexcluded.
2. Readingofsummariesofthestudiesselectedatthefirst stage.Similarly,weexcludedarticlesthatclearlydidnot meetanyofthepre-establishedinclusioncriteria. 3. All studies that were not excluded in these first two
stageswereread infullfor theselection ofthosethat wouldbeincludedinthisreview.
All studies used met the inclusion criteria defined in thebeginningofthemethodologicalprotocolofthisstudy, aimingtoanswer thequestionthatguidedthisintegrative review.Themaindataofeacharticlewerefullycollected and entered into a Microsoft Office Excel 2011 program database.
Forbetter presentation of the results, it was decided toconsiderthefollowingvariablesoftheselectedarticles: author,year/location, type of study,gradeof recommen-dation/levelofscientificevidence,objective,sample, age range, mean age in years, tests performed, results and conclusion.
As for the level of scientific evidence, the classifica-tion used was that of Oxford Center for Evidence-Based Medicine.8
Results
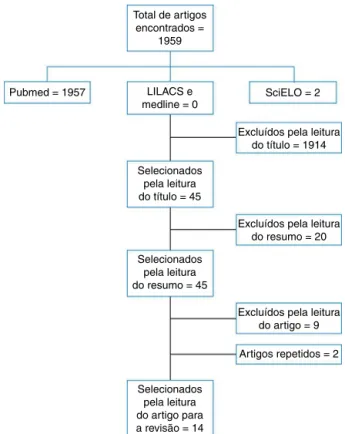
Accordingtotheperformedsearch,1959articleswerefound in theelectronicsearches. Accordingtothe inclusionand exclusion criteria defined in the method and after elim-inating the repeated references found in more than one database,14articleswereselected.
Inthe MedLinedatabase, via PubMed,after employing the keywords and free terms, 1959 articles were found, of which 1913 were excluded after reading the title, 44 abstractswerereadand25articleswereselectedfor read-inginfull.Ofthese25,twowererepeatedarticlesandnine were excluded. In the LILACSand MEDLINE databasesvia Bireme,noarticleswerefoundforthissearch.Twoarticles werefoundintheSciELOdatabase;onewasexcludedafter reading the title and the other was excluded after being readinfull.
The following flow chart (Fig.1) is a synthesis of the articleselectionprocessfortheintegrativereview.
Table1isasynthesiswiththecharacteristicsofthe stud-iesincludedintheintegrativereview.
Discussion
of
cochlear
microphonic
potentials
in
auditory
neuropathy
Table1 Summarywithcharacteristicsofthestudiesincludedinthereview. Author Year/place Studytype Gradeof
recom-mendation/level ofscientific evidence
Objective Sample Arerangein years
Meanagein years
Tests Results Conclusion
Deltenre etal.
1997/Belgium Casestudy C/4 Describeanew formofhearing dysfunction characterizedby absentABR,with evidenceof functionofthe outerhaircells ofthecochlea, thecochlear microphonic potentialand preservedOAE
3 0---4months Not reported
ABR(clipped), OAE,acoustic immittance testing
OAEpresent, absentABRwith thepresenceof CM,residual hearinginone casein Behavioral Audiometry, normal tympanogram and
contralateral acoustic reflexespresent
OAEandABR alonemay indicatean unusual
situation,butthe verificationonly occurswiththe recordingofCM. Recognitionof themicrophonic potentialisolated fromroutine recordings facilitatedbythe useofreverse polaritycanbe valuableforthe
neuro-physiological evaluationof peripheral hearingandthus, itishighly recommended. Santarelli
andArslan
2002/Italy Casestudy C/4 Describethe findingsofthe ECoGin5 patients,one adultandfour children,with absentABRand presenceof DPOAE
5 3monthsto 19years
Not reported
EcogT,ABR clickDPOAEs, acoustic immittance testing, Behavioral Audiometry, Vocal Audiometry
Insomecases EcogTwasthe onlyreliable diagnostictool todetect peripheral damagesuchas brainstem generator dysfunction
726
Soares
IA
et
al.
Table1(Continued)
Author Year/place Studytype Gradeof recom-mendation/level ofscientific evidence
Objective Sample Arerangein years
Meanagein years
Tests Results Conclusion
Rapinand Gravel
2003/USA Literature review
D5 Identifyan adequateterm fordiseasesthat affectthe centralauditory pathwayinthe brainstemand, selectively,in thebrain
Not applicable
Not applicable
Not applicable
Notapplicable Pureauditory neuropathyis rare,inmany cases,boththe 8thnerveand
centralauditory pathwayor,in somecases,CC contributeto atypicalhearing lossandspeech recognition
ThetermANis notadequatefor casesinwhich thepathologyis predominantlyin thebrainstem andshouldbe reservedfor patientswith evidencethatthe diseaseinvolves thespiral ganglioncells andtheiraxons Berlinetal. 2003/USA Literature
review
D5 StudyofAN diagnosisand management
Not applicable
Not applicable
Not applicable
Notapplicable Studies performedin thelast20years showthat althoughthe electroacoustic evaluationcan providegood diagnosis,these responsesare productsofa complex physiological processandare notnecessarily thetrue perception indicators
of
cochlear
microphonic
potentials
in
auditory
neuropathy
Table1(Continued)
Author Year/place Studytype Gradeof recom-mendation/level ofscientific evidence
Objective Sample Arerangein years
Meanagein years
Tests Results Conclusion
Rance 2005/Australia Literature review
D5 Studyingthe mechanismsof AN,typeof disorder,clinical profileof patientsand mainlythe effectsofthe perceptionof AN,whichare quitedifferent fromthose associatedwith SNHL
Not applicable
Not applicable
Not applicable
Otoscopy EcogT,ABR click,DPOAEs, acoustic immittance testing
Theresultsshow thatinall patients, amplitudeand CMthreshold arecritically dependenton theCAP threshold, showingan associationof CMwithboth OHCandIHC
Thepresenceof aCNSdisorder seemstoimprove theCM
728
Soares
IA
et
al.
Table1(Continued)
Author Year/place Studytype Gradeof recom-mendation/level ofscientific evidence
Objective Sample Arerangein years
Meanagein years
Tests Results Conclusion
Santarelli etal.
2006/Italy Observational Cross-sectional
C4 Evaluatethe amplitudeofthe CMandthe hearing thresholdof normalearsand earswithvarying degreesof elevationinthe recordingofthe ActionPotential andcompare withthe corresponding valuesinagroup ofpatientswith AN
522 7monthsto 47years
3.1years Puretoneand vocal audiometry, acoustic immittance testing,OAE andABR
TheCM amplitudewas significantly higherin patientswith CNSdisease thaninthose withnormal hearing.CM responseswere detectedinall auditory patientswith AN,with amplitudesand thresholds similartothose calculatedfor individualswith normalhearing. Thedurationof theCMwas significantly higherinthe groupwithAN
1.CMdetection isnota distinctive characteristicof AN;2.Patients withCNSdisease showedan increasein amplitudeand durationofCM, possiblydueto theefferent system dysfunction; Theduration, highfrequency andamplitudeof theCMwere similarin patientswith normalhearing andAN.Thismay resultfroma variable combinationof thetypeof efferentsystem lesionandlossof OHC
Anastasio etal.
2008/Brazil Casereport D5 Demonstratethe clinical
applicabilityof EcogETinthe differential diagnosisofAN whencompared toABR
1 4years Not applicable
OAE,ABRclick, ABR0.5and 1kHztonepips andimaging test
A4-year-old child,diagnosed withAN underwentthe Ecog-ETwith 2000Hztone burstin rarefactionand condensation polarities
of
cochlear
microphonic
potentials
in
auditory
neuropathy
Table1(Continued)
Author Year/place Studytype Gradeof recom-mendation/level ofscientific evidence
Objective Sample Arerangein years
Meanagein years
Tests Results Conclusion
Ahmmed etal.
2008/United Kingdom
Casereport C4 Studythe diagnostic dilemmaabout thepresenceof CMtogetherwith asignificant increaseinABR thresholdsin infantswhofail atNHS
1 6weeks Not applicable
TOAE,Ecog, ABRbyclick, byBCand Toneburst(500, 1000and 2000Hz)
SNHLdiagnosed throughclinical andfamily history,physical examinationand imagingtests thatshowed enlarged vestibular aqueducts. PresenceofCM inthepresence ofveryhigh thresholdsinthe ABRclickand theobtainingof thresholdsfor andinABRtone pip0.5kHzmay notbeadequate todifferentiate betweenSNHL andother conditions associatedwith AN
730
Soares
IA
et
al.
Table1(Continued)
Author Year/place Studytype Gradeof recom-mendation/level ofscientific evidence
Objective Sample Arerangein years
Meanagein years
Tests Results Conclusion
Riaziand Ferraro
2008/USA Casereports C4 Toevaluate techniquesthat canoptimizethe recordingofCM inhumans. Througha varietyof stimulus parametersand shielding conditionsaimed at inhibit-ing/reducing artifactsthat cancontaminate theCM
11 7children and4adults
Not reported
TOAE,Ecog, ABR,byclick andtoneburst (500,1000and 2000Hz)
Theresults suggestthatitis easierto separatetheCM oftheartifact fromthe stimulususing anelectrodein theauditory canaland toneburst stimuli. Additionally, electromagnetic shieldingand groundingofthe powercables andtheacoustic transducerwere effectivein reducingand/or eliminatingthe stimulusartifact
Theresultsof thisnormative studymayhelp improvethe diagnosisofCM inANandother hearing-related disorders
Talaatetal. 2009/Egypt Prevalence Study
B2B Detectthe prevalenceofAN inchildrenand youngindividuals withsevereto profoundhearing loss
112 6---32months 19months Behavioral audiometryor VisualBoost, ABRbyclick andToneburst (500Hz), acoustic immittance test
15patients werediagnosed accordingtoour diagnostic criteria
of
cochlear
microphonic
potentials
in
auditory
neuropathy
Table1(Continued)
Author Year/place Studytype Gradeof recom-mendation/level ofscientific evidence
Objective Sample Arerangein years
Meanagein years
Tests Results Conclusion
Moetal. 2010/China Observational Cross-sectional
C4 Describethe audiological findingsofAN
48 6---58months Not reported
Behavioral audiometry, DPOAE,ABRby clickand acoustic immittance test
Therewere40 childrenwitha bilateralAN profileand8 unilateralcases; inthe
contralateral earsofthese cases,there were3earswith ABRthresholds thatwerebetter than30dBNHL, whichindicates normalauditory function,and5 withabsentor severelyaltered ABR.In
addition,four childrenwere diagnosedwith AuditoryNerve Disabilitiesafter further
investigation throughinner earmagnetic resonance imaging
732
Soares
IA
et
al.
Table1(Continued)
Author Year/place Studytype Gradeof recom-mendation/level ofscientific evidence
Objective Sample Arerangein years
Meanagein years
Tests Results Conclusion
Shietal. 2012/China Observational Cross-sectional
C4 Investigatethe characteristics andclinical significanceof CMinthe diagnosisofAN ininfantsand children
36 3monthsto9 years
3years Behavioral audiometry, DPOAE,ABRby clickand acoustic immittance testing
Therewasno significant differencein thelengthor amplitudeofCM betweenthe groupwithAN andthegroup withnormal hearing.Butthe amplitudesof theCMwithAN andabsent DPOAEwere significantly lowerthanin individualswith normalhearing
of
cochlear
microphonic
potentials
in
auditory
neuropathy
Table1(Continued)
Author Year/place Studytype Gradeof recom-mendation/level ofscientific evidence
Objective Sample Arerangein years
Meanagein years
Tests Results Conclusion
Liuetal. 2012/China Retrospective cross-sectional cohort
C4 Explorea possible correlation between cochlearnerve impairmentand unilateralAN
85 2---23years Not reported
Puretone audiometry, DPOAE,TOAE, ABRbyclick andacoustic immittance testing
Eightcaseswere diagnosedwith unilateralAN causedby cochlearnerve impairment.7 hadatype‘‘A’’ tympanogram withnormal bilateralOAE; thelastonehad unilateraltype ‘‘B’’,
tympanogram, absentOAEand presentCM, accordingto alterationsin themiddleear. ABRwasabsent inallpatients andneuronal responsesfrom thecochlea werenot disclosedwhen viewedby magnetic resonance imagingofthe internal auditorycanal
Thecochlear nerve
impairmentcan beseenby elec-trophysiological evidenceand maybean importantcause ofunilateralAN. Magnetic resonance imagingofthe internalauditory canalis
734
Soares
IA
et
al.
Table1(Continued)
Author Year/place Studytype Gradeof recom-mendation/level ofscientific evidence
Objective Sample Arerangein years
Meanagein years
Tests Results Conclusion
Penidoand Issac
2013/Brazil Cohortstudy C4 Determinethe prevalenceofAN inindividuals withSNHL
2292 0---95years Not reported
Puretoneand vocal audiometry; acoustic immittance testing;OAE; ABRandCM
1.2%hadAN.Of these,29.6% hadmildSNHL; 55.5%
moderate;7.4% severeand7.5% profound.14.8% wereaged0---20 years;33.4% were21---40 years;44.4% were41---60 yearsand7.4% wereolderthan 60years
Theprevalence ofANwas1.2%in individualswith SNHL
Total de artigos encontrados =
1959
Pubmed = 1957 LILACS e
medline = 0
SciELO = 2
Excluídos pela leitura do título = 1914
Selecionados pela leitura do título = 45
Selecionados pela leitura do resumo = 45
Selecionados pela leitura do artigo para a revisão = 14
Excluídos pela leitura do artigo = 9
Artigos repetidos = 2 Excluídos pela leitura do resumo = 20
Figure 1 Flowchart of articles identified, excluded and includedintheintegrativereview.
MCrecordingthroughtwospecifictests,ABRandtheEcog, usinginvasiveornon-invasivemethods,inadditiontoother teststoassessauditoryfunction.
There was greater investment in research in this area inthelate90s,whenANwasdescribed.1Sincethen,
stud-ieshave sought toexplain thelocationof the lesion,risk factors,prevalence and moreaccuratediagnostic testsin AN.
Regardinglocation,theliteratureindicatesabroad pos-sibility,asthelesion mayoccurinseveralstructuresorin morethanoneatthesametime,suchastheIHC,auditory nervefibers,or intheir synapses.9Anotherstudy suggests
thatthereisanabnormalityintheauditorysystem,located intheVIIInerve,ganglionneurons,intheIHC,betweentheir synapsesoracombinationofthem.1
Riskfactorsareusuallyassociatedtoneonatalproblems such as prematurity, low birth weight, anoxia, hypoxia, hyperbilirubinemia, need for mechanical ventilation and intracranial hemorrhage,10 as well as genetic and
mito-chondrial disorders11 and a family history of hearing
disorders.3,12
Accordingtothestudiesshowninthisreview,the preva-lenceof ANin childrenand young individualswithsevere toprofoundhearinglosswas13.4%9and1.2%inindividuals
withSNHL.13Theprevalencehasalsobeendescribedin
chil-drenwithriskcriteriaforANas1in433(0.23%)andinthe groupofchildrenwithpermanenthearingdeficit,itwas1in 9(11.01%).5Anotherstudyindicatesaprevalenceof8.44%
inagroupof379childrenwithABRalteration.4
There is an agreement in the reviewed literature regardingexaminationfindingsinpatientswithneuropathy, who have present OAE and CM, absent or very altered
ABRandabsent acousticalreflexes.9,10,12---23 Inaudiometry,
thedescribed patternis permanentor fluctuatinghearing lossofvaryingdegrees,withflator ascendingaudiometric configurations,12,17inadditiontodifficultiesinspeech
per-ception,especiallyinthe presenceofnoise.9,10,12,14---17,22,23
TheOAEarepresent,buttheymaydisappearwithtime.16
Theresults of objectiveelectrophysiological testssuch as presenceofTOAE,absentorveryalteredABRandpresence ofCM haveemerged asthefirst diagnostictool for ANin infants.4,24Additionally,patientswithANhaveanalteration
inOAEsuppressioneffectcausedby theefferentauditory pathways.25 TheabsenceofOAE suppressionsuggeststhat
theolivocochlearefferentfunctionisaltered.24
Consideringthe findingsof theauditory functiontests, thepresenceofCMbecomesthedeterminantfindinginthe differentialdiagnosisofAN.16
The protocol used to record the CM by ECoG or ABR shouldalwaysreversethestimuluspolaritiestoconfirmthe recordinginversion and,therefore, confirm CM.13,16,17,19,22
Furthermore,the use of insert earphonesis important to allow the blocking of the plastic tube, indispensable to confirm the biological response, discarding the presence ofelectrical signal artifact.13,17,20 Insert earphonesshould
always be used in the ABR to allow stimulus artifacts to beseparatedfromcochlearpotentials.2Anotherstudyalso
confirmedtheCMresponsebyclosingthestimulustube to prevent the acoustic signal from reaching the ear canal, eliminatingtheartifacts.5
Some studieshave reportedthe useof Ecog asa diag-nostic test for AN. But there are reports suggesting that theTranstympanicElectrocochleography(EcogT)isthegold standard tool to evaluate CM,9,16,17 because Ecog allows
a more detailed analysis of cochlear function in relation toABR.9,17However,promontoryrecordingsareconsidered
moresensitivethantheearcanalandthatresultsinabetter signal-to-noiseratio,astheCMcomesfirstfromthebasal portionsofthecochlea,withanegligiblecontributionofthe apicalregions.7
In one of the reviewed studies, no significant differ-encewasfoundbetweentheamplitudeoftheCMinnormal hearingindividualsandthosewithAN.Themaximum ampli-tudesofCMforalmostallpatientswerearound0.6msafter thestimulus.13 The literaturereports that CMin patients
withAN are especially prominent and persist for several milliseconds after a transient stimulus.2,24 Another study
reportedthat themean amplitudes of the CMwas0.4ms inpatientswithAN,significantlyhigherthaninindividuals withnormalhearing.24
The duration of the CM was longer in the group with ANthan inthe groupwithnormalhearing.13,16 Inpatients
withANintheABR,theCMappearswideandcanexhibita durationofupto4---6ms,andmaybemistakenfor electri-calactivityofthebrainstem;howeveritdoesnotchange withdecreasing intensity, but with the reversed stimulus polarity.25
Ingeneral,theassessedliteratureagreesonthelocation, riskfactorsandclinicalfindingsof ANandreportsthat its differentialdiagnosisis confirmedbased onthe CM recor-ding,becauseevenatanadvancedstateofAN,CMremains present.
736 SoaresIAetal. Microphonism in Auditory Neuropathy/Dyssynchrony. For
thatpurpose,severaltypesofstudieswereselected,which mayseemlikealimitation,butontheotherhand,theymay have differentperspectiveson thesubject, always taking intoaccountthepreviouslydefinedselectioncriteria.
Conclusion
Basedonthestudies includedinthisliteraturereview,we concludethat:
ThepresenceoftheCMisacrucialfindinginthe differen-tialdiagnosisofAN.
The CMrecordingprotocolmustincludetheuseofinsert earphonesandreversepolarityandthestimulusblocking topreventelectricalartifactinterference.
TheamplitudeofCMinANshowednosignificantdifference when compared withthe amplitude of CMin individuals withnormalhearing.
ThedurationofCMislongerinindividualswithAN.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.StarrA,PictonTW,SiningerY,HoodLJ,BerlinCI.Auditory neu-ropathy.Brain.1996;119:741---53.
2.BerlinCI,BordelonJ,StJohnP,WilenskyD,HurleyA,KlukaE, etal.Reversingclickpolaritymayuncoverauditoryneuropathy ininfants.EarHear.1998;19:37---47.
3.Madden C, Rutter M, Hilbert L, Greinwald JH Jr, Choo DI. Clinicalandaudiologicalfeaturesinauditoryneuropathy.Arch OtolaryngolNeckSurg.2002;128:1026---30.
4.FoerstA,BeutnerD,Lang-RothR,HuttenbrinkKB,VonWedelH, WalgerM.Prevalenceofauditoryneuropathy/synaptopathyina populationofchildrenwithprofoundhearingloss.IntJPediatr Otorhinolaryngol.2006;70:1415---22.
5.RanceG,BeerD,Cone-WessonB.Clinicalfindingsforagroupof infantsandyoungchildrenwithauditoryneuropathy.EarHear. 1999;20:238---52.
6.DallosP,Cheatham MA.Production ofcochlearpotentialsby innerandouthaircells.JAcoustSocAm.1976;60:510---2. 7.WithnellRH.Briefreport:thecochlearmicrophonicasan
indi-cationofouterhaircellfunction.EarHear.2001;22:75---7. 8.OxfordCentreforEvidence-basedMedicine(CEBM).Centrefor
EvidenceBasedMedicine.LevelsofEvidence;2009.
9.SantarelliR,ArslanE.Electrocochleographyinauditory neurop-athy.HearRes.2002;170:32---47.
10.RapinI,GravelJ.Auditoryneuropathy:physiologicand patho-logicevidencecallsformorediagnosticspecificity.IntJPediatr Otorhinolaryngol.2003;67:707---28.
11.NgoRYS,Tan HKK,BalakrishnanA,LimSB,LazarooDT. Audi-toryneuropathy/auditorydys-synchronydetectedbyuniversal newborn hearing screening. Int J Pediatr Otorhinolaryngol. 2006;70:1299---306.
12.RanceG.Auditoryneuropathy/dys-synchronyanditsperceptual consequences.TrendsAmplif.2005;9:1---43.
13.ShiW, Ji F,LanL, Liang SC, DingHN, Wang H,et al. Char-acteristics of cochlear microphonics in infants and young childrenwithauditoryneuropathy.ActaOtolaryngol.2012;132: 188---96.
14.DeltenreP,MansbachAL,BozetC,ClercxA,HecoxKE. Audi-toryneuropathy:areportonthreecaseswithearlyonsetsand majorneonatalillnesses.ElectroencephalogrClinNeurophysiol. 1997;104:17---22.
15.Berlin CI, Hood L, Morlet T, Rose K, Brashears S. Auditory neuropathy/dys-synchrony: diagnosis and management. Ment RetardDevDisabilResRev.2003;9:225---31.
16.Santarelli R, Scimemi P, Dal Monte E, Arslan E. Cochlear microphonic potential recorded by transtympanic electro-cochleographyinnormally-hearingandhearing-impairedears. ActaOtorhinolaryngolItal.2006;26:78---95.
17.Anastasio AR, Alvarenga KF, Costa Filho OA. Extratym-panic electrocochleography in the diagnosis of auditory neuropathy/auditory dyssynchrony. Braz J Otorhinolaryngol. 2008;74:132---6.
18.AhmmedA, Brockbank C,Adshead J.Cochlear microphonics in sensorineural hearing loss: lesson from newborn hearing screening.IntJPediatrOtorhinolaryngol.2008;72:1281---5. 19.RiaziM,FerraroJA.Observationsonmastoidversusearcanal
recordedcochlearmicrophonicinnewbornsandadults.JAm AcadAudiol.2008;19:46---55.
20.TalaatHS,KabelAH, SamyH,ElbadryM.Prevalenceof audi-toryneuropathy(AN) amonginfantsand youngchildrenwith severetoprofoundhearingloss.IntJPediatrOtorhinolaryngol. 2009;73:937---9.
21.MoL,YanF,LiuH,HanD,ZhangL. Audiologicalresultsina groupofchildrenwithauditoryneuropathyspectrumdisorder. ORLJOtorhinolaryngolRelatSpec.2010;72:75---9.
22.LiuC,BuX,WuF,XingG.Unilateralauditoryneuropathycaused bycochlearnervedeficiency.IntJOtolaryngol.2012:914986. 23.PenidoRC,IsaacML.Prevalenceofauditoryneuropathy
spec-trum disorder in an auditory health care service. Braz J Otorhinolaryngol.2013;79:429---33.
24.StarrA,SiningerY,NguyenT, MichalewskiHJ,ObaS,Abdala C.Cochlearreceptor(microphonicandsummatingpotentials, otoacousticemissions) and auditory pathway (auditorybrain stem potentials) activity in auditory neuropathy. Ear Hear. 2001;22:91---9.