REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
Official Publication of the Brazilian Society of Anesthesiologywww.sba.com.br
SCIENTIFIC
ARTICLE
Comparison
of
the
effectivity
of
oral
and
intra-articular
administration
of
tenoxicam
in
patients
with
knee
osteoarthritis
Mesut
Erbas
∗,
Tuncer
Simsek,
Hasan
Ali
Kiraz,
Hasan
Sahin,
Huseyin
Toman
DepartmentofAnesthesiologyandReanimation,MedicalFaculty,C¸anakkaleOnsekizMartUniversity,C¸anakkale,Turkey
Received5November2013;accepted17December2013 Availableonline6February2014
KEYWORDS
Osteoarthritis; Tenoxicam; Knee;
Intra-articular administration
Abstract
Backgroundandobjectives: Tenoxicamiswidelyusedinosteoarthritistreatmentandweaimed tocomparetheeffectivityoforalandintra-articularadministrationoftenoxicamin osteoarthri-tistreatment.
Methods:Thisstudywasperformedbetween2011and2012byretrospectivelyanalyzingand comparingthefindingsof60patientswhowereclinicallyandradiologicallydiagnosedwithknee degenerativeosteoarthritisinBünyanstatehospitalpainpoliclinic.60patientsincludedinthe study were dividedinto two groups.The first group(tenoxicam IA,n=30)includedpatient findings ofthosesubjectedtointra-articularinjectionof20mgtenoxicam tothekneeonce aweekforthreeweeksandthesecondgroup(oraltenoxicam,n=30)includedpatientswho wereadministered20mgoraltenoxicamonceadayforthreeweeks.Allpatientswere clini-callyevaluatedpre-treatmentandinthe1stweek,1stmonthand3rdmonthpost-treatment accordingtospecifiedcriteria.
Resultsandconclusions:Twenty twoof60 patientsincludedinthestudy weremaleand38 were female.In bothgroupssignificant improvementswere detectedinalloftheobserved parameters:visualanalogscale,WesternOntarioMcMasterOsteoarthritisIndex(pain,physical activity,kneestiffness)andLequesneindexscoresandintheevaluationsperformedin1stweek, 1stmonthand3rdmonthwithrespecttopre-treatmentvalues.Besides,abettercompliance totreatmentandgastrointestinalsystemtolerabilityintenoxicamIAgroupwasalsoobserved. Intra-articulartenoxicamadministrationcouldbethoughtasanalternativetreatmentmethod inpatientswithkneeosteoarthritiswhocannotuseoraltenoxicamespeciallyduetosystemic gastrointestinalsystemsideeffectsandthosewhohavedifficultiesinadaptingtotreatment. © 2014SociedadeBrasileirade Anestesiologia.Publishedby ElsevierEditoraLtda.Allrights reserved.
∗Correspondingauthor.
E-mail:[email protected](M.Erbas).
0104-0014/$–seefrontmatter©2014SociedadeBrasileiradeAnestesiologia.PublishedbyElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE
Osteoartrite; Tenoxicam; Joelhos; Administrac¸ão intra-articular
Comparac¸ãodaeficáciadetenoxicamadministradoporviaoraleintra-articulara
pacientescomosteoartritedejoelhos
Resumo
Justificativaeobjetivos: Tenoxicaméamplamenteusadonotratamentodaosteoartrite(OA) eonossoobjetivofoicompararaeficáciadetenoxicamadministradoporviaoral(VO)e intra-articular(IA)notratamentodaOA.
Métodos: Esteestudo foiconduzidoentre 2011e2012por meiode análiseretrospectivae comparac¸ãodosresultadosde60pacientesqueforamclínicaeradiologicamentediagnosticados comOAdegenerativadejoelhosnaPoliclínicadeTratamentodaDordoHospitalEstadualde Bünyan.Os60pacientesincluídosnoestudoforamalocadosemdoisgrupos.Oprimeirogrupo (tenoxicamIA, n=30) incluiuresultados de pacientessubmetidos àinjec¸ãonos joelhospor viaIAde20mgdetenoxicamumavezporsemanadurantetrêssemanaseosegundogrupo (tenoxicamVO,n=30)incluiupacientesquereceberam20mgdetenoxicamporVOumavez pordiadurantetrêssemanas.Todosospacientesforamavaliadosclinicamentenafasebasal pré-tratamentoeemumasemana,ummêsetrêsmesespós-tratamento,deacordocomos critériosespecificados.
Resultadoseconclusões: Dos60pacientes,22eramdosexomasculinoe38dosexofeminino. Emambososgrupos,melhoriassignificativasforamdetectadasemtodososparâmetrosdaescala visualanalógica,doíndiceWestern OntarioandMacMaster(Womac ---dor,atividadefísicae rigidezdosjoelhos)edoíndicedeLequesnenasavaliac¸õesfeitasemumasemana,ummêse trêsmesesecomparadasaosvaloresbasais.Alémdisso,umamelhoradesãoaotratamentoe tolerabilidadeaosistemagastrointestinalnogrupotenoxicamIAtambémforamobservadas.A administrac¸ãodetenoxicamIApodeserconsideradacomoummétodoopcionaldetratamento empacientescomOAdejoelhosquenão podemusartenoxicamporVO,especialmentepor causadosefeitoscolateraissobre osistemagastrintestinal,e naquelescomdificuldadesde adaptac¸ãoaotratamento.
©2014SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
Osteoarthritis (OA) is the arthritis form most commonly encountered in the world. OA is primarily defined as a repair process developed against joint degeneration and joint destruction that cause a series of biochemical andmorphologicchangesinjointcapsuleandsynovial mem-brane and against erosion in joint cartilage, osteophytic hypertrophyofbonesinjointedges,subchondralsclerosis.1
OA is especially one of the leading causes of morbidity thataffectslifequalityofgeriatricpatientsnegatively.Pain is the most encountered and the most important symp-tom. OA pain is complicated and complex. Tissues other than cartilage in the joint have a rich nociceptive net. OA treatment should be conducted with pharmacological andnon-pharmacological method.The primaryaim in OA treatment is tostop thepain; mainlyacetaminophenand NSAI drugs are used for this purpose. But the physicians try to develop new treatment alternatives because the abovestatedtreatmentoptionsremaininadequateandside effects develop in the long term.2,3 Analgesics and NSAI
(Nonsteroidalanti-inflammatory) drugsare widely usedin OAtreatment.Butcareshouldbetakeninthe administra-tionofthesedrugsin elderlypatientsduetotheirserious side effects and the weakness of their effectivity.4 They
mustreacha specific concentrationin theblood for anti-inflammatorycharacteristicsofNSAIdrugstoappearandbut theirpotentialsideeffectscausepatientstodecreasethe
dose theyuse and generallyeffective dose concentration cannotbereached. Tenoxicamis widelyusedinOA treat-ment.Furthermoreitisshownthatintra-articularinjection of tenoxicam is commonly usedin OA treatment and has beneficialeffects.5
Withthis study we estimated that IAtenoxicam treat-ment in patients with OA provided a more effective treatmentthanoraltenoxicam(TXO),withlesssideeffects.
Methods
Thisstudywasperformedbyretrospectivelyanalyzingand comparingfindings of 60patients diagnosedclinically and radiologically withknee degenerative OA in Bünyan state hospital between2011 and 2012. Required consents were obtainedfromthepatientsbyexplainingthemthedisease andthetreatmenttobeperformed.ConsentofC¸anakkale 18MartUniversityClinicalResearchEthicsCommitteewas alsoobtained(15.05.2013/11-08;AksuluHA).Dataof50---80 yearsold patientsin ASA I---III groupwere included in the study.
Table1 Demographiccharacteristicsofpatients.
GroupTXIA GroupTXO
Age(year) 65±5.6 66±4.7 Bodymassindex(BMI) 30.9±1.93 30.2±1.31 Durationofillness(month) 16.2 16.9 ASAI/II/III 4/14/12 6/13/11
included in the study. Sixty patients, data of which were usedinthestudy,weredividedintotwogroups.Inthefirst group(n=30)patientswereadministered20mgtenoxicam IA(TXIA)injectiononceaweekforthreeweeks.Inthe sec-ondgroup(n=30),patientsadministeredoraldailydosisof 20mgtenoxicam(TXO)forthreeweeks.Furthermore, phys-icaltreatmentprogramincludingrehabilitation,stretching andaerobicexercisestoincreasejointrangeofmovement was applied to all patients. All patients were clinically evaluated pre-treatment and in the 1st week, 1st month and 3rd month post-treatment according tothe specified criteria.Accordingtothis,sensationofpainwasevaluated withvisualanalogscale (VAS)(0:nopain,10:verysevere pain).Furthermore,painstatus,functionalcapabilitiesand morningstiffness ofpatients wereevaluatedaccording to Western Ontario McMaster Osteoarthritis (WOMAC) index. And,Lequesne indexwasusedtoevaluatepainand func-tionalcapabilities ofpatients.Alsocomplaintsofpatients associatedwithgastrointestinalsystem(GIS)(gastritis, nau-sea,epigastricburning,constipation)duringtreatmentwere definedasGIStolerabilityanddataofcomplianceto treat-mentwererecorded.
Statisticalanalysis
The SPSS software (SPSS 13, Chicago, IL, USA) was used for analysis. Descriptive parameters are presented as mean±standard deviation,median(minimum---maximum). Independentsimple t test wasused for comparingmeans of continuous variables between twogroups. When there were more than two groups, Friedman test was used, Bonferroni correction was used for multiple comparisons (˛*=0.05/6=0.0083),respectively. Ap-valueof <0.05was consideredassignificant.
Results
22 of 60 patients included in the study were male and 38 were female. Demographic characteristics of patients in both groups were shown in Table 1. Significant recov-eries in all the parameterswere detected in both groups inVAS,WOMAC(pain,physicalactivity,kneestiffness)and Lequesne index in 1st week, 1st month and 3rd month when compared with pre-treatment values (Tables 2---4) (p<0.001).
Significant increaseswere detected in all the parame-tersinVAS,WOMAC(pain,physicalactivity,kneestiffness) andLequesneindexinthe3rdmonthevaluationswhen com-paredwiththepost-treatment1stweekvalues(p<0.001). Butitwasobservedthattheseresultsremainedlowerthan pre-treatmentvalues.
Table2 VASin1stweek,1stmonthand3rdmonthwhen comparedwithpre-treatmentvalues.
VAS GroupTXIA GroupTXO
Baseline 8.2±0.61 8.1±0.54 1stweek 2.3±0.49a 2.8±0.48a
1stmonth 3.2±0.40a 3.7±0.44a
3rdmonth 4.1±0.37a 4.8±0.40a
Generalpvalue 0.001 0.001
a Differencescomparedwithbaselinewerestatistically
signif-icant(p<0.001).
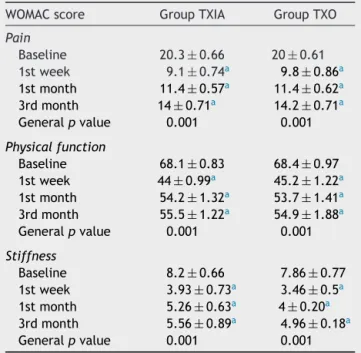
Table3 WOMAC(pain,physicalactivity,kneestiffness)in 1st week, 1stmonth and3rdmonth whencompared with pre-treatmentvalues.
WOMACscore GroupTXIA GroupTXO
Pain
Baseline 20.3±0.66 20±0.61 1stweek 9.1±0.74a 9.8±0.86a
1stmonth 11.4±0.57a 11.4±0.62a
3rdmonth 14±0.71a 14.2
±0.71a
Generalpvalue 0.001 0.001
Physicalfunction
Baseline 68.1±0.83 68.4±0.97 1stweek 44±0.99a 45.2±1.22a
1stmonth 54.2±1.32a 53.7±1.41a
3rdmonth 55.5±1.22a 54.9±1.88a
Generalpvalue 0.001 0.001
Stiffness
Baseline 8.2±0.66 7.86±0.77 1stweek 3.93±0.73a 3.46±0.5a
1stmonth 5.26±0.63a 4±0.20a
3rdmonth 5.56±0.89a 4.96±0.18a
Generalpvalue 0.001 0.001
a Differencescomparedwithbaselinewerestatistically
signif-icant(p<0.001).
GIStolerabilityduringthetreatmentandtreatment con-tinuityareshowninTable5.
Discussion
Significantimprovements weredetected in allthe param-eters in scores of VAS, WOMAC (pain, physical activity,
Table4 Lequesne indexin1stweek,1stmonth and3rd monthwhencomparedwithpre-treatmentvalues.
Lequesneindex GroupTXIA GroupTXO
Baseline 13.73±0.52 13.4±0.72 1stweek 4.33±0.47a 4.63±0.66a
1stmonth 6.80±0.88a 6.53±0.50a
3rdmonth 8.03±0.71a 8.33±0.47a
Generalpvalue 0.001 0.001
a Differencescomparedwithbaselinewerestatistically
Table 5 Patients’ adherence to treatment and GIS tolerance.
GroupTXIA GroupTXO
GISintolerance 2/30 6/30
Treatmentinterruption 3/30 7/30
GIS,gastrointestinalsystem.
kneestiffness)andLequesneindexin1stweek,1stmonth and3rdmonthpost-treatmentinintra-articulartenoxicam administered patients for three weeks and TXO adminis-teredpatientsforthesametimewhencomparedwiththe pre-treatment values. An improvement in all the param-eters in scores of VAS, WOMAC (pain, physical activity, kneestiffness)andLequesneindexwasobservedinthe3rd month post-treatment whencompared withthe 1st week post-treatmentinallthepatients inbothgroups, butthis improvementremainedunderthepre-treatmentvalues.
Although NSAIdrugsareusedcommonly fortheir anal-gesicandanti-inflammatoryeffectsforlowtomildpainin patientswithkneeOA,theirsystemicsideeffectslimittheir long-term use. And therefore in the last few years intra-articular procedures became a current issue and for this purposeintra-articular NSAID, corticosteroids, local anes-thetics or hyaluronicacid preparations were used.6---8 But
becausehyaluronicacidtreatmenthasahighcostand cor-ticosteroidtreatment isnot suitablefor frequentuse, we considerthattenoxicamintra-articularinjectionwithalow costandfewsideeffectscanbeusedinsuitablepatients.
All selective COX-2 inhibitors are contraindicated to thosewithcongestiveheartfailure,ischemicheartdisease orstrokehistory.Itshouldbeusedwithcautioninthosewith cardiovascular risk factor (hypertension, hyperlipidemia, diabetes,cigaretteconsumption).9,10 Forthisreason
mini-mumeffectivedoseshouldbeusedfortheshortestperiod. SelectiveCOX-2inhibitorsareindicatedinthosewithhigh Gastrointestinal risk and withno cardiovascular risk. FDA demandedblackboxwarningtobeputonallNSAIDboxes andalsoawarningstatingthatitcouldcauseanincreasein GIbleedingandCardiovascularproblemstobementioned. Thestudiesregardingthissubjectcontinue.9,10 Mostofthe
patientsinourstudy hadat leastonesystemicdisease;in otherwordstheywereASAII---IIIgrouppatients.
Althoughtherearesomequestionsregardingthesafety of intra-articular injection of NSAI drugs, it is supposed thattenoxicamissafeinthisrespect.Especiallyinpatients subjectedtoarthroscopicsurgeryitwasadministered intra-articularly in order to provide post-operative analgesia. Intra-artical tenoxicam appears to be a safe treatment methodforkneeOA.Butalthoughitisencounteredrarely, riskssuchasbleedingandsepsisshouldbekeptinmind.11---13
It is stated that tenoxicamdoes not affect prostaglandin metabolismincartilagetissueanditseffectsonhyaluronan synthesisvarydependingonthedosage.Anditisindicated that it inhibits glycosaminoglycan loss in the cartilage.14
In the comparative study between tenoxicam and other NASID it was shown that proteoglycan and collagen syn-thesiswas suppressed by tenoxicamand tenoxicam could be helpful in decreasing cartilage catabolism in patients withOA.15Intra-articularuseoftenoxicaminpatientswith
OA becomes increasingly popular due to its ease of use,
chondroprotective and pain revealing characteristic. And NSAIdrugsshouldbeusedwithcautioninoldpatientsdue totheirsystemicside effects.Theyincrease bleedingrisk in patientsusinganticoagulants.GIS shouldbethoroughly examined.11,12Inthestudyweconducted,weobservedthat
direct injection of tenoxicam into knee joint provided a goodalternativeinpatientswhowererequiredtouseNSAID withregardstobothgastrointestinaltolerabilityand treat-mentcontinuity.Furthermore,inastudy40mgsingledose tenoxicamwasadministeredtopatients withpolyarthritis andthenconcentrationofdruginplasmaandsynovial liq-uidweremeasured;half-lifewas42hintheplasmaand45h insynovialliquid.Thus,half-lifeoftenoxicaminplasmaand synovialliquidwasshowntobeparallel.16
In a study patients with OA were divided into three groups: TXO, TXIAand onlyexercisegroup. Patientswere followedfor6monthsandcomparedwithregardsto func-tional capacityandpain, andnodifference wasobserved between3groups.5Andinanotherstudy,singledose
intra-articularinjectionoftenoxicamwasperformedtopatients withkneeOA.Intheevaluationsofpatientsperformedone month later,40% decreasein painand60%increase inthe jointmovementaperturewasobserved.12Ourresultsshow
thatintra-articulartenoxicamtreatmentmaybepreferred to TXO treatment especially for patients that cannot use druginsufficientdosesduetogastrointestinalintolerance. In patients with knee arthritis who cannot use TXO due tosystemic, especially GIS side effectsor thosewho havedifficultyinadaptingtothetreatment,intra-articular tenoxicamtreatmentcanbethoughtasanalternative treat-mentmethod.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.VanelliR, Costa P,Marco S,et al. Efficacyof intra-articular polynucleotidesinthetreatmentofkneeosteoarthritis:a ran-domized,double-blindclinicaltrial.KneeSurgSportsTraumatol Arthrosc.2010;18:901---7.
2.Seed SM,DunicanKC, Lynch AM. Osteoarthritis:a review of treatmentoptions.Geriatrics.2009;64:20---9.
3.ErginS.Painmechanismsinosteoarthritisandcurrent thera-peuticapproaches.TurkJGeriatr.2011;14Suppl.1:63---7.
4.NeustadtDH.Intra-articularinjectionsforosteoarthritisofthe knee.CleveClinJMed.2006;73:897---911.
5.UnluZ, Ay K,Tuzun C.Comparison ofintra-articular tenoxi-camand oraltenoxicamfor painand physicalfunctioning in osteoarthritisoftheknee.ClinRheumatol.2006;25:54---61.
6.BjordalJM,KlovningA,LjunggrenAE,etal.Short-termefficacy of pharmacotherapeutic interventions in osteoarthritic knee pain:ameta-analysisofrandomisedplacebocontrolledtrials. EurJPain.2007;11:125---38.
7.ChanFK,WongVW,SuenBY.Combinationofa cyclo-oxygenase-2 inhibitor and a proton pump inhibitor for prevention of recurrentulcerbleedinginpatientsatveryhighrisk:a double-blind,randomisedtrial.Lancet.2007;369:1621---6.
9.EuropeanMedicineAgencyPublicStatementannounces regula-toryactiononCOX-2inhibitors.Availableathttp://www.emea. eu.int;2011.
10.FDA News, Available at http://www.fda.gov FDA announces series of changes to the class of marketed NSAIDs; 2011.
11.Cook TM, Tuckey JP, Nolan JP. Analgesia after daycase kneearthroscopy:double-blindstudyofintra-articular tenoxi-cam,intra-articular bupivacaineand placebo. Br J Anaesth. 1997;78:163---8.
12.PapathanassiouNP. Intraarticular useoftenoxicamin degen-erative osteoarthritis of the knee joint. J Int Med Res. 1994;22:332---7.
13.ColbertST,CurranE,O’HanlonDM,etal.Intra-articular tenoxi-camimprovespostoperativeanalgesiainkneearthroscopy.Can JAnaesth.1999;46:653---7.
14.ManicourtDH,Druetz-VanEgerenA, HaazenL,et al.Effects oftenoxicamandasprin onthemetabolismofproteoglycans and hyaluronaninnormal and osteoarthritichumanarticular cartilage.BrJPharmacol.1994;113:1113---20.
15.Vignon E, Mathieu P, Louisot P, et al. In vitro effect of nonsteroidalantiinflamatorydrugsonproteoglycanaseand col-lagenase activity in humanosteoarthritic cartilage. Arthritis Rheum.1991;34:1332---5.