RevBrasAnestesiol.2015;65(3):235---236
REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiology www.sba.com.brLETTER
TO
THE
EDITOR
What
is
missing
for
difficult
airway
management
in
the
21st
century
O
que
falta
para
o
manejo
de
via
aérea
difícil
no
século
21
DearEditor,
The difficult airwayalgorithmdeveloped by theAmerican SocietyofAnesthesiologistshassignificantlydecreased mor-bidityandmortalityrelatedtoairway management.1 This
algorithm, widely spread in different countries, provides a rational and effective framework for the anesthesiolo-gist’sperformanceinthisclinicalsetting.Thenewversion ofthisalgorithmhighlightstheuseofsupraglotticdevices andvideolaryngoscopy.2
Difficult airway algorithms have become a mainstayof training programs in anesthesiology and clinical practice. Its effectiveness depends on the proficiency of its users, and trainingin various techniques of airway management ismandatory.Nevertheless,notallusersintraining,oreven experienced physicians, have full competence regarding current algorithms or techniques for difficult airway. In a recent study conducted in the UK, the incidence of complicationsreached1:5000cases.Hypoxemiaisthemain causeforbringingdisastrousconsequences,suchascardiac arrest,braindamage,anddeath.3Unfortunately,thereisno
comparativestudywiththecurrentBrazilianreality.Among thereasonsgivenfortheseoutcomes,theinabilityto pre-dictivelyassesstheairwayandthelack ofpropertraining andessentialequipmentmaybecited.3
Inordertosuccessfullyensurethedifferentairway pre-sentations,thephysicianmusthavepsychomotorskillsthat can only be obtainedthrough trainingand experience. In thisregard,theStanfordUniversityAdvancedAirway Man-agement Program, led byDr. Vladimir Nekhendzy,trained over a thousand Brazilian anesthesiologists in various air-way management techniques. This is the result of joint work with various state societies of anesthesiology since 2007(personalcommunication).Thefactofliving/knowing both (American and Brazilian) realities allows us toissue a challenge to all colleagues in order to reduce this
DMV Difficult mask
ventilation
Laryngeal mask
Success
Fiberoptic intubation Difficult mask
ventilation Cricothyrotomy Failure – revert to
face mask
continue operation under ML
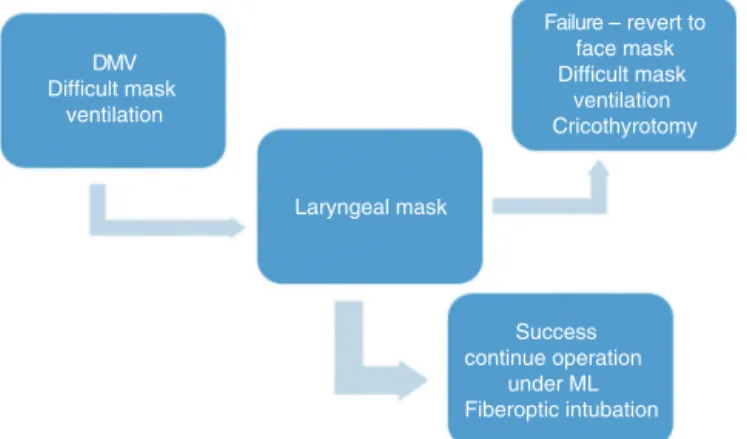
Figure1 Difficultmaskventilation(DMV).
difference,particularlyregardingtheprovisionofessential equipment.
Bougie4andlaryngealmask5 haveshowntobeefficient
in most settings of unpredicted difficult airway manage-ment;however, nowadaysoptical deviceshave been used frequently.Unfortunately,manytrainingprogramshaveno accesstothesedevices.
Weproposeanewsimplifiedalgorithmfordifficultairway management.Ourgoalistoprovideastandardizedapproach for difficult airway management that focuses on institu-tionalissues(e.g.,accessibility,material,andtraining)and canbe widely applied.Based onthe organizational strat-egyrecommendedbySchmidtandEikermann,weproposea modelfordifficultairwaymanagementthatleadsto learn-ingand,oncemastered,tostrongadhesion.Wesimplifythe decisionchartfor threesituations: (1)difficult mask ven-tilation (DMV, Fig. 1); (2) failed direct laryngoscopy (DL) withCormack---Lehane/Yentis6,7 Grade I or II (Fig. 2);and
(3)faileddirectlaryngoscopy(DL)withC---L/YGrade IIIor IV(Fig.3).Inanefforttosimplifythisapproach,while maxi-mizingtheexpertise,ourapproachincludedonlyfiveairway devices:bougie,laryngealmaskairway(whichmayserveto ventorconduitforintubation),videolaryngoscope, broncho-scope,andtheoxygenflowmodulatordevice(Enk®).
Apilotstudyincludingpreceptorsandresidentsof anes-thesiologyat twoacademic institutions wasconducted in Recife, Pernambuco, from September 2012 to September
http://dx.doi.org/10.1016/j.bjane.2013.11.008
236 LETTERTOTHEEDITOR
DL
Success
Failure
C-L /Y 3 and 4
C-L /Y 1 and 2a, 2b
DL failure C-L/Y C-L or 2a, 2b
- Success - Failure (consider as Class 3 and 4)
GEB
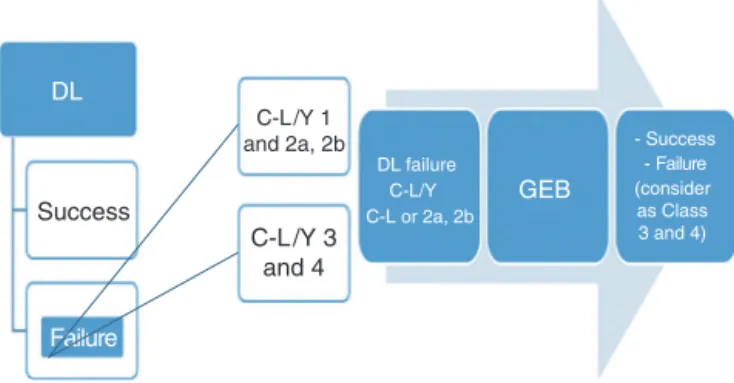
Figure2 Faileddirectlaryngoscopy(DL)withvisionGradesI andII,accordingtoCormack---Lehaneclassificationmodifiedby Yentis(C---L/1and2).
Failed DL C-L /Y 3 or 4
Bronchofibroscopy Videolaryngoscopy Laryngeal mask
Figure3 Faileddirectlaryngoscopy(DL)withvisionGrades
IIIandIV,accordingtoCormack---Lehaneclassificationmodifiedby
Yentis(C---L/Y3and4).
2013.Eachcenter receiveda dayofinstructionaspartof theprogram,whichincludedadidacticmoduleandanother withskillstations.Afterthistraining,therewasalso mon-itoringwithinthesurgicalward.Weknowthattovalidate an algorithm,hundredsor even thousandsof patients are needed.8 This proposal includes tools that are available
toanesthesiologists and has been validated in the litera-ture.We emphasize thateach device hasindications that areunique, which may be advantageous in certain situa-tionsandlimiting inothers. Thereis nosinglesolutionor devicethatallowstheultimatesolutionfordifficultairway management.The lessonlearnedisthat,witharelatively lowinvestmentforhospitaladministration,itispossibleto enableouranesthesiologistsandsurgicalcenters appropri-ately.Weareanalyzingthefeasibilityofconductingalarge prospectivestudyinthefuture.
Initiativessuchasthiswillhelpidentifythespeciallocal needsanditsimplementationfeasibility,andalsoprovidea varietyofsolutionstoproblemsencounteredindailyclinical practiceincommunitieswithlowsocioeconomicstatus.We maynotallowourpatientstocontinuetosufferfromlack ofbasicequipment.Hereisourappeal:ZEROcomplication fromthelackofessentialmaterialinairwaymanagement!
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.MetzerJ,PosnerKL,LamMS,etal.Closedclaim’sanalysis.Best PractResClinAnaesthesiol.2011;25:263---76.
2.ApfelbaumJL,HagbergCA,CaplanRA,etal.,AmericanSocietyof AnesthesiologistsTaskForceonManagementoftheDifficult Air-way.Practiceguidelinesformanagementofthedifficultairway: anupdate reportbytheAmericanSocietyofAnesthesiologists TaskForceonManagementoftheDifficultAirway.Anesthesiology. 2013;118:251---70.
3.CookTM,WoodallN,FrekC,FourthNationalAuditProject.Major complicationsofairwaymanagement intheUK:resultsofthe FourthNationalAuditProjectoftheRoyalCollegeofAnaesthesia andtheDifficultAirwaySociety.PartI:anesthesia.BrJAnaesth. 2011;106:617---31.
4.LattoIP, StaceyM, MecklEnburgh J, etal. Surveyof theuse of the gum elastic bougie in clinical practice. Anaesthesia. 2002;57:379---84.
5.CombesX,LeRouxB,SuenP,etal.Unanticipateddifficultairway inanesthetizedpatientsprospectivevalidationofamanagement algorithm.Anesthesiology.2004;100:1146---50.
6.Schmidt U, Eikermann M. Organizational aspects of difficult airwaymanagementthink globally,actlocally.Anesthesiology. 2011;114:3---6.
7.YentisSM,LeeDJ.Evaluationofanimprovedscoringsystemfor thegradingofdirectlaryngoscopy.Anaesthesia.1998;53:1041---4.
8.Combes X, Jabre P, Margenet A, et al. Unanticipated dif-ficult airway management in the prehospital emergency setting:prospectivevalidationofanalgorithm.Anesthesiology. 2011;114:105---10.
PedroPauloTanakaa,∗,RafaelaPessoab,
RaphaellaFernandesb, JayBrodskyb
aStanfordUniversitySchoolofMedicine,Stanford,
CA,UnitedStates
bHospitaldasClínicas,UniversidadeFederalde
Pernambuco(UFPE),Recife,PE,Brazil
∗Correspondingauthor.
E-mail:ptanaka@stanford.edu(P.P.Tanaka).