REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
Official Publication of the Brazilian Society of Anesthesiologywww.sba.com.br
SCIENTIFIC
ARTICLE
Comparison
of
sevoflurane
concentration
for
insertion
of
proseal
laryngeal
mask
airway
and
tracheal
intubation
in
children
(correlation
with
BIS)
夽
Mahantesh
S.
Mudakanagoudar
∗,
M.C.B.
Santhosh
DepartmentofAnaesthesiology,SDMCollegeofMedicalSciencesandHospital,Karnataka,India
Received20April2014;accepted4July2014
Availableonline27October2014
KEYWORDS
Sevoflurane; Proseallaryngeal maskairway; Endotrachealtube; Bispectralindex monitor
Abstract
Background: Sevofluraneisaninhalationalagentofchoiceinpaediatricanaesthesia.For man-agementofairwaysinchildrenasuitablealternativetoETTisapaediatricproseallaryngeal maskairway(benchmarksecondgenerationSAD).Variousstudieshaveshownthatless sevoflu-raneconcentrationisrequiredforLMAinsertionincomparisontoTI.BISisausefulmonitorof depthofanaesthesia.
Aims:Tocompareconcentrationofsevoflurane(endtidalandMACvalue)requiredforproseal laryngealmaskairwayinsertionandtrachealintubationincorrelationwithBISindex.
Method: Theprospectiverandomisedsingleblindstudywas doneinchildren between2and 9yearsofASAIandIIandtheywererandomlyallocatedtoGroupP(proseallaryngealmask airwayinsertion)andGroup TI(trachealintubation). Nosedativepremedication wasgiven. Inductionwasdonewith8%sevofluraneandthenpredeterminedconcentrationwasmaintained for10min.Airwaywassecuredeitherbyproseallaryngealmaskairwayorendotrachealtube withoutusingmusclerelaxant.Endtidalsevofluraneconcentration,MAC,BIS,andothervital parametersweremonitoredeveryminutetillinsertionofanairwaydevice.Insertionconditions wereobserved.StatisticalanalysiswasdonebyANOVAandStudentsttest.
Results:Difference between ETLMI (2.49±0.44) and ETTI (2.81±0.65) as well as MACLMI
(1.67±0.13) and MACTI (1.77±0.43) was statistically very significant, while BISLMI
(49.05±10.76)andBISTI(41.25±3.25)wassignificant.Insertionconditionswerecomparable
inboththegroups.
夽 StudydoneatDepartmentofAnaesthesiology,MedicalCollegeandSSGHospital,Vadodara,India.
∗Correspondingauthor.
E-mail:[email protected](M.S.Mudakanagoudar).
http://dx.doi.org/10.1016/j.bjane.2014.07.011
Conclusion: Wecanconcludethatinchildrenairwaycanbesecuredsafelywithproseal laryn-gealmaskairwayusinglesssevofluraneconcentrationincomparisontotrachealintubationand thiswassupportedbyBISindex.
© 2014SociedadeBrasileirade Anestesiologia.Publishedby ElsevierEditoraLtda.Allrights reserved.
PALAVRAS-CHAVE
Sevoflurano; Máscaralaríngea proseal;
Tuboendotraqueal; Monitordoíndice bispectral
Comparac¸ãodaconcentrac¸ãodesevofluranoparaainserc¸ãodeMLproseale
intubac¸ãotraquealemcrianc¸as(correlac¸ãocomBIS)
Resumo
Justificativa: Sevofluranoéumagenteinalatóriodeescolhaemanestesiapediátrica.Parao manejodeviasaéreasemcrianc¸as,umaalternativaadequadaparaoTETéumaMLPpediátrica (referênciadesegundagerac¸ãoSAD).Váriosestudosmostraramqueumamenorconcentrac¸ão dosevofluranoénecessáriaparaainserc¸ãodaMLemcomparac¸ãocomaIT.OBISéummonitor útildaprofundidadedaanestesia.
Objetivos: Compararaconcentrac¸ãodesevoflurano(valoresaofinaldaexpirac¸ãoedaCAM) necessáriaparaainserc¸ãodeMLPeintubac¸ãotraquealemcorrelac¸ãocomoBIS.
Método: Estudoprospectivo,randômicoecegoconduzidocomcrianc¸asentre2-9anosdeidade, estadofísicoASAI-II,randomicamentealocadosnosgruposP(inserc¸ãodeMLP)eIT(intubac¸ão traqueal).Pré-medicac¸ãosedativanãofoiadministrada.Ainduc¸ãofoirealizadacomsevoflurano a8%e,emseguida,aconcentrac¸ãopredeterminadafoimantidadurante10min.Aviaaéreafoi garantidaporMLPoutuboendotraqueal,semousoderelaxantemuscular.Aconcentrac¸ãode sevofluranoaofinaldaexpirac¸ão,CAM,BISeoutrosparâmetrosvitaisforammonitoradosacada minutoatéainserc¸ãododispositivorespiratório.Ascondic¸õesdeinserc¸ãoforamobservadas. Aanáliseestatísticafoirealizadacomoteste-tdeStudenteANOVA.
Resultados: As diferenc¸as entre TEIML (2,49±0,44) e TEIT (2,81±0,65), bemcomo CAMIML
(1,67±0,13)eCAMIT(1,77±0,43)foramestatisticamentemuitosignificativas;enquantoBISIML
(49,05±10,76)eBISIT(41,25±3,25)foramsignificativos.Ascondic¸õesdeinserc¸ãoforam
com-paráveisemambososgrupos.
Conclusão:PodermosconcluirqueaMLPemcomparac¸ãocomaintubac¸ãotraquealpodeser segura para aviaaéreade crianc¸as,usandomenos concentrac¸ãodesevoflurano, oquefoi confirmadopeloBIS.
©2014SociedadeBrasileira deAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
Sevoflurane inhalation anaesthesia is considered gold standard in children as it provides fast, safe and accu-rate controlof anaesthesia depthcombined withsecurity of qualityrecovery.LMA iswidely usedfor anaesthesiain children with advantages over tracheal tube in terms of stressresponsetoinsertionandremovalofdeviceandfewer postoperativecomplicationslikecoughingandsorethroat.1 Second generation supraglotticairway (SAD), viz. proseal LMAwithhighersealpressure,hasbecomethebenchmark device.2 Previousstudies haveshownthatless sevoflurane isrequiredforLMAinsertionthanlaryngoscopyandtracheal intubation.1,3,4MorerecentlyBISmonitorisusedasclinical markerofhypnosisandvariousworkershaveusedBISindex tostudythesevofluraneconcentration.5,6Theliteraturesof Medline didnot show anystudy which has correlated the sevoflurane concentration required for LMA insertion and laryngoscopyandtrachealintubationusingBISmonitor.So
wedesignedastudytodetermineandcomparetheminimum sevofluraneconcentrationforinsertionofPLMAandtracheal intubationinpaediatricpatientsincorrelationwithBIS.
Methods
Thiswasarandomised,prospective,comparativestudyand wasapprovedbytheinstitutionalethicalcommitteeanda writteninformedconsentwasobtainedfromthechildren’s parents.
Group P(np=30):Proseal Laryngeal Mask Airway (PLMA)
insertiongroup
GroupTI(nti=30):Trachealintubationgroup
After thorough preanaesthetic checkup, written and informedconsentwasobtainedfromparentsandNBMstatus ofchildwasconfirmed.Intravenousglycopyrrolate20g/kg
wasgiven 20min before induction. No sedative premedi-cationwasgiven.
Compactairwaymoduleofanaesthesiamachinewasused tomeasuresevofluraneconcentration(endtidalandMAC) andothervitalparameters.FormeasurementofBISindex, adultdisposablebiosensorstripswereattached.Itconsists of 4 gel electrodes, the proximal lead wasplaced above thenasionandthedistalleadwasplacedmidwaybetween tragusoftheearandoutercanthusoftheeye.
Baselineparameterslikepulserate,bloodpressure, oxy-gensaturation,respiratoryrate,EtCO2andBISwerenoted.
Anaesthesia was conducted in conventional manner by ananaesthesiologistwhowasblindedforBISvalue aswell asendtidalsevofluraneconcentration.Generalanaesthesia wasinducedwithinhalationofsevoflurane8%with(50:50) O2+N2OusingJacksonReescircuitforchildrenbelow20kg
andBain’scircuitforchildrenabove20kg.Variousstudies have shown that PLMA insertion requires less concentra-tionofsevofluraneincomparisontotrachealintubationand hencewestartedwithpredeterminedconcentrationof2% ingroupPwhile2.5%ingroupTI.Afterthelossofeyelash reflex,anaesthesiawasmaintainedwiththepredetermined endtidalsevofluraneconcentrationfor10min1,3,5(Table1) toallowadequate timefor sevofluranepartialpressureto achieveequilibriuminalveoliandbrain.IPPVwasgivenif depthsofrespirationdecreaseandendtidalCO2morethan
45mmHg.Attheendof10mintheattemptwasmadeeither toinsertPLMAortrachealtubewithoutusingmuscle relax-ant.According to the weight of the child, size of airway devicewasselected.PLMAwasinsertedusingindexfinger technique.ProperplacementofthePLMAandtrachealtube wasconfirmedwithbilateralequalairentryandsquarewave capnography.
If the attempt failed to secure airway the end tidal sevofluranewasincreasedby0.5%andanother10minwas allowedtoelapsebeforethenextattempt.Ifthis second attemptalsofailed,itwasdecidedfornofurtherattempts tobemadebutproceduretobecompletedbyusing conven-tionalmethodofintubationusingmusclerelaxantandthis childwasexcludedfromthestudy.
The conditions during insertion and intubation were evaluatedandgraded asexcellent,satisfactory and poor.
Table 1 Predetermined concentration of sevoflurane in relationwithage.
Wtinkg Predeterminedendtidal
sevofluraneconcentration
GroupP GroupTI
9---10 2% 2.5%
10---15 2.5% 3%
>20 3% 3.5%
Number ofattempts in each patientwasalsonoteddown alongwithinsertionconditions.
The sevoflurane concentration and BIS values were recorded by an observerfrom induction at an interval of 1min tilltheairwayis securedeither byPLMAor tracheal tube.
Vitalparameters(heartrate,bloodpressure,SPO2)and
anycomplicationslikelaryngospasm,bronchospasmduring insertionofairwaygadgetwererecordedbytheobserver.
Thestudyendedonceairwaygadgetwassecured. Anaesthesia wasmaintainedwithO2+N2O (50:50)with
sevoflurane in conventional manner without using mus-cle relaxant by the same clinician who inserted PLMA or intubated.Patientsweremonitoredthroughoutthe periop-erativeperiodtilltheirstayinthepostanaesthesiacareunit (PACU).
Statisticalanalysis
As ourpilotstudy waswithnoprevious informationbeing availableregardingexpectedmeansorstandarddeviations, apre-studypowercalculationwasnotpossible.Thenumber ofparticipantswasbasedonafeasibleconveniencesample andwasthereforearbitrarilydecided.Theprimaryoutcome wastocompare sevofluraneconcentrationfor insertionof prosealLMAandtrachealintubationinchildren.Secondary outcomes were to compare haemodynamic changes and complications during insertion of airway gadgets. Statis-tical testing of ordinal data (ratio of male and female, age of the patient, weight of the patients, and type of surgery)wasdoneusingFisher’sexacttest.Theremaining variables were analysed for statistical significance using two tailed unpaired t test. The results are presented as mean±standard deviation (SD), number (%) of cases. A
p-valueof<0.05wasconsideredsignificant.
Results
Demographic datalikeage, weight,ASA werecomparable inboththegroupsasshowninTable2.Malepreponderance wasseeninboththegroupsbecauseofselectionofsurgery. Durationofsurgerywasshortandcomparableinboth the groups.
Induction time (time to loss of eye lash reflex) was comparableinboththegroups.PLMAwasinsertedinsingle attemptinallthecases.IngroupTItrachealintubationwas
Table2 Demographicdata.
GroupP GroupTI p-Value
Age(yrs) 5.65±3.10 4.6±1.46 >0.05
Weight(kg) 14.40±4.96 11.65±1.76 >0.05
Gender
Male 19 18 >0.05
Female 1 2 >0.05
ASAgrade
I 18(90%) 17(85%) >0.05
Table3 Endtidalsevofluraneconcentrationatvariousphasesofinductionandinsertion.
Stages GroupP GroupTI p-Value
Induction 6.35±1.06 5±1.45 >0.05
Afterpredeterminedconcentration
0min 3.82±1.41 3.97±1.31 >0.05
1min 2.71±0.47 2.87±0.67 >0.05
2min 2.53±0.43 2.81±0.65 <0.01
3min 2.47±0.45 2.83±0.65 <0.01
4min 2.46±0.46 2.81±0.65 <0.01
5min 2.43±0.45 2.82±0.64 <0.01
6min 2.47±0.44 2.82±0.64 <0.01
7min 2.47±0.45 2.82±0.4 <0.01
8min 2.46±0.47 2.81±0.64 <0.01
9min 2.47±0.44 2.81±0.64 <0.01
10min(insertion) 2.49±0.44 2.81±0.65 <0.01
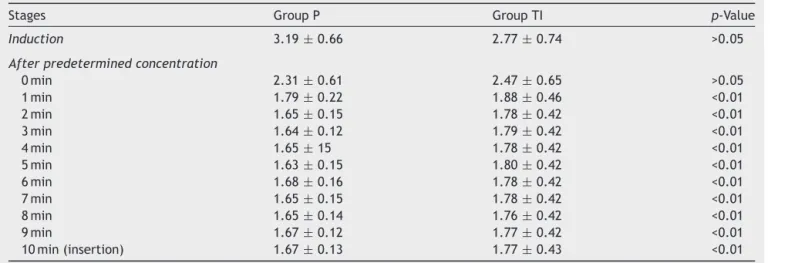
Table4 MACofsevofluraneatvariousphasesofinductionandinsertion.
Stages GroupP GroupTI p-Value
Induction 3.19±0.66 2.77±0.74 >0.05
Afterpredeterminedconcentration
0min 2.31±0.61 2.47±0.65 >0.05
1min 1.79±0.22 1.88±0.46 <0.01
2min 1.65±0.15 1.78±0.42 <0.01
3min 1.64±0.12 1.79±0.42 <0.01
4min 1.65±15 1.78±0.42 <0.01
5min 1.63±0.15 1.80±0.42 <0.01
6min 1.68±0.16 1.78±0.42 <0.01
7min 1.65±0.15 1.78±0.42 <0.01
8min 1.65±0.14 1.76±0.42 <0.01
9min 1.67±0.12 1.77±0.42 <0.01
10min(insertion) 1.67±0.13 1.77±0.43 <0.01
doneatfirstattemptin85%ofthecasesandinremaining 15%secondattemptwasrequired.However,thedifference wasstatisticallyinsignificant(p>0.05).
End tidalsevoflurane concentrationwascomparablein both the groups at the time of induction (Table 3). The difference in two groups was not significant for first two minutes but it started becoming significant from end of twominutesonwardstilltheinsertionofairwaydevice.At thetimeofinsertion/intubationETLMI was2.49±0.44 and
ETTI was 2.81±0.65 andthus thedifference was
statisti-callyverysignificant.SimilarlyMACLMI was1.67±0.13and
MACTIwas1.77±0.43andthusthedifferencewas
statisti-callyverysignificant(Table4).BISwascomparableinboth the groups upto8min after induction but therewas sta-tisticallysignificant differencebetween twogroups at the timeof insertion of airway device, viz.in group Pit was 49.05±10.76andingroupTIitwas41.25±3.25(p<0.05) (Table5).
Insertion conditions were comparable in both the groups andgrading. Vitalparameterslikepulse,meanBP,
respiratoryrate,SpO2,EtN2OandEtCO2werecomparable
inboththegroupsthroughouttheobservationperiod.
Discussion
Table5 BISvalueatvariousphasesofinductionandinsertion.
Stages GroupP GroupTI p-Value
Preinduction 94.35±2.50 93.60±2.80 >0.05
Induction 81.05±10.69 81.75±7.95 >0.05
Afterpredeterminedconcentration
0min 38.80±17.53 35.50±12.71 >0.05
1min 40.11±16.25 35.40±11.62 >0.05
2min 43±14.61 40.75±7.59 >0.05
3min 41.75±14.06 45.30±8.63 >0.05
4min 40.45±14.75 44.40±6.41 >0.05
5min 45.21±14.14 43.85±6.49 >0.05
6min 46.47±13.53 43.10±6.79 >0.05
7min 47.89±12.6 43.15±5.03 >0.05
8min 47.37±12.02 42.75±5.64 >0.05
9min 48.63±11.07 41.95±5.93 <0.05
10min(insertion) 49.05±10.76 41.25±3.25 <0.05
study is that we included BIS index as clinical marker of hypnosisforthecomparison.5,8
Comparing sevoflurane concentration at the time of insertion of airway device significant difference was observedinendtidalsevofluraneconcentrationaswell as MACvalue.Endtidalsevofluraneconcentrationatinsertion ofPLMA,i.e.ETLMI 2.49±0.44waslowerincomparisonto
ETTI2.81±0.65.MACLMI 1.67±0.13wasalsolowerin
com-parisontoMACTI1.77±0.43.Ourfindingsaresimilartoother
studies.1,3,4
BIS value in group P during insertion was 49±10.76 whereasinTIgroupitwas41.25±3.25andthedifference wasstatisticallysignificant.Ourfindingsareinconsonance withotherstudies.6
Thus less sevoflurane is required for PLMAinsertion in comparisontoTI. This wassupportedby BISvalue, which washigherindicatinglesserdepthofanaesthesiaforPLMA insertion.
In ourstudy insertionconditionsfor PLMA andTIwere comparable.OurfindingsaresameasthoseofAantaaetal.1 andPateletal.9
Thus we concluded that in children, airway can be securedsafelyandeffectivelywithPLMAusingless sevoflu-rane concentration in comparison to tracheal intubation whichwassupported byBISindex.Thus,PLMAcanbethe airwayofchoiceforprocedureswherethereisnoneedof deeplevelofanaesthesia.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.AantaaR,TakalaR,MuittariP.SevofluraneEC50andEC95values forlaryngealmaskinsertionandtrachealintubationinchildren. BrJAnaesth.2001;86:213---6.
2.RameshS,Jayanthi R.Supraglotticairwaydevicesinchildren. IndJAnaesth.2011;55:476---82.
3.TaguchiM,WatanabeS,AsakuraN,etal.Endtidalsevoflurane concentrationforlaryngealmaskinsertionandfortracheal intu-bationinchildren.Anesthesiology.1994;81:628---31.
4.Inomata S, WatanabeS, Tagucchi M,et al. End tidal sevoflu-rane concentration for tracheal intubation and minimum alveolar concentration in paediatric patients. Anesthesiology. 1994;80:93---6.
5.DenmanWT,SwansonEL,RosowD,etal.Paediatricsevaluation ofthebispectralindexmonitorandcorrelationofBISwithend tidalsevofluraneconcentrationininfantsandchildren.Anaesth Analg.2000;90:872---7.
6.McCann ME, Bacsik J, Davidson B, et al. The correlation of bispectralindexwithendtidalconcentrationandhaemodynamic parameters in pre-schoolers. Paediatr Anaesth. 2002;12: 519---25.
7.Patki A. Laryngeal mask airway vs the endotracheal tube in paediatric airway management: a meta-analysis of prospec-tive randomised controlled trials. Ind J Anaesth. 2011;55: 537---41.
8.Wappler F, Frings DP, Scholz J, et al. Inhalational induction ofanaesthesiawith8% sevoflurane inchildren: conditionsfor endotrachealintubation and side effects.Eur JAnaesthesiol. 2003;20:548---54.