M évisùz d û Soc ieda de B rasileira de M ed icin a T ropical 24(2): 97-99,, abr-jun, 1991
SPECIFIC TREATMENT OF HEPATOSPLENIC
SCHISTOSOMIASIS CAN INCREASE T-LYMPHOCYTE
REACTIVITY
Maria Imaculada Muniz-Junqueira, José Tavares-Neto, Meire Ataide, Aluizio Prata and Car los Eduardo Tost a
I t h a s b e e n r e c o g n i z e d t h a t Schistosoma mansoni in f e c tio n c a u s e s d e p r e s s i o n o f T - c e ll r e s p o n s i v e n e s s . I n t h i s s t u d y w e h a v e e v a l u a t e d w h e t h e r i m m u n o d e p r e s s i o n a s s o c i a t e d to s c h i s t o s o m i a s i s c o u l d b e r e v e r t e d b y s p e c if i c tr e a tm e n t. T - c e l l i m m u n e r e s p o n s e w a s a s s e s s e d b y
m e a n s o f i n t r a d e r m a l t e s t s u s in g r e c a l l a n t i g e n s in a g r o u p o f 2 2 p a t i e n t s w ith h e p a t o s p l e n ic s c h i s t o s o m i a s i s , o n e y e a r a f t e r t r e a t m e n t w i th o x a m n i q u i n e a n d c o m p a r e d w i th a g r o u p o f
u n t r e a t e d h e p a t o s p l e n i c p a t i e n t s . O n l y 2 7 % o f t r e a t e d p a t i e n t s p r e s e n t e d c o m p l e t e a n e r g y t o a l l t e s t e d a n tig e n s , in m a r k e d c o n t r a s t to 8 0 % u n r e s p o n s iv e n e s s s h o w e d b y h e p a to s p le n ic p a t i e n t s w ith o u t
t r e a tm e n t . A l t h o u g h m o s t o f th e t r e a t e d i n d i v i d u a l s s h o w e d s o m e r e s p o n s e to th e t e s t e d a n tig e n s , in s o m e i n d i v i d u a l s t h i s u n r e s p o n s i v e n e s s s t i l l p e r s i s t e d a f t e r tr e a tm e n t. A n e r g y w a s n o t f o u n d in a n y
n o r m a l i n d i v i d u a l o f t h e c o n t r o l g r o u p . I t w a s c o n c l u d e d t h a t Schistosoma mansoni in f e c te d p a t i e n t s m a y r e c o v e r t h e i r n o r m a l im m u n e r e s p o n s i v e n e s s a f t e r th e e l i m i n a t i o n o f th e w o r m b y t r e a t m e n t
K e y - w o r d s : I m m u n o d e p r e s s i o n . S c h i s t o s o m i a s i s . O x a m n i q u in e .
It is well established that infection by S c h is to s o m a m a n s o n i results in a depressed function of T- lymphocytes^ 6. This immunodepression may be both specific4 9 or unrelated to the antigens of schistosoma wormiO 11 18. The non-specific immunodepression may represent a serious constraint to the elimination of
intracellular pathogens in these patients13.
T-lymphocyte immunodepression in patients with schistosomiasis has been related to the worm burden18 and can be induced by the administration of worm membrane preparation to non-infected mice16.
It is therefore possible that T-lymphocyte immunodepression to unrelated antigens in S c h is to
-ioma-infected patients may be reverted by the elimination of the worm by means of specific therapy.
This work aimed to evaluate in v iv o T-lympho cyte response to unrelated antigens in patients with hepatosplenic schistosomiasis after the elimination of the worm by specific therapy.
Núcleo de Medicina Tropical e Nutrição e Laboratório de Imunologia Celular, Faculdade de Ciências da Saúde, Uni versidade de Brasilia, Brasília, DF.
Faculdade, de Medicina do Triângulo Mineiro, Uberaba, MG.
Grants: CNPq (Proc. 40.1041/PIDE VI and 40.1868/87).
Address for correspondence: Dr.“ Maria Imãculada Muniz- Junqueira, Laboratório de Imunologia, Departamento de Patologia/FCS/UnB. 70910 Brasília, DF, Brasil.
R ecebido para publicação em 2 2 /0 1 /9 1 .
MATERIAL AND METHODS
The ethical rules of the Helsinki Declaration12 were strictiy followed throughout this investigation.
Twenty two patients of both sexes and 35±14 years old with hepatosplenic schistosomiasis were studied. Most of them (55%) were Caucasians. All patients had been previously treated with a single oral dose of 15 mg/kg of oxamniquine.
The diagnosis of schistosomiasis was previously established on clinical and parasitological grounds. Eggs of S c h is to s o m a m a n s o n i were detected in faeces by the Kato-Katz method14. Parasitological assessment of cure was performed after treatment, by the absence of S. m a n s o n i eggs in at least three examination of the faeces. The clinical criteria for the diagnosis of hepatosplenic schistosomiasis were those described by Prata1’ . Physical examination showed no signs of clinical decompensation or nutritional imbalance. Another three patients, not belonging to the previous group and who had been previously sple- nectomized, were also treated with oxamniquine and submitted to the tests. They also did not show any S. m a n so n i- e g g s in faeces.
The positive control group was formed by five female, 21+8 years old patients with hepatosplenic schistosomiasis. All of them were passing S. m a n so n
i-eggs in faeces. Ten healthy individuals, of both sexes, 26±5 years old, 70% of them Caucasians, were considered as the negative control group.
T-lymphocyte function was evaluated by intra dermal tests, using the recall antigens candidin, PPD, streptokinase-streptodomase, trichophytin and vacci nia virus (Allergofar). The later was exclusively used in those individuals showing a scar of smallpox vaccine. One tenth of ml of antigen solution was intradermally injected in the undersurface of the left forearm. Induration was read 48 hours later,
M un iz-J u n q u eira M I, T avares-N etô J, A ta íd e M , P ra ta A , T osta CE. Specific treatm ent o f hepatosplenic sc histo so m ia sis can increase T-lym p ho cy te reactivity. R evista da Soc iedade B rasileira de M ed icina T ropical 24: 97-99, abr-jun, 1991
considered as positive when the largest diameter was equal or higher than 5 mm2^.
The results were statistically analysed by the Chi-square test and Fisher’s exact test
RESULTS
Only six out of 22 schistosomiasis patients without S. m a n s o n i eggs in faeces (27%) showed a complete unresponsiveness to all applied intradermal antigens, while 4 out of 5 patients still passing eggs showed anergy. This difference was statistically signi ficant (p .< 0.05). However, both groups of schistoso miasis individuals showed a higher frequency of anergic tests, when compared to those of the normal control group, where no anergic individual was found (Table 1).
Table 1 - R e s p o n s e o f i n d i v i d u a l s w ith a c t i v e h e p a t o s p l e n ic s c h i s t o s o m i a s i s ( H S ) , o f p r e v i o u s l y t r e a t e d
H S p a t i e n t s a n d o f n o r m a l i n d i v i d u a l s to r e c a l l a n t i g e n s b y i n t r a d e r m a l te s ts .
Groups N Anergy to all applied antigens
number %
Normal 10 0/10 0
Active HS 5 4/5* 80
Treated HS 22 6/22*/** 27
* Significantly different from normal group (p<0.05). Fisher’s Exact Test
** Significantly different from active HS group(p<0.05). Chi-square test
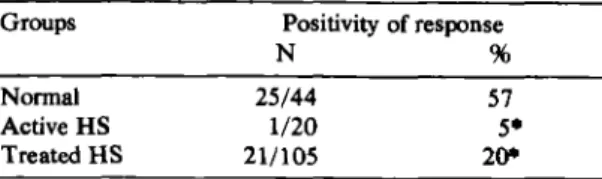
Twenty one out of the 105 intradermal tests applied in the schistosomiasis group without worm were positive (20%), whereas only one test out of 20 (5%) showed positivity in the group presenting worms. However, both groups showed a significantly decre ased number of positive responses when compared with those of normal individuals (57%) (Table 2).
Table 2 - P o s i t i v i t y o f t h e r e s p o n s e to r e c a l l a n t i g e n s b y i n t r a d e r m a l t e s t s o f p a t i e n t s w ith a c t i v e h e p a t o s
p l e n i c ( H S ) s c h i s t o s o m i a s i s , o f p r e v i o u s l y t r e a t e d H S p a t i e n t s a n d n o r m a l i n d i v i d u a l s .
Groups Positivity of response
N %
Normal 25/44 57
Active HS 1/20 5*
Treated HS 21/105 20*
* Significantly different from normal group (p- 0.05 ). Chi-square Test
None of the three splenectomized patients showed anergy and six out of the 15 tests applied (40%) showed positivity.
DISCUSSION
S c h is to s o m a m a n s o n i-infected patients may present T-lymphocyte-dependent immunodépression
9 8
and this could make difficult the elimination of intra cellular pathogens as observed in prolonged septi- caemic salmonellosis associated with schistosomia sis22. The immunodepression is related to the worm burden. Thus, it can be postulated that the elimination of S . m a n s o n i by means of specific therapy would help recovering normal immune responsiveness.
Our data showed that hepatosplenic individuals, considered to be cured by chemotherapy, presented a lower degree of T-cell immunodepression than those who were actively passing 5. m a n s o n i eggs in faeces. In support to our data are the observations of Abdel- Salam etal1 and Barsoum et al^ who showed increased in vitro proliferative responses of lymphocytes to mitogens or antigens, after specific treatment of S c h is to s o m a -in fe c te d patients. It has also been demonstra ted in mice infected with S. m a n s o n i21 or S. h a e m a t o b iu m15 an increased reactivity of lymphocytes after treatment with praziquantel.
Our results also indicated that the recovery of T- cell reactivity was not complete in some treated individuals. Although the reasons for that are not known, it is possible to speculate that it could be related to the degree of previous involvement of the immune system due either to the duration of the infection, the worm burden or the peculiar response of each individual. In fact, Tawfik et al21 have showed in mice that the duration of infection prior to treatment was a determining factor in the subsequent expression of immunoreactivity. Butterworth et al^ have also showed in S . m a n s o n i-infected patients that the resis tance to reinfection after specific therapy depended on the duration of previous infection.
The low frequency of individuals with T-lym- phocyte immunodepression amongst treated patients points to the possibility that factors related to the presence of S. m a n s o n i may play a causal role. In fact, it has been showed that injections of worm membrane preparation induces immunodepression in normal mice16 and, in patients, this immunodepression is related to the worm burden18. However, other factors can also be implicated in the development of this immunodepression, since the elimination of the worm is not enough to completely revert immunodepression. It is possible that factors related to the alterations of the structure and functions of the liver and spleen during the infection, which can persist after treatment2 8 may play a role in this immunodepression. In fact, our limitated observation of three patients previously splenectomized and treated with oxaminiquine sho wed that none of them presented with anergy to all antigens, and the number of positive responses to intradermal tests was similar to that of the normal individuals. Besides, it has been showed that immu nodepression is related to the spleen size17.
M u n iz-J u n q u eira M I, T avares-N eto J, A ta íd e M , P rata A , T osta C E . Specific treatm ent ofh ep a to sp le n ic sc h isto so m ia tís c a n increase T-lym pho cyte reactivity.: R ev ista da Sociedade B rasileira de M ed icina Tropical 24: 97-99, abr-jun. 1991
RESUMO
T e m s i d o o b s e r v a d o q u e in f e c ç ã o p o r Schistosomu mansonip o d e c a u s a r i m u n o d e p r e s s ã o c e lu la r . N e s t e t r a b a lh o f o i a v a l i a d o s e a im u n o d e p r e s s ã o a s s o c i a d a à e s q u i s t o s s o m o s e p o d e s e r r e v e r t i d a p e l o t r a t a m e n t o e s p e c ific o . A r e s p o s ta i m u n e c e l u l a r f o i d e t e r m i n a d a a t r a v é s d e t e s t e s c u t â n e o s d e h i p e r s e n s i b i l i d a d e r e t a r d a d a e m 2 2 p a c i e n t e s c o m a f o r m a h e p a t o e s p lê n i c a d a e s q u i s t o s s o m o s e u m a n o a p ó s t r a t a m e n t o c o m o x a m n i q u i n e e c o m p a r a d o c o m a q u e la o b s e r v a d a e m u m g r u p o d e p a c i e n t e s h e p a t o e s p lê n i c o s n ã o tr a t a d o s . S o m e n t e 2 7 % d e s t e s p a c i e n t e s a p r e s e n t a r a m a l e r g ia a t o d o s o s a n t í g e n o s t e s ta d o s , e m c o n t r a s t e c o m 8 0 % d e i n d i v í d u o s a n ê r g i c o s o b s e r v a d o s e n t r e a q u e l e s n ã o t r a t a d o s . E m b o r a a m a i o r i a d o s i n d i v í d u o s t r a t a d o s te n h a m o s t r a d o a l g u m g r a u d e r e s p o s t a a o s a n t í g e n o s t e s ta d o s , a l g u n s i n d i v í d u o s p e r m a n e c e r a m a n ê r g i c o s a p ó s o t r a t a m e n to e s p e c íf ic o . A n e r g i a a t o d o s o s a n t í g e n o s a p l i c a d o s n ã o f o i o b s e r v a d a e m n e n h u m d o s i n d i v í d u o s n o r m a is . N o s s o s d a d o s i n d i c a m q u e p a c i e n t e s e s q u i s t o s s o m ó t i c o s p o d e m r e c u p e r a r s u a r e a t i v i d a d e i m u n e a p ó s a e li m in a ç ã o
d o v e r m e p e l o t r a t a m e n t o e s p e c ífic o .
P a l a v r a s - c h a v e s : I m u n o d e p r e s s ã o . E s q u i s t o s s o m o se . O x a m n iq u in e .
ACKNOWLEDGEMENTS
The authors gratefiilly acknowledge the assis tance of Rodolfo Gomes de Oliveira and Joaquim Cândido de Lima during field work.
REFERENCES
1. Abdel-Salam E, Higashi GI, Kamal KA, Ishaac S. Cell- mediated immune assay in children with S c h i s t o s o m a h a e m a to b i u m infection and the effect of niridazole therapy. Transactions of the Royal Society of Tropical Medicine and Hygiene 75: 207-214, 1981.
2. Andrade ZA, Grimaud JA. Evolution of the schisto somal hepatic lesions in mice after curative chemothe rapy. American Journal of Pathology 124:59-65,1986. 3. Andrade ZA, Warren KS. Mild prolonged schistoso miasis in mice: alterations in host response with time and the development of portal fibrosis. Transactions of the Royal Society of Tropical Medicine and Hygiene 5 8:53- 57, 1964.
4. Barsoum IS, Gamil FM, Al-Khafif MA, Ramzy RM, El Alamy MA, Colley DG. Immune responses and immu- noregulation in relation to human schistosomiasis in Egypt I. Effect of treatment on in v it r o cellular respon siveness. The American Journal of Tropical Medicine and Hygiene 31: 1181-1187, 1982.
5. Bina JC, Prata A. Regressão da hepatotosplenomegalia
pelo tratamento especifico da esquistossomose. Revista da Sociedade Brasileira de Medicina Tropical 16: 213- 218, 1983.
6. Boros DL, Pelley RP, Warren KS. Spontaneous modu lation of granulomatous hypersensitivity in schistoso miasis mansoni. Journal of Immunology 114: 1437- 1441, 1975.
7. Butterworth AE, Capron M, Cordingley JS, Dalton PR, Dunne DW, Kariuki HC, Kimani G, KoechD, Mugam- bi M. Ouma JH, Prentice MA, Richardson BA, Arap Siongok TK, Sturrock RF, Taylor DW. Immunity after
treatment of human schistosomiasis mansoni. II. Identi fication of resistant individuals, and analysis of their immune responses. Transactions of the Royal Society of Tropical Medicine and Hygiene 79: 393-408, 1985. 8. Cheever AW, Deb S. Persistence of hepatic fibrosis and
tissue eggs following treatment of S c h i s t o s o m a j a p o n i -c u m in f e -c t e d m i-c e . T h e A m e r i -c a n J o u r n a l o f T r o p i -c a l M e d i c i n e a n d H y g i e n e 4 0 : 6 2 0 - 6 2 8 , 1 9 8 9 .
9 . C o l l e y D G , T o d d C W , L e w i s F A , G o o d g a m e R W . I m m u n e r e s p o n s e s d u r in g h u m a n s c h i s t o s o m i a s i s m a n s o n i. V I I n v itr o nonspecific suppression of phyto hemagglutinin responsiveness induced by exposure to certain schistosomal preparations. Journal of Immuno logy 122: 1447-1453, 1979.
10. Cottrell BJ, Humber D, Sturrock RF, Seitz H, Rees P. Non-specific cell mediated immunity in patients infected with S c h i s t o s o m a m a n s o n i in Kenya. Transactions of the Royal Society of Tropical Medicine and Hygiene 76: 234-237, 1982.
11. Coutinho AD, Antunes MTA, Domingues ALC. Es tudo da imunidade humoral e celular na doença hepática esquistossomótica. Revista do Instituto de Medicina Tropical de São Paulo 24: 282-291, 1982.
12. Gutteridge F. Human experimentation and medical ethics international guidelines for biomedical research involving human subjects. World Health Organization Chronicle 35: 212-215, 1981.
13. Hahn H, Kauftnann SHE. The role of cell-mediated immunity in bacterial infections. Reviews of Infectious Diseases 3: 1221-1250, 1981.
14. Katz N, Chaves A, Pellegrino J. A simple device for quantitative stool thick-smear technique in schistoso miasis mansoni. Revista do Instituto de Medicina Tro pical de São Paulo 14: 397-400, 1972.
15. Kumada M, Hosaka Y, Kawabata M, Asahi H, KatoK, Kobayakawa T, Hayashi S. Recovery from immunesu- pression in mice infected with S c h i s t o s o m a j a p o n i c u m by treatment of praziquantel. Japanese Journal of Me dical Science and Biology 40: 89-93, 1987.
16. Mota-Santos TA, Tavares CAP, Gazzinelli G, Pelle grino J. Immunosuppression mediated by adult worms in chronic schistosomiasis mansoni. The American Journal of Tropical Medicine and Hygiene 26: 727-731, 1977. 17. Muniz-Junqueira MI. Resposta imune e atividade de
macrófagos para S a l m o n e l l a na esquistossomose man soni. Tese de Mestrado, Universidade de Brasilia, Bra silia, 1987.
18. Muniz-Junqueira MI, Tosta CE, Prata A. T cell-depen dent immunodepression in v iv o in S c h i s t o s o m a m a n -sow'-infected patients. Revista da Sociedade Brasileira de Medicina Tropical 23: 27-31, 1990.
19. Prata A. Como caracteriza a forma hepato-esplênica da esquistossomose? In : II Simpósio sobre Esquistosso mose, Salvador p. 179, 1970.
20. Rosen FS, Wedgwood RJ, Eibl M. Primary immuno deficiency diseases. Clinical Immunology and Immu- nopathology 40: 166-196, 1986.
21. Tawfik AF, Carter CE, Colley DG. Effects of anti- schistosomal chemotherapy on immune responses, pro tection and immunity. I Changes in cellular and humoral responses. The American Journal of Tropical Medicine and Hygiene 35: 100-109, 1986.
22. Teixeira RS. Associação de infecção por S . m a n s o n i e bacteremia prolongada por enterobactérias. In: As pectos peculiares da infecção por S . m a n s o n i. CEDRE, Universidade Federal da Bahia p. 35-102, 1984.