www.rpped.com.br
REVISTA
PAULISTA
DE
PEDIATRIA
ORIGINAL
ARTICLE
Respiratory
muscle
strength
test:
is
it
realistic
in
young
children?
João
Paulo
Heinzmann-Filho,
Márcio
Vinícius
Fagundes
Donadio
∗CentroInfant,InstitutodePesquisasBiomédicas,PontifíciaUniversidadeCatólicadoRioGrandedoSul(PUCRS),PortoAlegre, RS,Brazil
Received1September2014;accepted18January2015 Availableonline27June2015
KEYWORDS Respiratoryfunction tests;
Musclestrength; Respiratorymuscles; Feasibilitystudies
Abstract
Objective: Todeterminethesuccessrateofthemanovacuometrytestinchildrenbetween4
and12yearsofage.
Methods: Cross-sectionalstudyinvolvingchildrenandadolescentsfrom4to12yearsofage,
enrolledinthreebasiceducationschools.Allsubjectshadtheanthropometricandrespiratory
musclestrength(maximuminspiratorypressureandmaximumexpiratorypressure)data
mea-sured.Studentswhoseparentsdidnotauthorizeparticipationorwhodidnotwanttoundergo
thetestwereexcluded.Thetestwasconsideredsuccessfulwhenthesubjectreached
accept-ability(noairleaks)andreproducibility(variation<10%betweenthetwo majormaneuvers)
criteriaestablishedbyguidelines.Failurewasdefinedwhensubjectsdidnotmeettheabove
criteria.Datawereexpressedasmeanandstandarddeviationandthecategoricalvariablesin
absoluteandrelativefrequency.Thecomparisonbetweenproportionswasperformedusingthe
chi-squaretest.
Results: Weincluded196childrenandadolescents,meanageof8.4±2.5years,53.1%female.
Thesuccessrateofthemanovacuometrytestinchildrenandadolescentsevaluatedwas92.3%.
Whencomparingthedifferencesbetweenthesuccessratesofpreschoolchildrenwiththose
childrenandadolescentsofschoolage,therewasasignificantlylowersuccessrateinthe
pre-school(85.1%)groupcomparedtotheschoolgroup(94.6%)(p=0.032).However,nosignificant
differences(p=0.575)werefoundwhengendercomparisonswereperformed.
Conclusions: Themanovacuometrytestshowedahighsuccessrateinbothpreschoolandschool
populationassessed.Furthermore,therateofsuccessappearstoberelatedtoaging.
© 2015Sociedadede Pediatria de S˜ao Paulo. Published by Elsevier Editora Ltda.All rights
reserved.
DOIoforiginalarticle:http://dx.doi.org/10.1016/j.rpped.2015.01.008
∗Correspondingauthor.
E-mail:[email protected](M.V.F.Donadio).
PALAVRAS-CHAVE Testesdefunc¸ão pulmonar; Forc¸amuscular; Músculos respiratórios; Estudosde viabilidade
Testedeforc¸amuscularventilatória:éviávelemcrianc¸asjovens?
Resumo
Objetivo: Determinarataxadesucessodotestedemanovacuometriaemcrianc¸asdequatro
a12anos.
Métodos: Estudotransversalqueincluiucrianc¸aseadolescentesdequatroa12anos,
matricu-ladasemtrêsescolasdaredebásicadeensino.Todososparticipantesfizeramamensurac¸ãodas
medidasantropométricas,seguidasdotestedemanovacuometria(pressãoinspiratóriamáxima
epressãoexpiratóriamáxima).Escolares cujosresponsáveisnão autorizaramaparticipac¸ão
e aquelesque nãoquiseram fazeroteste foramexcluídos.Oteste foiconsiderado sucesso
quandoo sujeitoavaliado atingia oscritérios de aceitabilidade(ausênciade escapeaéreo)
ereprodutibilidade(variac¸ão<10%entreasduasmaioresmanobras)estabelecidospelas
dire-trizes.Oinsucessofoidefinidocomonãopreenchimentodoscritériosdescritosacima.Osdados
foramexpressosemmédiaedesviopadrãoeemfrequênciaabsolutaerelativa.Acomparac¸ão
entreasproporc¸õesfoifeitapormeiodotestedequi-quadrado.
Resultados: Foramincluídas196crianc¸aseadolescentes,comidademédiade8,4±2,5anos,
53,1%dosexofeminino.Ataxadesucessodotestedemanovacuometriaem crianc¸ase
ado-lescentesavaliadosfoide92,3%.Quandocomparadasasdiferenc¸asentreastaxasdesucesso
de crianc¸asnafaixa etáriapré-escolarcomcrianc¸as eadolescentesnafaixaetáriaescolar,
observou-seumataxadesucesso significativamentemenornogrupopré-escolar(85,1%),em
comparac¸ãocomogrupoescolar(94,6%)(p=0,032).Noentanto,nãohouvediferenc¸a
significa-tiva(p=0,575)quandoanalisadasdiferenc¸asentresexos.
Conclusões: Otestedemanovacuometriaapresentouumaelevadataxadesucessonapopulac¸ão
pré-escolareescolaravaliada.Alémdisso,ataxadesucessopareceestarrelacionadacomo
aumentodaidade.
© 2015Sociedadede Pediatriade S˜ao Paulo. Publicado porElsevier Editora Ltda.Todosos
direitosreservados.
Introduction
Althoughrespiratorydiseases andotherclinical conditions inthepediatricpopulationaresomeofthemaincausesof morbidityandmortalityinchildhood,1,2manyofthemhave
not often been evaluatedby objectivemeasures in clini-calpractice.Thereareseveralreasonsforthisinchildren, mainlythefactthatmanytestsarenotstandardized.3Itis
difficultforthesubjectstounderstandandcooperate,there islowreproducibility,andalsolackofinformationon cer-tainmethodsamonghealthcareprofessionals,aspartofthe evaluationofmanylungconditionsanddiseases.3
In this sense, lung function tests are important tools usedtoevaluatetherespiratorysystem.Theysupply objec-tivemeasurestohelpdiagnoseandmanagevariousclinical conditions.3Among these,therespiratory musclestrength
testisasimple,non-invasiveresource,easytoapply,andis usedtoevaluatethemaximumstaticrespiratorypressures, which reflect respiratory muscle strength.4 It consists of
twomeasures:onedirectedatevaluatinginspiratory mus-cle strength throughmaximum inspiratorypressure (MIP), the other to investigate the expiratory muscle strength throughmaximum expiratory pressure (MEP).4,5 It is
com-monlyusedtodeterminerespiratorymuscleweaknessand toquantifytheseverityofcertaindiseases.4,6Inthe
pedi-atricagerange,itcanhelpinthemanagementandfollow-up of neuromusculardiseases, lung disorderssuch asasthma and cystic fibrosis, and it is also used in rehabilitation programs.4,7
In clinical practice, respiratory muscle weakness can beassociatedwithhypercapnia, withrecurrent infections and inefficient coughing, predisposing to the develop-ment of respiratory failure and the onset of more severemorbidities.8,9 Therefore, inthe lasttwodecades,
studies10---12havebeenperformedtogeneratereference
val-ues for maximum static respiratory pressures in healthy childrenandadolescents,inordertomakegreater useof theminclinicalpractice,duetothepossibilityof normal-izingandinterpreting theserespiratoryfindings.Recently, normalityvalues were published for healthy preschoolers andschoolchildren,10 showing that this evaluationcan be
performedeveninyoungindividuals.Theabsenceof normal-ityvaluesinsmallerchildrenhasbeenascribedmainlytothe technicaldifficultyandthechildren’slackofunderstanding whilethe test isbeingperformed,13,14 demonstratingthat
theagefactormaybethemainlimitationtoevaluatingand usingrespiratorymusclestrengthinthispopulationgroup. However,thereisasyetnoevidenceshowinghowthe suc-cessratesoftherespiratorymusclestrengthtestbehavein differentagegroups.
patientsunderdifferentsituationsandconditionsinclinical practice.
Method
This is a cross-sectional, observational study with chil-drenandadolescentsaged4---12yearswhowereregularly enrolledat threebasic educationschools (two publicand oneprivate) in Porto Alegre, state of Rio Grande do Sul, during 2011 and 2012. First, all the children and adoles-cents were invited to participate in the study, and they receiveda letterofinvitation,togetherwiththefreeand informedconsentform.Aftertheparentsand/orguardians hadsignedandauthorizedit,theywereinvitedfor anthro-pometricmeasurements,followedbytherespiratorymuscle strengthtest (manovacuometry) at their ownschool. Stu-dentswhoseparentsand/orguardiansdidnotauthorizethe subjects’participationinthestudy,andschoolchildrenwho did not want toundergo the test on the day when eval-uation was performed were not included. The study was approvedby theResearchEthicsCommitteeofthe Pontif-ícia Universidade Católica doRio Grande doSul (PUCRS), underregistration number 11/05503. The anthropometric evaluationwasperformedbymeasuringweightandheight intriplicate, or until twoidenticalvalues wereobtained. Weight was obtained with the individuals in the ortho-staticposition,wearingaminimumamountofclothesand noshoes,usingdigital scales (G-Tech, Glass1 FW, Riode Janeiro,Brazil)previouslycalibratedwitha100gprecision. Then,heightwasobtained,withtheparticipantsbarefoot andfeetinaparallelposition,anklesjoinedtogether,arms extended along thebody, andthe head ina neutral posi-tion.Theheightwasobtainedusingaportablestadiometer (AlturaExata,TBW,SãoPaulo,Brazil)witha1mmprecision. Respiratorymusclestrengthwasevaluatedalwaysbythe sameevaluator(physiotherapist),whopresentedoverayear ofpreviousexperienceperformingthetestandwhowasalso trainedandsupervisedbytheprincipalinvestigatorofthe study.Thetestwasevaluatedusingapreviouslycalibrated digital manovacuometer(MVD300, Globalmed, Porto Ale-gre, Brazil) witha variationof −300 to+300cmH2O. The instrument wasconnected to a silicone tube, coupled to an isolatingfilterand toaconnector withan inner diam-eter of approximately 2.5cm, which was connected to a mouthpiece.Theflattish,semi-rigidmouthpiecehadan ori-fice,withadiameterofapproximately2mmtopreventan increaseinintra-oralpressuregeneratedbythecontraction oftheoralcavitymuscles.4Beforemeasuringtherespiratory
pressures,thetechniciandemonstratedandgavedetailed guidanceregardingthemaneuverstobeperformed.
First, MIP was measured from the residual volume, followedbyMEP fromthetotallungcapacity.4 While
per-formingthelattermeasurement,theindividualsweretold topositiontheirhandsonthecheekstokeepairfrom accu-mulatingonthesidesoftheoralcavity.15Themeasurements
were performed with a nasal clip, in a seated position, withthetorso erect at a positionof 90◦ tothe hip.Both
measurementswere performed withmaximum efforts, at approximately1-min intervalsbetweenthemeasures,and sustainedforatleastonesecond.16Aminimumofthreeand
amaximumofninemeasureswereusedforeachtest.13The
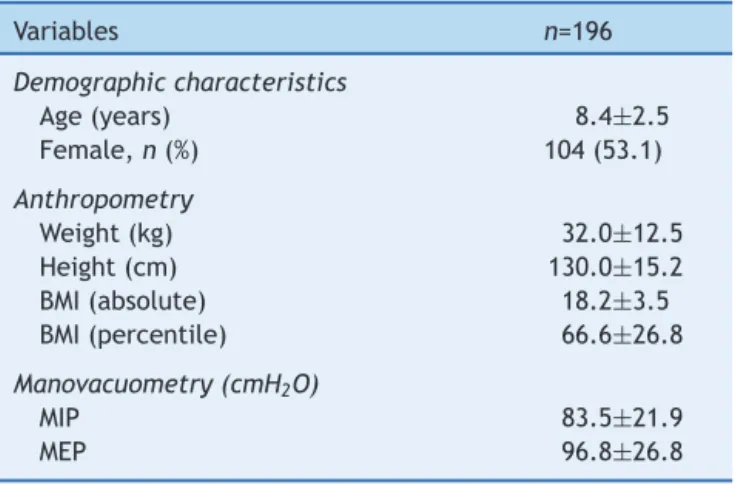
Table1 Characterizationofthestudysample.
Variables n=196
Demographiccharacteristics
Age(years) 8.4±2.5
Female,n(%) 104(53.1)
Anthropometry
Weight(kg) 32.0±12.5
Height(cm) 130.0±15.2
BMI(absolute) 18.2±3.5
BMI(percentile) 66.6±26.8
Manovacuometry(cmH2O)
MIP 83.5±21.9
MEP 96.8±26.8
Resultspresentedasmeanandstandarddeviation.
n,totalnumberofsubjects evaluated;BMI,bodymassindex; MIP, maximal inspiratory pressure; MEP,maximum expiratory pressure.
testwasconsideredsuccessfulwhenthesubjectperformed technicallycorrectmaneuvers,includingthreeacceptable measures(withoutairescaping)andtworeproducibleones (variationoflessthan10%betweenthetwolarger maneu-vers). The last value recorded could not be larger than the previous ones,4 and the final result was the highest
value obtained.The test wasconsidered inadequate (fail-ure)whenthesubjectevaluateddidnotreachthecriteria ofacceptabilityandreproducibilitydescribedabove.
Thesample sizewasestimated todetect afailurerate of approximately10%,witha confidencelevel of95% and amaximumacceptabledifferenceof5%.Forthat,itwould benecessarytoincludeatleast140individuals.Thus,the sampleincludedinthisstudysurpassesthisestimate.Data normalitywastestedusingtheKolmogorov---Smirnovtestand presentedanormaldistribution,sothedatawereexpressed asmeanandstandarddeviationofthemean.Thecategorical variableswerepresentedinabsoluteandrelativefrequency. Thecomparisonbetweenproportions(agegroupsand gen-derinrelationtothetestsuccessrate)wasperformedusing the Chi-square test. All analyses and the data processing wereperformedusingtheSPSSsoftware,version18.0(SPSS Inc., EUA). In all cases, the differences were considered significantwhenp<0.05.
Results
In thestudy,196children andadolescentswereincluded, withameanageof8.4±2.5years,weightof32.0±12.5kg, and130.0±15.2cmofheight;theywerepredominantly Cau-casian(69.4%),and53.1%werefemale.Thecharacterization ofthesamplewiththeanthropometricdataandinformation onrespiratorymusclestrengthareshowninTable1.
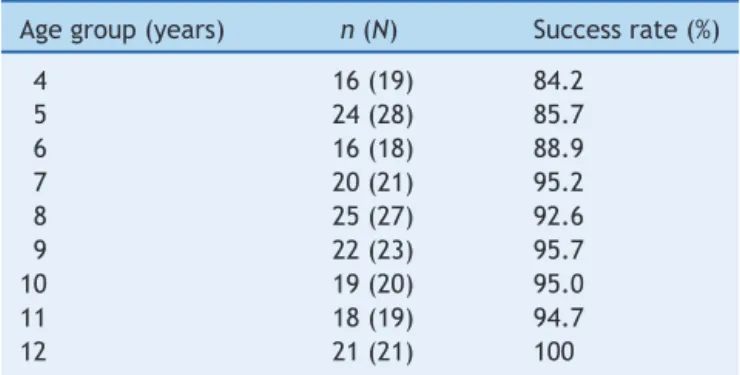
Table2 Success rateoftherespiratory musclestrength
testaccordingtotheagestudied.
Agegroup(years) n(N) Successrate(%)
4 16(19) 84.2
5 24(28) 85.7
6 16(18) 88.9
7 20(21) 95.2
8 25(27) 92.6
9 22(23) 95.7
10 19(20) 95.0
11 18(19) 94.7
12 21(21) 100
n,subjectswithasuccessfultest;N,totalsubjectsevaluated.
from84.2%at4yearsofageto100%at12years.Thesuccess valuesforeachagegroupareshowninTable2.
Whenthedifferencesbetweensuccessratesofchildren inthepre-schoolagerange(4and5years)andchildrenand adolescentsintheschoolagerange(6---12)werecompared, asignificantlylowersuccessratewasseen(p=0.032)inthe pre-school group (85.1%), compared to the school group (94.6%)(Fig.1).Differencesinthesuccessrateswerealso analyzedaccordingtogender.However,therewasno signif-icantdifference(p=0.575)whenthesuccessratesbetween boysandgirlswerecompared(Fig.2).
Discussion
In this study, the success rate observed in children and adolescentsevaluatedwas92.3%.Thisshowsthatthe respi-ratory muscle strength test is a simple resource,easy to apply and highly feasible in this age group. Further, it is a non-invasive method that supplies important infor-mation about the function of the respiratory muscles implicatedinthebreathingprocess,thatareofteninvolved inand/oratamechanicaldisadvantageunderseveral con-ditionsor clinicalsituations,asinlungandneuromuscular diseases.4,5
100
*
Preschool
School 80
60
40
20
Total rate observed
0
Failure Success Failure Success
Figure1 Comparisonbetweenthesuccessandfailurerates
observedinbothagegroups(preschoolandschool).*Chi-square
test:p=0.032.
100
Girls
Boys 80
60
40
20
Total rate observed
0
Failure Success Failure Success
Figure2 Comparisonbetweenthesuccessandfailurerates
observedinrelationtosex.
Tothebestofourknowledge,thisisthefirststudy aim-ingtodeterminethesuccessrateoftherespiratorymuscle strengthtestindifferentagegroupsofthepre-schooland schoolpopulation,whichmakesitdifficulttocomparethe valuesfoundinthoseofotherstudies.Inanycase, consid-eringotherlungfunctiontests,webelievethatthesuccess ratefound in thisstudy ishigh. Possiblecontributing fac-tors includea higher level of explanationtothe subjects evaluated,alongermeasurementtimeandpatienceofthe evaluatorresponsibleforperformingthetests.10Differently
fromspirometry,inwhichspecificstandardsandguidelines weredeveloped to allow itsuse in younger age groups,17
toevaluatetherespiratorymusclestrengthinthisstudyit wasnotnecessary touse anymethodologydifferent from thatpublishedbytheguideline,4,13 suggestingthatitisnot
difficult to perform the test in these age groups in the clinicalpractice.Whenwecomparedourresultstothe suc-cess rates of the spirometry test, the respiratory muscle strength test is also easy and simple, since the spirom-etry success rates are close to the results shown here, around85%.18---21 Additionally,areviewofrecentliterature
hasshownthatalthoughthepreschoolagegroupis charac-terizedasanextremelyyoung sample,withitsdifficulties andmotor limitations, thesuccess rate of thespirometry (regardless of previous experience) ranged between 71% and92%,demonstratingthefeasibilityofpulmonary evalu-ationinthisagegroup.22Althoughbothtestshavedifferent
methodologies,objectives andfunctionality, the compari-sonwithawell-knownandextensivelystudiedlungfunction testmayindicateaparameteruntilfurthersuccessratesare generatedfortheevaluationofpediatricrespiratorymuscle strength.
As expected,the successrates of the respiratory mus-cle strength test appear to increase with the age of the childrenevaluated.Inaddition,whencomparedtothe vari-ablesex,nosignificantdifferencewasfound.Thesefindings aresimilartothosefoundinvariousstudiesthatevaluated thelungfunctionsuccessratesinthepediatricpopulation, showingthat asthe children grow older, thesuccess rate alsorises.21,23,24Previousstudies thataimedat generating
normality values for the respiratory muscle strength test ascribethefailureofthetechniquetothedifficultyin under-standing,lowreproducibilityandlackofcooperationbythe childreninthisagegroup.13,14However,thesestudieshave
hinderingabetterknowledgeandunderstandingoftheage asaninfluencingfactoronthisoutcome.Inthissense, sev-eralstudiesthatevaluatedthefrequencyofsuccessofthe spirometrytesthave shownthat,in preschoolers,the dif-ficultyofobtaining anadequate test maybeexplainedas beingduetoreducedattention,easydistraction,difficulty inunderstanding,motorcoordination,andlowtolerancefor frustrationduringmaneuvers.Besides,thechild’semotional stage and stage of development are important factors in determiningthesuccessofthetest.18,25
Although the present study does not show informa-tionabout theprevious respiratoryhistoryofthesubjects included,itis believedthatthosefactorswouldnot influ-encetheabilityofanindividualtoperformthetest,which wasthemainoutcomeofthestudy.Also,itisunlikelythat severerespiratory conditionsthatcouldpossiblyalterthe performanceofthetestwouldbepresentinsuchayoung, healthysample,recruitedataschoolenvironment,andwith normalnutritionalstatus.Ontheotherhand,evenifthatis possible,previousstudies26,27haveshownthatmildto
mod-erateasthmaticsubjectsdonotpresentrespiratorymuscle strengthreduction, whichis usually associatedwithmore severelungdisease,includingthepresenceofhyperinflation andpoornutritionalstatus.28,29
One of the limitations of this study is that the test is performedby anexperienced evaluator,whoisinterested inachievingasmuchsuccessaspossibleinthetests,which mayhavecontributedtothehighsuccessratefoundinthis sample. However,these findings only strengthen the idea thatitispossibletoperformthistestinthepediatricage range,andthatatleastinpart,achievingsuccessdepends notonlyonthechildrenand/oradolescentsevaluated,but also on the effort and stimulus supplied by the evalua-tor.Inthissense,apreviousstudy30 recentlydemonstrated
thatthequalityofspirometrytestsincreasedfrom57%to 83%aftertheinclusionofatrainingprogramconductedby telemedicinein15participatingcenters.Newstudies con-cerningthefrequencyofsuccessinthepre-schoolagegroup shouldbeencouragedtoobtainnewinformationaboutthe behaviorofsuccessrates inthisagegroup,enabling com-parisonsamongstudiesandhelpingtoachievegreateruse ofthisresourceamongthechildpopulation.
Inbrief, therespiratorystrength test presented ahigh rate of success amongthe pre-school and school popula-tionevaluated.Besides,thesuccessrateappearstoincrease withage.Thefindingsofthisstudyshowthattherespiratory musclestrengthtestisasimpleandeasytoapplyresource. Thus, obtaining an adequate test may ensure the quality ofthemeasurementsandconsequently,successinthe con-trolandfollow-upoftheoutcome ofdifferentrespiratory involvements.
Funding
Thisstudydidnotreceivefunding.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgments
TheauthorsthankFAPERGSforthescholarship(JPHF).
References
1.MacedoSE,MenezesAM,AlbernazE,PostP,KnorstM.Risk fac-torsfor acute respiratory disease hospitalizationin children underoneyearofage.RevSaudePublica.2007;41:351---8. 2.ChiesaAM, Westphal MF, Akerman M. Acute respiratory
dis-eases: a study on health inequalities. Cad Saude Publica. 2008;24:55---69.
3.Rodrigues JC, Cardieri JM, Bussamra M, et al. Provas de func¸ão pulmonar em crianc¸as e adolescentes. J Pneumol. 2002;28:207---21.
4.SouzaRB.Pressõesrespiratóriasestáticasmáximas.JBras Pneu-mol.2002;28:155---65.
5.TomalakW,PogorzelskiA,PrusakJ.Normalvaluesformaximal staticinspiratoryandexpiratorypressuresinhealthychildren. PediatrPulmonol.2002;34:42---6.
6.PessoaIM,HouriNetoM,MontemezzoD,SilvaLA,AndradeAD, ParreiraVF.Predictiveequationsforrespiratorymusclestrength accordingtointernationalandBrazilianguidelines.BrazJPhys Ther.2014;18(5):410---8.
7.Mellies U, Stehling F, Dohna-Schwake C. Normal values for inspiratory muscle function in children. Physiol Meas. 2014;35:1975---81.
8.SimõesRP,DeusAP,AuadMA,DionísioJ,MazzonettoM, Borghi-SilvaA.Maximalrespiratorypressureinhealthy20to89 year-oldsedentaryindividualsofcentralSãoPauloState.RevBras Fisioter.2010;14:60---7.
9.SeverinoFG,Resqueti VR, BrunoSS, AzevedoIG, Vieira RH, FregoneziGA.Comparison betweena nationaland a foreign manovacuometerfornasalinspiratorypressuremeasurement. RevBrasFisioter.2010;14:426---31.
10.Heinzmann-FilhoJP, Vasconcellos VidalPC, Jones MH, Dona-dio MV. Normal values for respiratory muscle strength in healthy preschoolers and school children. Respir Med. 2012;106:1639---46.
11.ArnallDA,NelsonAG,OwensB,etal.Maximalrespiratory pres-surereference valuesfor Navajochildrenages6---14.Pediatr Pulmonol.2013;48:804---8.
12.Mendes RE, Campos TF, Macêdo TM, Borja RO, Parreira VF, Mendonc¸a KM. Prediction equations for maximal respi-ratory pressures of Brazilian adolescents. Braz J Phys Ther. 2013;17:218---26.
13.Domènech-ClarR,López-AndreuJA,Compte-TorreroL,etal. Maximal static respiratory pressures in children and adoles-cents.PediatrPulmonol.2003;35:126---32.
14.MateckiS,PriouxJ,JaberS,HayotM,PrefautC,RamonatxoM. Respiratorypressuresinboysfrom11---17yearsold:a semilon-gitudinalstudy.PediatrPulmonol.2003;35:368---74.
15.ParreiraVF,Franc¸aDC, ZampaCC,FonsecaMM, TomichGM, BrittoRR.Maximalrespiratorypressures:actualandpredicted valuesinhealthysubjects.RevBrasFisioter.2007;11:361---8. 16.Fiore Junior JF, Paisani DM, Franceschini J, Chiavegato LD,
FaresinSM.Maximalrespiratorypressuresand vitalcapacity: comparisonmouthpieceandface-maskevaluationmethods.J BrasPneumol.2004;30:515---20.
17.BeydonN,DavisSD, Lombardi E,et al.Anofficial American ThoracicSociety/EuropeanRespiratorySocietystatement: pul-monaryfunctiontestinginpreschoolchildren.AmJRespirCrit CareMed.2007;175:1304---45.
19.Pesant C, Santschi M, Praud JP, Geoffroy M, Niyon-senga T, Vlachos-Mayer H. Spirometric pulmonary function in 3- to 5-year-old children. Pediatr Pulmonol. 2007;42: 263---71.
20.SantosN,AlmeidaI,CoutoM,Morais-AlmeidaM,BorregoLM. Feasibilityofroutinerespiratoryfunctiontestinginpreschool children.RevPortPneumol.2013;19:38---41.
21.VerasTN,PintoLA.Feasibilityofspirometryinpreschool chil-dren.JBrasPneumol.2011;37:69---74.
22.VidalP,MattielloR,JonesM.Spirometryinpreschoolchildren. PulmãoRJ.2013;22:20---5.
23.MayerOH,JawadAF,McDonoughJ,AllenJ.Lungfunction in 3---5-year-old children withcystic fibrosis. Pediatr Pulmonol. 2008;43:1214---23.
24.Franc¸aDC,CamargosPA,MartinsJA,AbreuMC,AvelareAraújo GH,ParreiraVF.Feasibilityand reproducibilityofspirometry andinductanceplethysmographyinhealthyBrazilian preschool-ers.PediatrPulmonol.2013;48:716---24.
25.StocksJ.Clinicalimplicationsofpulmonaryfunctiontestingin preschoolchildren.PaediatrRespirRev.2006;7:S26---9. 26.OliveiraCM,LanzaF,SoléD.Respiratorymusclestrengthin
chil-drenand adolescentswithasthma:similartothatofhealthy subjects?JBrasPneumol.2012;38:308---14.
27.MarcelinoAM,CunhaDA,CunhaRA, daSilvaHJ.Respiratory musclestrengthinasthmaticchildren.IntArch Otorhinolaryn-gol.2012;16:492---6.
28.LaghiF,Tobin MJ.Disordersoftherespiratorymuscles. AmJ RespirCritCareMed.2003;168:10---48.
29.Weiner P, Suo J, FernandezE, Cherniack RM. The effectof hyperinflationonrespiratorymusclestrengthandefficiencyin healthysubjectsandpatientswithasthma.AmRevRespirDis. 1990;141:1501---5.