A novel three-dimensional dynamic anorectal ultrasonography
technique for the assessment of perineal descent, compared
with defaecography
S. M. Murad-Regadas, D. dos Santos, G. Soares, F. S. P. Regadas, L. V. Rodrigues, G. Buchen, V. T. Kenmoti, W. S. Surima˜ and G. O. da S. Fernandes
Department of Surgery, Clinical Hospital, Federal University of Ceara´, Brazil
Received 25 January 2011; accepted 13 April 2011; Accepted Article online 22 July 2011
Abstract
AimThe purpose of the study was to describe a novel three-dimensional dynamic anorectal ultrasonography technique (dynamic 3-DAUS) for assessment of perineal descent (PD) and establishment of normal range values, comparing it with defaecography. Secondarily, the study compares the ability of the two techniques to identify various pelvic floor dysfunctions.
MethodA prospective study was undertaken in 29 women (mean age 43 years) with obstructed defecation disorder. All patients underwent defaecography and dynamic 3-DAUS and the results were compared. Lee kappa coefficients (K) were used.
ResultsOn defaecography, PD > 3 cm was detected in 12 patients. On dynamic 3-DAUS, 10 of these patients had PD > 2.5 cm. Seventeen had normal PD on
defae-cography and PD£2.5 cm on dynamic 3-DAUS (K
0.85). Normal relaxation was observed in 10 patients and anismus in 14 with both techniques (K 0.65). Both techniques identified five patients without rectocele, two with grade I rectocele (K0.89 and 1.00, respectively) and 10 with grade II and nine with grade III (K0.72 and
0.77, respectively). Rectal intussusception was identified in six patients on defaecography. These were confirmed on dynamic 3-DAUS in addition to the identification of another seven cases indicating moderate agreement (K 0.46). Enterocele⁄sigmoidocele grade III was identified
in one patient with both techniques, indicating sub-stantial agreement (K0.65).
ConclusionDynamic 3-DAUS was shown to be a reliable technique for the assessment of PD and pelvic floor dysfunctions, identifying all disorders and confirm-ing findconfirm-ings from defaecography.
KeywordsUltrasound, perineal descent, pelvic floor, images
What is new in this paper?
This paper demonstrates a new three-dimensional dy-namic anorectal ultrasound technique to evaluate perineal descent and pelvic floor dysfunctions with the advantage of verifying all the pelvic floor anatomical structures and the integrity of anal muscles.
Introduction
The descending perineum syndrome, described in 1966 by Alan Parks [1], is defined quantitatively by the relationship of the anorectal angle to the pubococcygeal line on radiographs. It is a complex pelvic floor disorder usually associated with prolapse and symptoms such as impaired defecation, excessive straining and sensation of incomplete evacuation. In this situation, clinical
manage-ment – including a fibre-rich diet, bulk laxative and pelvic floor retraining – should be effective. On the other hand, excessive perineal descent can lead to the development of neuropathy-related faecal incontinence due to stretching injury to the pudendal nerve and sacral roots [1,2], although this may also be a late sign of the descending perineum syndrome. In such patients, response to treat-ment will be less effective. On clinical examination, the perineum may be seen ballooning downwards during straining; nevertheless, the descending perineum syn-drome is often not diagnosed clinically. In any case, the identification of this dysfunction and other pelvic floor disorders is important in the planning of proper Correspondence to: S. M. Murad-Regadas, Department of Surgery, Clinical
treatment. Current methods for evaluating pelvic floor disorders include manometry [3], defaecography [3–5], dynamic ultrasonography [6–12] and dynamic magnetic resonance imaging [13–15].
Defaecography is an established method of evaluating the dynamics of rectal voiding and anorectal dysfunctions [4,5]. Pelvic floor descent is the movement initiating defecation. It may be defined as the descent of the anorectal junction from rest to evacuation and can be measured as the vertical distance between the pubococcy-geal line and the anorectal junction. In normal subjects, the perineum descends 1–3 cm [16]. Other anorectal dysfunctions, such as anismus, rectocele, intussusception and sigmoidocele⁄enterocele, may be evaluated with
defaecography as well, although with the disadvantage of exposing patients to ionizing radiation [3–5].
In recent years, alternatives to defaecography, such as dynamic ultrasonography and dynamic magnetic reso-nance imaging, have been developed for the evaluation of pelvic floor dysfunctions, with good correlation and the advantage of showing the entire pelvis [6–15,17]. Thus, Murad-Regadas et al.[12] developed echodefae-cography, a three-dimensional dynamic anorectal ultra-sonography technique (dynamic 3-DAUS) using a 360
transducer, automatic scanning and high frequencies for high-resolution images to evaluate evacuation disorders affecting the posterior compartment (rectocele, intussus-ception, anismus) and the middle compartment (grade III sigmoidocele⁄enterocele). Echodefaecography was
shown to correlate well with conventional defaecography and was validated in a prospective multicentre study [17]. Murad-Regadaset al. [18] subsequently used the same transducer to evaluate perineal descent without, however, establishing the range of normality. The purpose of the present study was to describe a novel dynamic 3-DAUS for the assessment of perineal descent and establishment of normal range values, comparing it with conventional defaecography. Secondarily, the study compares the ability of the two techniques to identify a variety of pelvic floor dysfunctions in the posterior and middle compartment, such as perineal descent, anismus, rectocele (grades I, II or III), rectal intussusception and grade III sigmoidocele⁄enterocele. The results were
compared.
Method
Patients with obstructed defaecation disorder (excessive straining, vaginal splinting and sensation of incomplete evacuation), despite increased intake of dietary fibre (up 30 g⁄day for 3 months), were prospectively enrolled in
the study. Fifteen patients had undergone at least one vaginal delivery. The clinical protocol was previously
approved by the Research Ethics Committee of the Walter Cantı´dio University Hospital and all patients gave their informed written consent. The subjects were given a complete proctological examination and underwent def-aecography and dynamic 3-DAUS performed by different examiners for the evaluation of pelvic floor dysfunctions. The results were compared.
Defaecography
Defaecography was performed without opacification of the small bowel. Following rectal enema, the patient was placed in the left lateral position and approximately 25 ml of liquid iodine contrast was introduced into the vagina in order to demonstrate the effect of defaecation on the posterior vaginal wall. The rectum was filled with 200 ml barium paste. The patient was asked to sit on a special commode, contract the pelvic floor musculature and empty the rectum as completely as possible. Measurements were made at rest, squeeze and
Anterior
Bladder
Vagina
Maximal straining
PR
Posterior
PD = 1.2 cm
PR At rest
during expulsion of the contrast. A difference of more than 3 cm in the position of the anal canal between relaxation and straining was considered perineal descent [16].
Non-relaxation or paradoxical contraction of the pubo-rectalis muscle (PR) was considered present when the muscles failed to relax or contracted during defaecation.
Anterior rectocele was defined as a herniation of the anterior rectal wall protruding into the posterior vaginal wall during straining. It was measured perpendicularly to the expected contour of the anterior rectal wall and quantified according to the classification proposed by Marti et al. [19] (Grade I£2.0 cm; Grade II 2.0–
4.0 cm; Grade III > 4.0 cm). Sigmoidocele⁄enterocele
was defined as a herniation of the peritoneum (containing the sigmoid colon or small bowel) into the pelvis. It was considered significant when the loop of sigmoid⁄bowel
extended below the ischiococcygeal line (Grade III). Patients with an invagination of the rectal wall during straining not passing through the anal canal were diagnosed with intussusception.
Dynamic 3-DAUS
Dynamic 3-DAUS was performed with a three-dimen-sional ultrasound device (Pro-Focus, endoprobe model
2052; B-K Medical
, Herlev, Denmark) with proximal-to-distal 6.0-cm automatic scans. By moving two crystals on the extremity of the transducer, axial and longitudinal images were merged into a single cube image, recorded and analysed in multiple planes, as described in previous publications by Murad-Regadaset al.[11,12]. Following rectal enema, patients were examined in the left lateral position. Images were acquired by four automatic scans and analysed in the axial, sagittal and, if necessary, the oblique plane by an examiner blinded to defaecography findings.
Anterior
EAS
IAS
EAS
Posterior
PR
Vagina
Anterior
EAS
IAS
EAS
Posterior
PR
Vagina
(a) (b)
Figure 3 Sagittal plane: (a) angle measured in the rest position; (b) decreased angle (anismus) during straining (black and white lines). EAS, external anal sphincter; IAS, internal anal sphincter; PR, puborectal.
Anterior
Bladder
Vagina
Maximal straining
At rest
PR
PR
Posterior
PD > 2.5 cm
Scans 1, 3 and 4 used a slice width of 0.25 mm and lasted 55 s each. Scan 2 lasted 30 s with a slice width of 0.35 mm.
Scan 1 (rest)
Scan 1 was for verification of the anatomic integrity of the anal sphincters.
Scan 2
The transducer was positioned proximally to the PR (ano-rectal junction). The scan started with the patient at rest (3.0 s), followed by maximum straining with the transducer infixedposition.WhenthePRbecamevisibledistally,thescan was stopped. Perineal descent was quantified by measuring the distance between the position of the proximal border of the PR at rest and the point to which it had been displaced by maximum straining (PR descent) (Figs. 1 and 2). Instead of using the cut-off value for defaecography (> 3 cm), normal range values were established for dynamic 3-DAUS by comparing with measurements from defaecography.
Scan 3
The transducer was positioned at 6.0 cm from the anal verge. The patient was requested to rest during the first 15 s, strain maximally for 20 s, then relax again, with the transducer following the movement. The purpose of the
scan was to evaluate the movement of the PR and the external anal sphincter during straining, identifying normal relaxation, non-relaxation or paradoxical contrac-tion (anismus) (Fig. 3).
Scan 4
Following injection of 120–180 ml ultrasound gel into the rectal ampulla, the transducer was positioned at 7.0 cm from the anal verge. The scanning sequence was the same as in scan 3. The purpose of the scan was to visualize and quantify all anatomical structures and functional changes associated with voiding (rectocele, intussusception, Grade III sigmoidocele⁄enterocele) (Figs. 4 and 5).
Statistical analysis
Lee kappa coefficients were calculated to verify the agreement between the methods. Differences in mean perineal descent were analysed with Student’sttest (CI 95%). Bland and Altman plots were drawn for perineal descent values obtained with the two techniques and Pearson’s correlation coefficients were calculated to test for possible correlations. Results were considered statis-tically significant whenP< 0.05.
Results
Between March 2008 and February 2009, 29 female patients (mean age 43 years, range 23–74) with a mean validated Wexner constipation score [20] of 10 (range 8– 18) were prospectively enrolled in the study. Fifteen patients had undergone at least one vaginal delivery.
Perineal descent
On defaecography, perineal descent > 3.0 cm was detected in 12 patients. On dynamic 3-DAUS, 10 of these patients had PR descent > 2.5 cm. Seventeen patients had normal perineal descent on defaecography
and PR descent £2.5 cm on dynamic 3-DAUS. Thus,
two patients diagnosed with perineal descent > 3.0 cm on
defaecography were considered normal (PR
des-cent£2.5 cm) on dynamic 3-DAUS. Thus, the value
> 2.5 cm was established as a cut-off for perineal descent on dynamic 3-DAUS (Figs. 1 and 2).
The index of agreement between defaecography and dynamic 3-DAUS with regard to the diagnosis of perineal descent was high (kappa 0.85; 95% CI 0.49–1.0) (Table 1).
The mean perineal descent (± SEM) measured on defaecography and on dynamic 3-DAUS differed signifi-cantly (3.2 ± 0.21 cmvs2.3 ± 0.14 cm) (P= 0.001). The mean difference between the techniques was 0.90 cm (95%
Anterior Bladder
Vagina
Vagina
EAS
Straining At rest
IAS EAS
Posterior
PR
At rest Gel
CI 0.69–1.11). However, perineal descent values obtained with the two techniques were significantly correlated (kappa 0.90;P= 0.0001). Figure 6 shows the difference in perineal descent measured with the two methods.
Anismus
For the purposes of this study, non-relaxation and para-doxical contraction were classified as anismus. Normal relaxation was observed in 10 patients and anismus in 14 patients with both techniques. However, diagnosis was discordant in five patients. The index of agreement between defaecography and dynamic 3-DAUS was substantial (kappa 0.65; 95% CI 0.29–1.00) (P< 0.001) (Table 2).
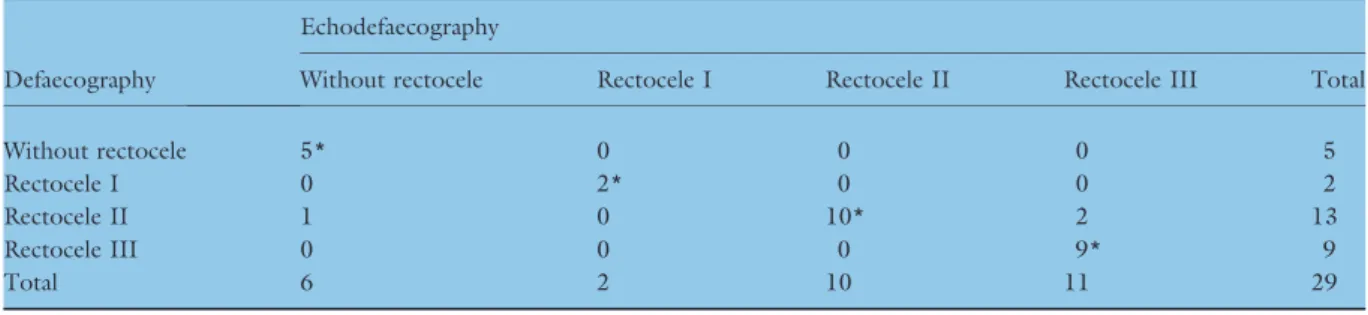
Rectocele
Both techniques identified five patients without rectocele, two with Grade I rectocele, 10 with Grade II rectocele
and nine with Grade III rectocele. Diagnosis was discor-dant in three cases with Grade II rectocele on defaecog-raphy: on dynamic 3-DAUS, two of these had Grade III rectocele and one had none. The index of agreement between defaecography and dynamic 3-DAUS was high with regard to patients without rectocele and Grade I rectocele (kappa 0.89 and 1.00; 95% CI 0.53–1.00 and 0.64–1.00, respectively) (P< 0.001), and agreement was substantial for Grade II and Grade III rectocele (kappa 0.72 and 0.77; 95% CI 0.37–1.00 and 0.41–1.00, respectively) (P< 0.001) (Table 3).
Table 1 Comparison of dynamic 3-DAUS (echodefaecography) with defaecography in the detection of perineal descent.
Defaecography
Echodefaecography Normal
perineal descent
Perineal descent Total
Normal perineal descent 17* 0 17
Perineal descent 2 10* 12
Total 19 10 29
*Concordant findings.
2.5
2.0
1.5
1.0
0.5
–0.5 0.0
0 1 2 3 4 5 6
–1.96 SD
AVERAGE of Defecography and Dynamic 3-DAUS
Def
ecog
raph
y - Dynamic 3-D
A
US
–0.21 0.90 Mean 2.01 +1.96 SD
Figure 6 Bland–Altman plot. The mean value of the perineal descent measured by defaecography and dynamic 3-DAUS.
Table 2 Comparison of dynamic 3-DAUS (echodefaecography) with defaecography in the detection of anismus.
Defaecography
Echodefaecography Normal
relaxation Anismus Total
Normal relaxation 10* 3 13
Anismus 2 14* 16
Total 12 17 29
*Concordant findings.
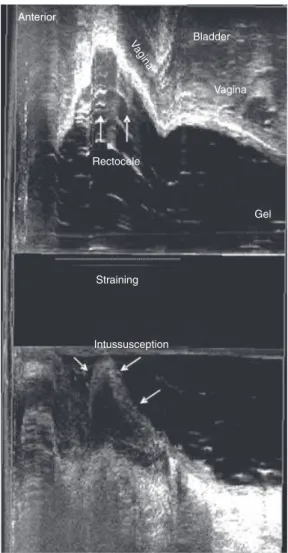
Anterior
Bladder
Vagina
Rectocele
Gel
Straining
Intussusception
Vagina
Rectal intussusception
Rectal intussusception was identified in six patients on defaecography. These were confirmed on dynamic 3-DAUS in addition to the identification of another seven cases (40%), indicating moderate agreement between the methods (kappa 0.46; 95% CI 0.12–0.79) (P< 0.007) (Table 4).
Grade III enterocele⁄sigmoidocele
Grade III enterocele⁄sigmoidocele was identified in one
patient on defaecography. This was confirmed on dynamic 3-DAUS in addition to the identification of another case, indicating substantial agreement between
the methods (kappa 0.65; 95% CI 0.31–0.99)
(P< 0.001).
Multiple dysfunctions
Perineal descent was associated with rectocele in eight patients in both examinations, with very high agreement (kappa 0.92; 95% CI 0.55–1.00) (Table 5). Rectocele was associated with intussusception in 16 patients in both examinations, with moderate agreement (kappa 0.47; 95% CI 0.13–0.81) (Table 6). Rectocele was associated with anismus in 13 patients in both examinations, with high agreement (kappa 0.86; 95% CI 0.50–1.00) (P< 0.001) (Table 7).
Discussion
Choosing the most suitable treatment for pelvic floor dysfunctions requires a complete clinical investigation and examination techniques capable of identifying ana-tomical and functional abnormalities. Defaecography is widely used [3–5] but does not allow visualization of anatomical structures such as the sphincter muscles, vagina and rectal wall. Other techniques using biplane endorectal [6,8], transperineal [7,9], three-dimensional transperineal [10] and three-dimensional anorectal
Table 4 Comparison of dynamic 3-DAUS (echodefaecography) with defaecography in the detection of intussusceptions.
Defaecography
Echodefaecography
Without Intussusception Total
Without 16* 7 23
Intussusception 0 6* 6
Total 16 13 29
*Concordant findings.
Table 5 Comparison of dynamic 3-DAUS (echodefaecography) with defaecography in the detection of perineal descent and rectocele association.
Defaecography
Echodefaecography
Without
Perineal
descent + rectocele Total
Without 20* 0 20
Perineal descent + rectocele
1 8* 9
Total 21 8 29
*Concordant findings.
Table 3 Comparison of dynamic 3-DAUS (echodefaecography) with defaecography in the detection of rectocele grade.
Defaecography
Echodefaecography
Without rectocele Rectocele I Rectocele II Rectocele III Total
Without rectocele 5* 0 0 0 5
Rectocele I 0 2* 0 0 2
Rectocele II 1 0 10* 2 13
Rectocele III 0 0 0 9* 9
Total 6 2 10 11 29
*Concordant findings.
Table 6 Comparison of dynamic 3-DAUS (echodefaecography) with defaecography in the detection of rectocele and intussus-ception association.
Defaecography
Echodefaecography
Without
Rectocele +
intussusception Total
Without 6* 1 7
Rectocele + intussusception
6 16* 22
Total 12 17 29
[11,12,17] transducers have been tested in the evaluation of pelvic floor dysfunctions with findings comparable to those of defaecography. These techniques have made it possible to clearly visualize all muscles, anatomical structures and changes during straining.
Murad-Regadas et al. [11,12] demonstrated the
advantage of using three-dimensional anorectal transduc-ers to evaluate pelvic floor dysfunctions, but did not include perineal descent in the technique. The present study describes a novel 3-DAUS technique for the assess-ment of perineal descent and establishes normal range values by comparing dynamic 3-DAUS findings with defaecography. The difference in position of the PR at rest and during maximum straining was measured (PR descent). Even with patients in the lateral position, the displacement of the PR is easily visualized and quantified. On dynamic 3-DAUS, normal perineal descent during straining was defined as a difference in PR position of
£2.5 cm and perineal descent > 2.5 cm. Acquisition
requires only 30 s and can easily be repeated. Although mean perineal descent was significantly greater on defae-cography (3.2 cm) than on dynamic 3-DAUS (2.3 cm), the methods were positively correlated. The difference may be explained by the difference in patient position during the examination (seated on a commode during defaecog-raphyvslying in the left lateral position during 3-DAUS). Thus, despite the fact that the two methods were in almost perfect agreement with regard to the detection of perineal descent, intrinsic technical differences justified the estab-lishment of normal range values for dynamic 3-DAUS.
Barthetet al.[6] tested a rigid linear endoanal probe with the patient in the lateral position, measuring the displacement of the PR (perineal descent) between rest and maximal straining and comparing findings with defaecography. According to the authors, the average displacement of the PR during straining was 12 mm (range 5–23 mm). Their measurements differ from ours mainly because of differences in image type and trans-ducer position. Our study shows a substantial agreement between defaecography and dynamic 3-DAUS with regard to the diagnosis of perineal descent⁄PR descent.
Likewise, Barthetet al.[6] reported a good correlation with defaecography. The pubic bone and the PR are not easily visualized with the transducer in the rectum, even when a three-dimensional anorectal transducer is used. Dietzet al.[7] described a technique for the assessment of pelvic organ descent with two-dimensional translabial ultrasound, measuring the distance between the base of the rectal ampulla and the lower margin of the symphysis pubis during the Valsalva manoeuvre. The technique was shown to correlate well with clinical measurements.
Other studies have shown the advantage of using magnetic resonance defaecography to evaluate all three compartments of the pelvic floor and provide a complete overview of structures (organs, bones and musculature) on which lines and angles may be drawn despite the supine position [13,14]. However, open dynamic mag-netic resonance can be performed with the patient seated on a commode [15].
In the present study, defaecography was chosen for comparison because, in spite of patient discomfort and exposure to radiation, it is still considered the gold standard in the assessment of posterior compartment disorders [4,5]. Defaecography and dynamic 3-DAUS were shown to yield similar results in the evaluation of rectocele size, intussusception, anismus and Grade III sigmoidocele⁄enterocele, as shown by a comparison with
results published by Murad-Regadaset al.[12]. Studies using ultrasound with different types of transducers and different techniques have produced findings compatible with defaecography even when a transperineal or transrectal probe was employed or the patient was placed in the left lateral or supine position as opposed to the sitting position used in defaecography [6–10]. The transperineal technique has the advantage of evaluating pelvic floor dysfunctions in the anterior, middle and posterior compartment without the use of radiation, even with the patient in the lateral or supine position and the pressure probe on the perineum [10].
In this study, posterior pelvic floor dysfunctions were evaluated. In spite of the association of dysfunctions, there was a substantial agreement between defaecography and dynamic 3-DAUS in the detection of perineal descent and rectocele. Likewise, a substantial agreement was observed in the identification of rectocele associated with intussus-ception. Some reports have covered multiple dysfunctions in the same patient [6,7,9,10,21]. The pelvic floor is a unit divided in three compartments (anterior, middle and posterior) and subject to multiple symptoms related to urinary and faecal incontinence, organ prolapse and obstructed defaecation. All dysfunctions should be iden-tified before choosing the best approach.
The advantage of dynamic 3-DAUS is the possibility of directly identifying anatomical structures of the pelvic floor,
Table 7 Comparison of dynamic 3-DAUS (echodefaecography) with defaecography in the detection of rectocele and anismus association.
Defaecography
Echodefaecography
Without Rectocele + anismus Total
Without 14* 1 15
Rectocele + anismus 1 13* 14
Total 15 14 29
changes during straining, evacuation disorders and sphinc-ter damage in a single examination [11,12,17]. Our study used a 16-MHz rotating transducer with two crystals (axial and longitudinal) on the extremity, producing a merged three-dimensional cube image recorded in real time for subsequent analysis (as in magnetic resonance). Automatic acquisition results in a volume image which can be freely manipulated in all planes and allows visualizing the ana-tomical structures simultaneously after image processing.
The current dynamic 3-DAUS technique may be limited by the position of the patient and the probe into the rectum. However, it has been found to correlate well with defaecography. Further analyses are required to compare dynamic 3-DAUS with transperineal ultraso-nography or dynamic magnetic resonance defaecography. The standardization of the technique, parameters and values of dynamic 3-DAUS, as proposed in this study, makes the method reproducible.
In conclusion, dynamic 3-DAUS was shown to be a reliable technique for the assessment of perineal descent and pelvic floor dysfunctions, identifying all disorders and confirming findings with conventional defaecography. In addition, dynamic 3-DAUS makes it possible to verify the anatomical integrity of anorectal structures and to detect sphincter injury during a single examination. The tech-nique is time-saving, inexpensive, radiation-free and well tolerated by patients.
References
1 Parks AG, Porter NH, Hardcastle J. The syndrome of the descending perineum.Proc R Soc Med1966;59:477–82.
2 Bartolo DC, Read NW, Jarratt JA, Read MG, Donnelly TC, Johnson AG. Differences in anal sphincter function and clinical presentation in patients with pelvic floor descent. Gastroenterology1983;85:68–75.
3 Wald A, Caruana BJ, Freimanis MG, Bauman DH, Hinds JP. Contribuitions of evacuation proctography and anorectal manometry to evaluation of adults with constipation and defecatory difficulty.Dig Dis Sci1990;35:481–7.
4 Mahieu P, Pringot J, Bodart P. Defecography: I. Description of a new procedure and results in normal patients. Gastro-intest Radiol1984;9:247–51.
5 Bartram CI, Turnbull GK, Lennard-Jones JE. Evacuation proctography: an investigation of rectal expulsion in 20 subjects without defecatory disturbance.Gastrointest Radiol 1988;13:72–80.
6 Barthet M, Portier F, Heyries L. Dynamic anal endosonog-raphy may challenge defecogendosonog-raphy for assessing dynamic anorectal disorders: results of a prospective pilot study. Endoscopy2000;32:300–5.
7 Dietz HP, Haylen BT, Broome J. Ultrasound in the quantification of female pelvic organ prolapse. Ultrasound Obstet Gynecol2001;18:511–4.
8 Van Outryve SM, Van Outryve MJ, De Winter BY, Pelck-mans PA. Is anorectal endosonography valuable in dyschesia? Gut2002;51:695–700.
9 Beer-Gabel M, Teshler M, Schechtman E, Zbar AP. Dynamic transperineal ultrasound vs. defecography in patients with evacuatory difficulty: a pilot study. Int J Colorectal Dis2004;19:60–7.
10 Dietz HP, Steensma AB. Posterior compartment prolapse on two-dimensional and three-dimensional pelvic floor ultra-sound: the distinction between true rectocele, perineal hypermobility and enterocele. Ultrasound Obstet Gynecol 2005;26:73–7.
11 Murad-Regadas SM, Regadas FSP, Rodrigues LV et al. A novel procedure to assess anismus using three-dimensional dynamic ultrasonography.Colorectal Dis2006;9:159–65.
12 Murad-Regadas SM, Regadas FSP, Rodrigues LV, Silva FRS, Soares FA, Escalante RD. A novel three-dimensional dynamic anorectal ultrasonography technique (echodefecog-raphy) to assess obstructed defecation, a comparison with defecography.Surg Endosc2008;22:974–9.
13 Lienemann A, Anthuber C, Baron A, Kohz P, Reiser M. Dynamic MR colpocystorectography assessing pelvic floor descent.Eur Radiol1997;7:1309–17.
14 Kaufman HS, Buller JL, Thompson JRet al.Dynamic pelvic magnetic resonance imaging and cystocolpoproctography alter surgical management of pelvic floor disorders.Dis Colon Rectum2001;44:1575–83; discussion 83–4.
15 Dvorkin LS, Hetzer F, Scott SM, Williams NS, Gedroyc W, Lunniss PJ. Open-magnet MR defaecography compared with evacuation proctography in the diagnosis and management of patients with rectal intussusception.Colorectal Dis2004;
6:45–53.
16 Brennan D, Williams G, Kruskal J. Practical performance of defecography for the evaluation of constipation and incon-tinence.Semin Ultrasound CT MR2008;29:420–6.
17 Regadas FSP, Haas EM, Abbas MA et al. Prospective multicenter trial comparing echodefecography with defecog-raphy in the assessment of anorectal dysfunctions in patients with obstructed defecation. Dis Colon Rectum 2011; 54:
686–92.
18 Murad-Regadas SM, Regadas FSP. (2008) Dynamic two-and three-dimensional ultrasonography: echodefecography. In: Imaging Atlas of the Pelvic Floor and Anorectal Diseases (eds Pescatori M, Regadas FSP, Murad-Regadas SM, Zbar AP), pp. 205–17. Springer, Italia.
19 Marti MC, Roche B, Dele´aval J. Rectoceles: value of video-defecography in selection of treatment policy.Colorectal Dis 1999;1:324–9.
20 Agachan F, Chen T, Pfeiffer J, Reissman P, Wexner SD. A constipation scoring system to simplify evaluation and management of constipated patients. Dis Colon Rectum 1996;39:681–5.