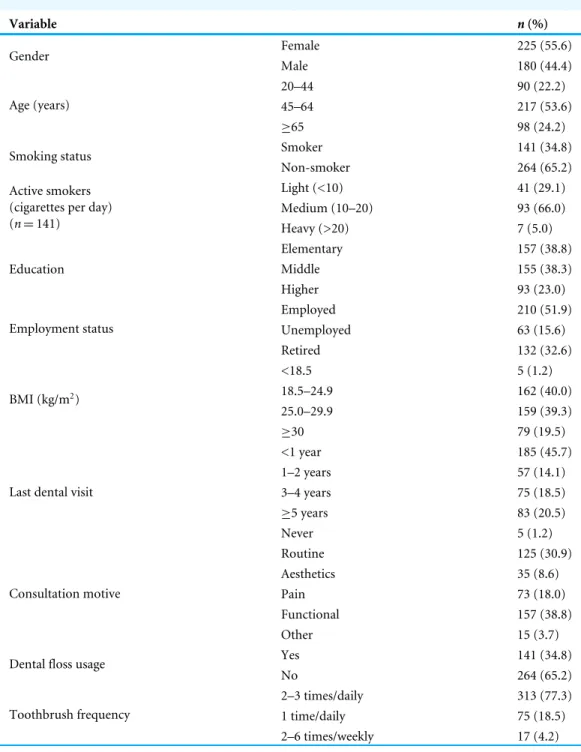
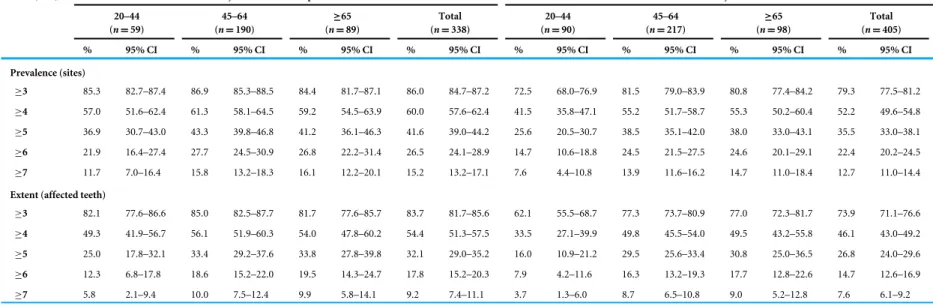
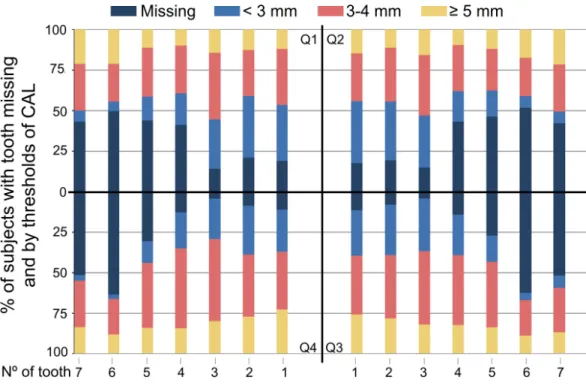
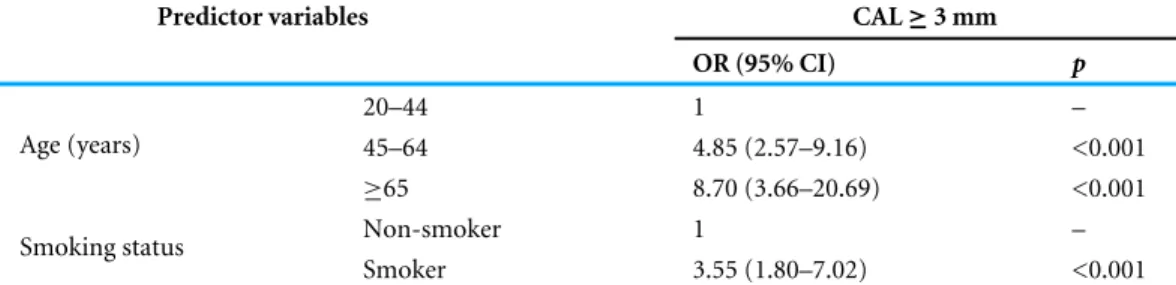
Prevalence and extent of chronic periodontitis and its risk factors in a Portuguese subpopulation: a retrospective cross-sectional study and analysis of clinical attachment loss
Texto
Imagem


Documentos relacionados
De acordo com o objetivo geral dessa dissertação, de monitorar e quantificar o processo de interceptação na Floresta Estacional Decidual, inserida no Bioma Mata Atlântica, através
Buscando entender os motivos que levam os professores a não utilizar os softwares matemáticos em suas aulas, questionou-se sobre este tema, e diversos são os motivos, tais como
The aim of the present study was to assess the prevalence of Common Mental Disorder (CMD) among incarcerated women and to investigate its association with sociodemographic
The aim of this study is to analyze epidemiological aspects of chronic back problems in Brazil, such as prevalence and the association with demographic and socioeconomic
Objective: The aim of our study was to assess body composition status and its association with inflammatory profile and extent of intestinal damage in ulcerative colitis
The aim of this case control study was to assess the association between the extent and severity of chronic periodontitis and oral cavity and/or oropharyngeal cancer.. The case
herefore, the aim of this study was to estimate the prevalence of overweight and investigate its association with sociodemographic factors, physical activity
