www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
The
effect
of
Foreign
Body
Aspiration
training
on
the
knowledge
level
of
pupils
夽
Selen
Ozakar
Akca
HititUniversityHealthSchool,Corum,Turkey
Received20March2015;accepted28June2015 Availableonline6November2015
KEYWORDS ForeignBody Aspiration(FBA); Nurse;
Training; Child
Abstract
Introduction:Educatorsdealingwith0---6yearsoldchildrenmustbeindividualswhoarewilling totakeallkindofmeasuresinordertoensurethesafetyofchildrenineducational institu-tionsandplaygrounds,providingprotectionfromdiseases,andwhoareabletoapplyfirstaid measuresincaseofanaccident.
Objective:Inthisstudy,weaimedtodeterminethelevelofknowledgeofallstudents continu-ingtheireducationinthedepartmentforchilddevelopment,regardingForeignBodyAspiration (FBA)andtheeffectofFBAtrainingontheirknowledgelevel.
Methods:Thissemi-experimentalstudywascarriedoutonhigh-schoolstudents(n=123) con-tinuingtheireducationinthedepartmentforchilddevelopmentinCorum, Turkey.Thedata wasevaluatedwithappropriatestatisticalmethods,andp<0.05wasdeterminedasstatistically significant.
Results:Beforethetraining,80%ofthehigh-schoolchildrenknewtheimportanceofagefactor incasesofFBA,improvingto92%aftertraining.Theincreaseinthenumberofstudentswho wereawareoftheimportanceofagefactorwasstatisticallysignificant(p<0.05).
Conclusion:Asaresultofthetraining,thevisualpresentationandtrainingonmodelsrelated toFBAhaveledtoanincreaseintheknowledgelevelofthestudents.
© 2015 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http:// creativecommons.org/licenses/by/4.0/).
夽 Pleasecitethisarticleas:AkcaSO.TheeffectofForeignBodyAspirationtrainingontheknowledgelevelofpupils.BrazJ
Otorhino-laryngol.2016;82:408---15.
E-mails:[email protected],[email protected],[email protected] http://dx.doi.org/10.1016/j.bjorl.2015.06.005
PALAVRASCHAVE Aspirac¸ãodecorpo estranho(ACE); Enfermeiro; Treinamento; Crianc¸a
Efeitodotreinamentoemaspirac¸ãodecorpoestranhononíveldeconhecimentode estudantes
Resumo
Introduc¸ão: Oseducadoresquelidamcomcrianc¸asde0-6anosdevemserpessoasdispostasa usartodosostiposdemedidasqueasseguremaseguranc¸adascrianc¸aseminstituic¸ões edu-cacionaiseemplaygrounds,proporcionandoprotec¸ãocontradoenc¸aseaplicandomedidasde primeirossocorrosemcasodeacidentes.
Objetivo: Nesteestudo,objetivamosdeterminaroníveldeconhecimentodeestudantesemum departamentodedesenvolvimentoinfantil,comrelac¸ãoàaspirac¸ãodecorpoestranho(ACE), eoefeitodotreinamentoparaACEemseuníveldeconhecimento.
Métodos: Realizamosestudodotiposemiexperimentalemtodososestudantes(n=123)que estavamdandocontinuidadeàsuaeducac¸ãonodepartamentodedesenvolvimentoinfantilde uma instituic¸ãodeeducac¸ãosecundáriaem Corum, Turquia.Osdadosforamavaliadoscom métodosestatísticosapropriados.Adotamosp<0,05comonívelestatisticamentesignificante. Resultados: Antesdotreinamento,80%dosescolarestinhamconhecimentodaimportânciado fatoridadenoscasosdeACE;depoisdotreinamento,essepercentualseelevoupara92%.Houve aumentoestatisticamentesignificantenonúmerodeestudantesquepercebiamaimportância dofatoridade(p<0,05).
Conclusão:Comoresultadodotreinamento,aapresentac¸ãovisualeotreinamentoemmodelos comrelac¸ãoàACElevaramaumaumentononíveldeconhecimentodosestudantes.
© 2015 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http:// creativecommons.org/licenses/by/4.0/).
Introduction
Foreign Body Aspiration (FBA) is the act of inhaling or breathingforeignbodies/objectsintotherespiratorytract. Children put these objects themselves into their mouths or the objects are given to them by others. As a result nearlycompleteobstruction/embolizationorevenhypoxia may occur andsymptoms and findings occur according to the level of obstruction.1,2 Foreign BodyAspiration
symp-tomsarisein70%inchildrenunder2years,whilechildren between1and3yearsconstitutemorethan75%.3
The reasons why Foreign Body Aspiration is seen fre-quentlyamong1---3agedgroupchildrenareasfollows;the fact that children try to put everything (nuts, toy parts, candyandcoins)intotheirmouthsinordertoacknowledge theirenvironment,performactivitieslikerunning,playing, laughingduringeating,havenotdevelopedtheirbackteeth foreating,havenotreceivededucationfor eating,eaton their own, possess immature neuromuscular mechanisms, anatomicalstructureoflarynxandepiglottisandlow socio-economic level.1,4,5 Apart fromthe factors relatedto the
patient,thestructuralspecificationsoftheaspiratedobject arealsoimportant.Theaspirationriskofsmall,smooth sur-face,roundorcylindricalshapedobjectsishigher.6
If the diagnosis of children who have aspirated a for-eignbodyisestablishedearly.Usuallyminimalcomplications develop,whereasifinspiteofearlydiagnosisno interven-tioniscarriedoutseriousanddifferentcomplications like recurrentpneumonia,pulmonaryabscessandbronchiectasis mayappear.6,7Ifprotectionisconsideredasthemost
impor-tantfactorofFBAandtherelatedcomplications,themain principlesofprotectingchildrenfromFBAareasmentioned
below:tokeepobjectswhich canbeaspiratedawayfrom children,andtotakepriortotheeventmeasureslike nutri-tioneducationetc. or relatedmeasures duringthe event (educationof familyandother adultstaking care of chil-dren regarding appropriate intervention to the child who hasaspiratedforeignbodiesetc.).8
Inthisrespect,theeducatorswhoaregivingeducation to0---6yearoldchildrenmustbeindividualswhoaretaking definitivemeasures in orderto ensure the safetyof chil-drenineducationalinstitutionsandplaygrounds,providing protectionfromdiseaseandarecapableof doingfirstaid applicationsin case of eventual accidents. As a result of thattheimportanceofcreatingpublicawarenessand train-ingofeducatorsresponsibleforchildcareisincreasing.8---10
ItisproposedthattheForeignBodyAspirationtrainingtask offamiliesandindividualsresponsibleforbabycareshould befulfilledbynurseswhohaveacounselingandeducational role.11
Considering the training and motivation of individuals responsibleforchildcarethispresentstudyaimedto deter-minetheknowledgelevelofpupilswhoarestudyinginthe departmentfor child developmentregarding FBAand the effectofFBAtrainingontheirknowledgelevel.
Methods
Preparation
thestudyconsistedof123pupilscontinuingtheireducation athighschoolinthedepartmentforchilddevelopment.No sampleselectionwasperformedandallpupilswereincluded in the study. The study was conducted on 100 voluntary pupils (100/123). Success rate of obtaining the sampling within the study was 81.3%. Before starting the study, the approval of the Provincial Directorate of Education and (20.10.2014/4674732) Ankara Numune Education and ResearchHospitalethicscommittee(05.11.2014/E-14-325) havebeenobtained.Apartfromthatvoluntarily participat-ingpupilshavebeeninformedaboutthepurposeofthestudy andwrittenconsentwasobtained.
Variablesoftheresearch
Independentvariablesconsistofdescriptivecharacteristics ofthestudents ofthe childdevelopmentdepartmentand whetherornottheycompletedtrainingaboutFBAbefore. ThedependentvariablewasthetrainingaboutFBAgivento thestudentsofchilddevelopment.
Instruments
Questionnaire
Datacollectionquestionnairewasdevelopedinaccordance tothewithresearcherandtheliteratureinformation.4,12---14
Itconsisted of questionsabout pupils’defining character-istics, knowledgelevel related toForeignBody Aspiration (ear---nose and respiratory) and knowledge about protec-tion from FBA. The pre-application was rehearsed on 10 pupils,necessary correctionsweremadeaccording tothe obtainedresponses andthefinal documentcomprisedthe questionnaire. 10th gradepupils who performed the pre-applicationofthestudyanddidtheirnurseryschooltraining betweenthedatesofstudywereexcluded.Questionnaires wereappliedbeforethetrainingandonemonthafter;taking approximately15minunderthesupervisionofaresearcher
ForeignBodyAspiration(ear,noseandrespiratory tract)training
Itwascarriedoutbytheresearcherintwostagesasavisual presentationandmodel.
Visualpresentation
Prepared in line with literature4,12---14 and lasting
approxi-mately45min,thevisualtrainingsubjecthasincludedthe answerstoquestionslike;‘‘What areFBAs (ear,noseand respiratorytract)?What isthefrequency ofFBA,the gen-derand agegroup? What arethecommon causes for FBA onchildren?Whatarethemostcommonaspiratedfoodand substancesbychildren?Whichsymptomscanbeseeninthe caseofpartialandcompleteobstructionoftherespiratory tractbyforeignbodies?Whatshouldcomprisefirstaidinthe caseofcompleteandpartialobstructionofrespiratorytract byforeignbodyinamorethanoneyearoldandconscious child?Whatshouldcomprisefirstaidinthecaseofcomplete obstructionofrespiratorytractbyforeignbodyinanunder oroveroneyearoldandunconsciouschild?Whatarethefirst symptomsofforeignbodiesinear(insects,legumes,small
particlestoys)andwhatshouldcomprisefirstaid?Whatare thefirstsymptomsof aspiratedforeignbodiesinthenose andhowshouldtheybetreated?Howshouldchildrenbe pro-tectedfromFBA?’’Theappliedtraininghasbeencarriedout ononeinfantandchildmodel.Everystudentperformedthe trainingonthemodel.Inthetrainingitwasdemonstrated whatfirstaidinterventionshouldbeandappliedincaseof partialandcompleteobstructionofrespiratorytractdueto FBAin<1yearand>1yearchildrenandcomplete obstruc-tionofrespiratorytractin<1yearand>1yearunconscious children.
Statisticalanalysis
Afterthepreliminarytest(beforetraining)andthefinaltest (aftertraining)wereapplied,theresponsestoopen-ended questionsinthequestionnairehavebeencodedand infor-mation givenin visual presentation has been accepted as accurateinformation.
Evaluationofthedataobtainedfromthequestionnaire resultswasperformedincomputerenvironmentbyusingthe SPSS17.0(StatisticalPackageforSocialScience)packet pro-gram.Inthedataevaluationchi-squarewasusedinorderto evaluatethedifferencesamongagegroupsduringdata anal-ysisanddeterminepercentagedistributionandaveragesin ordertoexaminetheencounteredagegroupsandgenders, defining characteristics of pupils, confrontation with FBA and perception and the McNemar test was carried out in orderto examinethe effectof FBAtrainingand informa-tionofFBA(ear,nose,respiratorytract)seenonchildren’s knowledgelevel.p<0.05wasacceptedasstatistically sig-nificant.
Results
The average age of pupilsparticipating in the study was 17.01±0.73.Itwasobservedthat99%(n=99)ofthepupils hadnotattendedtoanyseminar/courserelatedtoFBA.
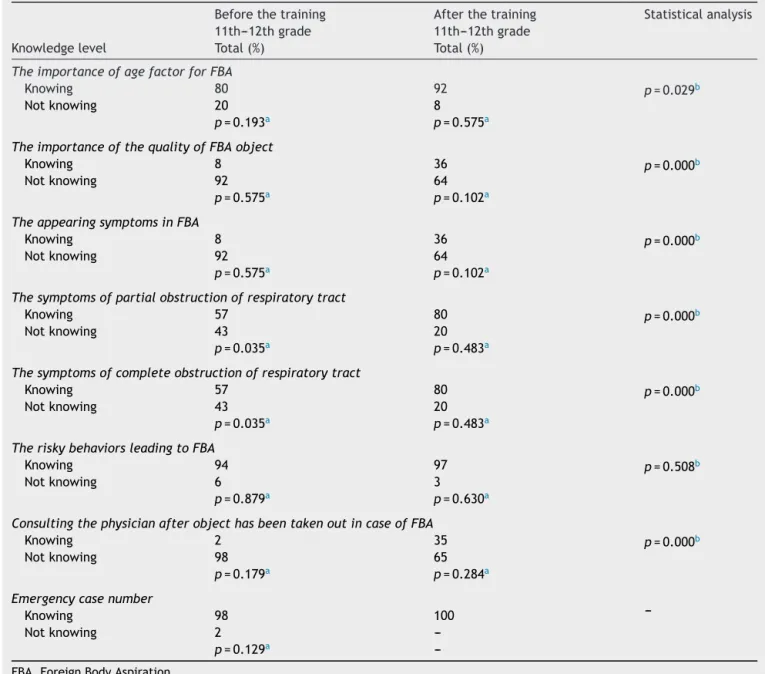
Table1 ComparisonofknowledgelevelsofstudentsincaseofFBA(nose---ear---respiratorytrack)beforeandafterthetraining.
Beforethetraining Afterthetraining Statisticalanalysis 11th---12thgrade 11th---12thgrade
Knowledgelevel Total(%) Total(%)
TheimportanceofagefactorforFBA
Knowing 80 92 p=0.029b
Notknowing 20 8
p=0.193a p=0.575a
TheimportanceofthequalityofFBAobject
Knowing 8 36 p=0.000b
Notknowing 92 64
p=0.575a p=0.102a
TheappearingsymptomsinFBA
Knowing 8 36 p=0.000b
Notknowing 92 64
p=0.575a p=0.102a
Thesymptomsofpartialobstructionofrespiratorytract
Knowing 57 80 p=0.000b
Notknowing 43 20
p=0.035a p=0.483a
Thesymptomsofcompleteobstructionofrespiratorytract
Knowing 57 80 p=0.000b
Notknowing 43 20
p=0.035a p=0.483a
TheriskybehaviorsleadingtoFBA
Knowing 94 97 p=0.508b
Notknowing 6 3
p=0.879a p=0.630a
ConsultingthephysicianafterobjecthasbeentakenoutincaseofFBA
Knowing 2 35 p=0.000b
Notknowing 98 65
p=0.179a p=0.284a
Emergencycasenumber
Knowing 98 100
---Notknowing 2
---p=0.129a
---FBA,ForeignBodyAspiration.
a Chi-square. b McNemartest.
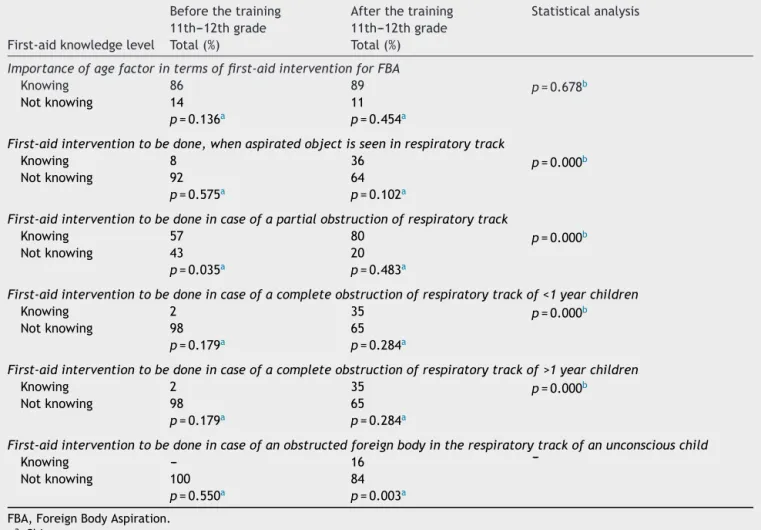
InTable2,thenumberofpupilsawareoftheimportance oftheagefactorregardingthefirstaidinterventionincase ofFBAandwhoknewthe firstaid interventionfor uncon-sciouschildren whohaveinhaled foreignbodiesincreased after training compared to before training; this increase was not statistically significant (p>0.05). Furthermore it wasdeterminedthat8%ofschoolchildrenparticipatingin thestudyknew thefirstaid interventionifaspiratedbody can be seen in the respiratory tract before training and 36% after training, 57% knew the first aid intervention in caseofpartialobstructionofrespiratorytractbefore train-ing and 80% after training, 2% were informed of first aid interventionincaseofcompleteobstructionofrespiratory tracton<1yearand>1yearoldchildrenbefore-trainingand 35%after-training.Nostatisticallysignificantdifferencewas found among the before-training and after-training group
(p>0.05), nevertheless the increase of knowing first aid interventionofpupilsincase ofan aspiratedbodycanbe seeninrespiratorytract,partialobstructionofrespiratory tract,complete obstruction of respiratorytractamong<1 yearand>1yearoldchildrenincaseofFBAwasstatistically significant(p<0.05)(Table2).
Table2 Comparisonoffirst-aidknowledgelevelsofstudentsincaseofFBAinrespiratorytrackbeforeandafterthetraining.
Beforethetraining Afterthetraining Statisticalanalysis 11th---12thgrade 11th---12thgrade
First-aidknowledgelevel Total(%) Total(%)
Importanceofagefactorintermsoffirst-aidinterventionforFBA
Knowing 86 89 p=0.678b
Notknowing 14 11
p=0.136a p=0.454a
First-aidinterventiontobedone,whenaspiratedobjectisseeninrespiratorytrack
Knowing 8 36 p=0.000b
Notknowing 92 64
p=0.575a p=0.102a
First-aidinterventiontobedoneincaseofapartialobstructionofrespiratorytrack
Knowing 57 80 p=0.000b
Notknowing 43 20
p=0.035a p=0.483a
First-aidinterventiontobedoneincaseofacompleteobstructionofrespiratorytrackof<1yearchildren
Knowing 2 35 p=0.000b
Notknowing 98 65
p=0.179a p=0.284a
First-aidinterventiontobedoneincaseofacompleteobstructionofrespiratorytrackof>1yearchildren
Knowing 2 35 p=0.000b
Notknowing 98 65
p=0.179a p=0.284a
First-aidinterventiontobedoneincaseofanobstructedforeignbodyintherespiratorytrackofanunconsciouschild
Knowing --- 16
---Notknowing 100 84
p=0.550a p=0.003a
FBA,ForeignBodyAspiration.
aChi-square. b McNemartest.
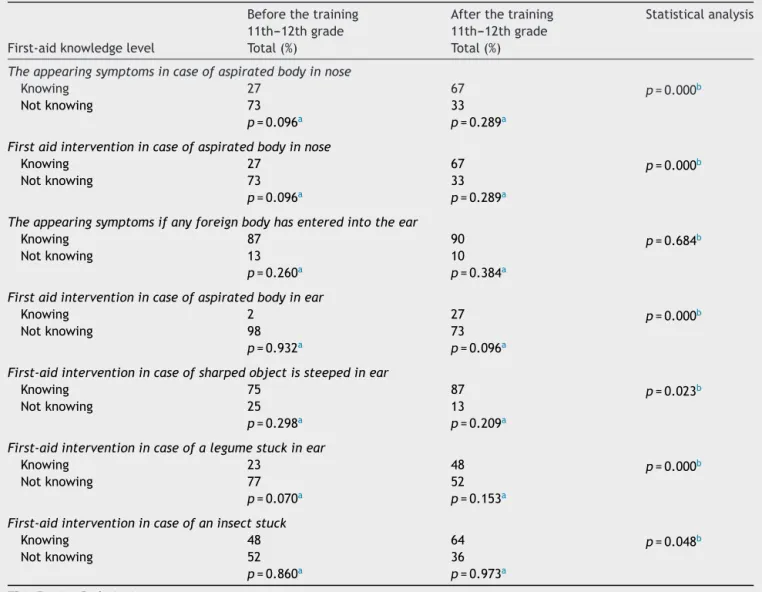
trainingand64% after training.Nostatistically significant differencewasfoundamongthebefore-trainingand after-traininggroup(p>0.05),neverthelesstheincreaseofpupils’ knowledgeaboutfirstaidinterventionincaseofdeveloping symptomswhena foreignbodyhasenteredintothenose, orifaforeignbodycanbeseenintheearcanal,alegume orinsecthasenteredtheearwasdeterminedtobe statis-tically significant (p<0.05)(Table 3).In Table3 it canbe observedthatthenumberofpupilsawareoftheappearing symptoms when any foreign body has entered into the earhasincreasedaftertrainingin comparisontotheones beforetraining.Thisincreasewasstatisticallyinsignificant (p>0.05).
Discussion
The findingsobtained in thisstudy showthat the training aboutFBAgiventothepupilsinthedepartmentforchildren developmenthasleadtoanincreaseintheknowledgelevel oftheschoolchildren.
In order to protect children from FBA the individuals responsibleforchildcaremustbetrained.Theyhavetobe trainedindividuallyoringroupsregardingthemeasuresto betakenincase ofsituationscreatingariskforaspiration
accordingtotheirdevelopmentalageandthemeasuresto betakeninordertoavoidaspiration.11,15Inthestudycarried
outbyC¸elikandArıkanitwasreportedthatthe participa-tionrateofhighschoolanduniversitypupilsislow(8.2%).11
Bölükbas¸et al. reported in their study that 12.7% of the pupils received first aid training.10 Our study is revealing
that theFBAseminar and courseparticipationrate is low (1%), andthus inline withthe literaturethereis training necessityinthisregard.
In reported studies it is stated that FBA is one the majorreasons leadingtomorbidity andmortalityin pedi-atricagegroupsandthatFBAismainlyidentifiedbetween the age group of 0 and 3.5,7,16 In ourstudy it was
deter-mined that after relevant training, the number of pupils knowingtheagefactorimportanceinFBAincreased signif-icantly(p<0.05)(Table1).Webelieved thatthisfactwas duetotheperformedtraining.
Ifaforeignbodyentertheearcanal,nose and respira-torytract,itisimportanttoknowthecharacteristicsofthe foreign body (drilling-cutting,cylindrical, legume, insect) beforeitsremoval.Inaddition,itisreportedthatthemost frequentsymptomsinFBAareasfollows;suddenasphyxia during alimentation or playing with toys, bruising, cough and rattle.17---19 In ourstudy therewas an increase of the
Table3 Comparisonoffirst-aidknowledgelevelsofstudentsincaseofFBA(nose---ear)beforeandafterthetraining.
Beforethetraining Afterthetraining Statisticalanalysis 11th---12thgrade 11th---12thgrade
First-aidknowledgelevel Total(%) Total(%)
Theappearingsymptomsincaseofaspiratedbodyinnose
Knowing 27 67 p=0.000b
Notknowing 73 33
p=0.096a p=0.289a
Firstaidinterventionincaseofaspiratedbodyinnose
Knowing 27 67 p=0.000b
Notknowing 73 33
p=0.096a p=0.289a
Theappearingsymptomsifanyforeignbodyhasenteredintotheear
Knowing 87 90 p=0.684b
Notknowing 13 10
p=0.260a p=0.384a
Firstaidinterventionincaseofaspiratedbodyinear
Knowing 2 27 p=0.000b
Notknowing 98 73
p=0.932a p=0.096a
First-aidinterventionincaseofsharpedobjectissteepedinear
Knowing 75 87 p=0.023b
Notknowing 25 13
p=0.298a p=0.209a
First-aidinterventionincaseofalegumestuckinear
Knowing 23 48 p=0.000b
Notknowing 77 52
p=0.070a p=0.153a
First-aidinterventionincaseofaninsectstuck
Knowing 48 64 p=0.048b
Notknowing 52 36
p=0.860a p=0.973a
FBA,ForeignBodyAspiration.
a Chi-square. b McNemartest.
natureof theaspirated objectin FBAandbeingawareof theFBAsymptoms(p<0.05)(Table1).Theknowledgeabout thisissueaftertrainingisanimportantreality intermsof childhealth.Furthermoreinourstudyitwasseenthatthe numberofpupilsknowingthesymptomsin caseof partial andcompleteobstructionofrespiratorytracthasincreased aftertraining(p<0.05)(Table1).Thefactthatthe major-ityofpupilswereawareofthesesymptomsaftertrainingis significantintermsofprovidingfirstaidtochildren.
Astheaspiratedforeignbodymayirritatethenose,ear andrespiratorytractor thebacteria onforeignbodymay causean infectionBren(2005) emphasizes consult a doc-tor necessarily after the foreign body removal.20 It is an
encouragingfindingthatthenumberofpupilsbeingaware of consulting a doctor after the foreign body has been removed increased after training(p<0.05) (Table 1). Our studyshowedthatalmost (98%)allpupilsknew thephone numbertocallincaseofemergencybeforetrainingandall aftertraining(Table1).Itmaybeduetothefactthatthey areconstantlyfacingsuchsituationsintheirdailylife.
According to the literature, if the aspirated foreign body can be seen in the respiratory tract, the action of removing the foreign body with the index finger can causedisplacement of the foreignbody furtherdown the pharyngeal-trachealpassageincaseofbabiesandchildren, thereforeit isemphasized toperformthismaneuver with thelittlefingerinstead.19---21Theincreaseof28%of
aware-ness of first aid intervention, when an aspirated foreign isseen inthe respiratory tract,and 23%of people know-ingfirstaidinterventioniftherespiratorytractispartially obstructedafter-trainingleadustoconcludethatitwasa resultofthe obtained training(p<0.05)(Table 2).As the firstaidapplicationshouldbeknownbyallpupilswhowill performthefirstaid,theincreaseofknowledgeinrelation withthis issue is an important findingin terms of having achievedthetrainingpurpose.
threateningconsequences. Ourstudydemonstratedthat thenumberof pupilsknowingthe firstaid interventionin caseoftotalobstructionofrespiratorytracton<1yearand >1 year old children increased after training in compari-sontothebeforetrainingstatus(p<0.05)(Table2).Asthe appliedfirstaidmethodislifesaving,itisessentialforchild developmentdepartmentgraduatestohavethisknowledge. Furthermoreitwasseenthatbeforetrainingnopupilknew thefirstaidinterventionifthechildisunconsciousandhas aspiratedaforeignbody,itwas16%after-training(Table2). Itisthoughtthattheincreaseinnumberofpupilsanswering correctlyarisesfromtheprovidedtraining.
Ifanyforeignbodyentersthenose,thefollowing symp-tomscan be seen: nosebleeds, breathingdifficulties, oral breathing,nasalspeech,sneezing,nasalpain;ifthe aspi-ratedbodyremainsforalong timeinthenose,symptoms likepurulent bloody nasaldischarge mayappear.21---23 It is
emphasized that if the aspirated foreign body is not the resultof drillingor cutting,the patientshouldbe encour-agedtoclosehis/hernoseandblowstronglywithoutdeep inhalationbeforeblowing,iftheobjectdoesnotexit,the patientshouldbebroughttoahealthfacilitywithout inter-veningwithtools like tweezersor pliers.11,23 To carryout
theseapplicationsincorrectlyposesathreattothechild’s firstaidinterventionimportance.Inordertobeableto per-formthefirstaidinterventionearlytheindividualslooking afterthechildshouldknowthesesymptomsandtheproper firstaid intervention. In our study, we observed that the numberofpupilsknowingthesymptomsincase offoreign bodyenteringintothenoseandtherelatedfirstaid inter-ventionincreasedaftertraining,whichisdesirable(p<0.05) (Table3).
Ifanyforeignbodyhasenteredintotheear,thiscanlead topain,drainageandhearingloss.21,23Iftheenteredforeign
bodycanbeseenintheearcanal,itshouldnotberemoved withtoolsliketweezers andpliers,rathertheheadofthe individualshouldbeturnedtothesideanddownortheouter earshouldbepulledoutwardsinordertoremovetheobject, iftheobjectdoesnotexit,thepatientshouldbebroughtto ahealthfacility.11,23
Itisencouragingthatthenumberofpupilsknowingthe symptomsincase offoreignbody enteringthe earis high (87%). In our study,an increase has been observed after training (p>0.05) (Table 3). Additionally, the number of pupilsknowingthefirstaidinterventioniftheforeignobject canbe seen inthe earcanal increased25% after training (p<0.05)(Table3).Furthermore,aftertraining,therewas anincreaseinthenumberofpupilswhoknewthefirstaid interventionifadrillingobject,alegumeoran insecthas enteredthe ear(p<0.05)(Table3). Thisresultshows the effectivenessofthetraining.
Conclusion
VisualpresentationandtrainingonmodelsrelatedtoFBA
hasledtoanincreaseintheknowledgelevelofpupils.Based ontheseresults,itcanbeproposedthatnursesshouldtrain familiesandindividualsresponsibleforchildcareregarding protection from FBA and first aid intervention at regular intervals and standardize these trainings, create training
modelsconcerningthisissueandconductjointprojectswith theMinistryofNationalEducationandMinistryofHealth.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
OzakarAkcastudydesign,manuscriptpreparationand anal-ysis.Guven,Goyhan,Kaya,Mercandatacollection.
References
1.FerraiLR.Thepediatricairway:anatomy,challenges,and solu-tions.In: MasonKP,editor.Pediatric sedationoutside ofthe operatingroom.2nded.NewYork:Springer;2015.p.95---109. 2.PassàliD,LaurielloM,BellussiL,PassaliGC,PassaliFM,
Gre-gori D.Foreignbodyinhalationin children:an update.Acta OtorhinolaryngolItal.2010;30:27---32.PMCID:PMC2881610. 3.AltkornR,ChenX, MilkovichS,StoolD,RiderG, Bailey CM,
etal.Fatalandnon-fatalfoodinjuriesamongchildren(aged 0---14years).IntJPediatr Otorhinolaryngol. 2008;72:1041---6, http://dx.doi.org/10.1016/j.ijporl.2008.03.010.
4.Saki N, Nikakhlagh S, Rahim F, Abshirini H. Foreign body aspirations in Infancy: a 20-year experience.Int J MedSci. 2009;6:322---8.PMCID:PMC2764343.
5.Singh H, ParakhA. Tracheobronchialforeign body aspiration in children. Clin Pediatr (Phila). 2014;53:415---9, http://dx. doi.org/10.1177/0009922813506259.
6.TokarB,OzkanR,IlhanH.Tracheobronchialforeignbodiesin children:importanceofaccuratehistoryandplainchest radio-graphyindelayedpresentation.ClinRadiol.2004;59:609---15. PMID:15208067.
7.Chew HS, Tan HKK. Airway foreign body in children. IJCM. 2012;3:655---60,http://dx.doi.org/10.4236/ijcm.2012.37117. 8.Güzel A, Paksu S¸. Foreign body aspiration in children
and adults. J Exp Clin Med. 2013;30:81---5, http://dx.doi. org/10.5835/jecm.omu.30.s1.012.
9.Despres N, Lapointe A, Quintal MC, Arcand P, Giguere C, Abela A. 3-Year impact of a provincial choking prevention program. J Otolaryngol. 2006;35:216---21, http://dx.doi.org/ 10.2310/7070.2005.0014.
10.Bölükbas¸N,KahramanAN,KaramanY,KalaycıG.Orduprovince girls’ high school’s last year students children development department, their knowledge level related to the first aid applications. Anadolu Hems¸irelik ve Sa˘glık Bilimleri Dergisi. 2007;10:52---9.
11.C¸elik N, Arikan D. The effect of the training given to the child development students about foreign body aspira-tion upon their knowledge levels. Int J Pediatr Otorhino-laryngol.2013;77:1811---7,http://dx.doi.org/10.1016/j.ijporl. 2013.08.010.
12.Paksu S, Paksu MS, Kilic M, Guner SN, Baysal K, Sancak R, et al. Foreign body aspiration in childhood: evaluation of diagnosticparameters. Pediatr Emerg Care. 2012;28:259---64, http://dx.doi.org/10.1097/PEC.0b013e3182494eb6.
13.ChinskiA,FoltranF,GregoriD,PasalliD,BelussiL.Nasalforeign bodies:theexperienceoftheBuenosAirespediatric otolaryn-gology clinic. Pediatr Int. 2011;53:90---3, http://dx.doi.org/ 10.1111/j.1442-200X.2010.03176.x.
PediatrOtorhinolaryngol.2011;75:1322---6,http://dx.doi.org/ 10.1016/j.ijporl.2011.07.027.
15.OzdemirC,UzünI,SamB.Childhoodforeignbodyaspiration inIstanbul,Turkey. ForensicSciInt.2005;153:136---41.PMID: 16139101.
16.HiguchiO,AdachiY, IchimaruT,AsaiM,KawasakiK.Foreign bodyaspirationinchildren:anationwidesurveyinJapan.IntJ PediatrOtorhinolaryngol.2009;73:659---61,http://dx.doi.org/ 10.1016/j.ijporl.2008.12.026.
17.KadishH.EarandNoseForeignBodies:itisallaboutthetools. ClinPediatr(Phila).2005;44:665---7.PMID:16211189.
18.LalaniSB.ForeignBodyAspiration:alife-threateningsituation. JPerianesthNurs.2015;30:50---3, http://dx.doi.org/10.1016/ j.jopan.2014.02.004.
19.Louie MC, Bradin S. Foreign body ingestion and aspiration. Pediatr Rev. 2009;30:295---301, http://dx.doi.org/10.1542/ pir.30-8-295.
20.Bren L. Prevent your child from choking. FDA Consum. 2005;39:27---9.PMID:16419289.
21.WongDL,HockenberryJM.Nursingcareofinfantsandchildren. St.Louis:MosbyCompany;2003.p.1376.
22.Acello B, Hegner BR. Nursing assistant: a nursing process approach:response to basicemergencies: childwithforeign body airway obstruction. USA: Cengage Learning; 2014. p. 984---1000.