R E S E A R C H A R T I C L E
Proteinuria in adults with sickle-cell disease: the role
of hydroxycarbamide(hydroxyurea) as a protective agent
Geraldo B. Silva Junior•Ana Patrı´cia F. Vieira •Amanda X. Couto Bem•
Marı´lia P. Alves•Gdayllon C. Meneses•Alice M. C. Martins•Sonia M. H. A. Arau´jo•
Alexandre V. Libo´rio•Elizabeth F. Daher
Received: 9 February 2014 / Accepted: 30 April 2014 / Published online: 17 June 2014 Koninklijke Nederlandse Maatschappij ter bevordering der Pharmacie 2014
Abstract BackgroundRenal abnormalities are often seen in sickle cell disease (SCD).ObjectiveTo investigate the role of hydroxycarbamide as a protective agent in sickle cell nephropathy. Setting Patients with SCD followed at a Hematology outpatients clinic.Methods Prospective study with 26 SCD patients. Renal function evaluation was per-formed and a comparison between patients and control group was done. Patients using hydroxycarbamide were compared to those not taking this drug. Main outcome measure Effect of hydroxycarbamide on renal function. Results Patients mean age was 32.1±9.9 years, and 16 (61 %) were males. Glomerular hyperfiltration was found in nine patients with SCD (34.6 %). GFR\60 mL/min/
1.73 m2was observed in three cases (11.5 %). Microalbu-minuria (30–300 mg/day) was found in seven cases (27 %) and macroalbuminuria ([300 mg/dia) in one patient
(3.8 %). All patients had urinary concentrating deficit, and inability to acidify urine was found in ten cases (38.4 %). The comparison of patients according to the use of hydroxycarbamide showed lower levels of serum creatinine in those using the drug (0.6±0.1 vs. 0.8±0.3 mg/dL,
p =0.03), as well as lower levels of 24 h-proteinuria (226 ±16 vs. 414±76 mg/dL,p=0.0001), but not mi-croalbuminuria (79±15 vs. 55±86 mg/dL, p =0.35). ConclusionSCD is associated with important renal abnor-malities. Hydroxycarbamide seems to protect kidney func-tion in SCD by decreasing proteinuria but not microalbuminuria.
Keywords HydroxycarbamideKidney disease
ProteinuriaRenal function testsSickle cell disease
Tubular dysfunction
Impact of findings on practice statements
• Patients with sickle cell disease (SCD) using hydrox-ycarbamide present lower levels of creatinine and proteinuria.
• Hydroxycarbamide may have a role in protecting renal function in SCD, mainly due to its possible effect on decreasing proteinuria.
Introduction
Sickle-cell disease (SCD) is the most common hereditary hematological disease in the world, its prevalence varying according to the geographical area [1]. Renal involvement in SCD was first reported at the beginning of twentieth century [2], and there are reports of renal inability to concentrate and acidify urine in SCD patients [3,4]. Other renal complications include haematuria, microalbuminuria, increase in urinary retinol-binding protein, b 2-microglob-ulin and endothelin-1, renal neoplasia, renal papillary necrosis and rhabdomyolysis [5–7].
G. B. Silva JuniorA. P. F. VieiraA. X. Couto Bem M. P. AlvesA. V. Libo´rioE. F. Daher
Department of Internal Medicine, School of Medicine, Federal University of Ceara´, Rua Vicente Linhares, 1198, Fortaleza, Ceara´ CEP 60135-270, Brazil
G. B. Silva Junior (&)S. M. H. A. Arau´jo
Health Sciences Center, School of Medicine and Master in Collective Health, University of Fortaleza, Fortaleza, Ceara´, Brazil
e-mail: [email protected]
G. C. MenesesA. M. C. Martins
Sickle-cell disease (SCD) treatment includes chronic red blood cell transfusions, the use of hydroxycarbamide, bone marrow and stem cell transplantation [8]. The prognosis of patients with SCD has improved significantly over the last few decades, due to widespread screening for the disease in newborns in many parts of the world [8]. Nowadays the main causes of mortality in SCD are cardiovascular diseases. The majority of deaths occur in the context of chronic organ damage, including chronic kidney disease, chronic conges-tive heart failure and chronic debilitating stroke [8].
The use of drugs that stimulate the production of foetal haemoglobin (HbF) is known to be beneficial in SCD. Hydroxycarbamide, a cytotoxic drug, increases the produc-tion of HbF and is associated with improved survival [9]. The benefits of hydroxycarbamide in SCD include a decrease in vaso-occlusive events, pain crisis, greater intervals between pain episodes, and fewer thoracic syndrome episodes. In addition there is, a reduction in the need for transfusions and in the number of hospital admissions [9,10]. Despite all these benefits the drug is still under prescribed, particularly in children [11]. Additional mechanisms of action for HbF induction have been proposed for hydroxycarbamide, including free radical formation, iron chelation, activation of soluble guanylyl-cyclase, and direct nitric oxide (NO) pro-duction [12]. It also decreases reticulocytes count and reduces surface expression of adhesion receptors [12].
According to Ware [12], an ideal therapeutic intervention for SCD would fulfill the following characteristics: single-agent, inexpensive, orally administered, once-daily dosing; increases HbF and total Hb, reduces WBC and reticulocytes, and lowers LDH; ameliorates anaemia, leads to fewer vaso-occlusive events and hospitalisations, decreases haemolysis; works in all age groups, prevents acute events and chronic organ dysfunction; benefits continue over time without medication resistance or tolerance; few short-term toxicities that might limit adherence, wide therapeutic index; no major short-term toxicities, plus no known long-term sequelae or complications of therapy. These characteristics are all demonstrated by hydroxycarbamide, making a strong argu-ment for its use in SCD treatargu-ment and possible prevention of major complications, including renal dysfunction [12].
Aim of the study
The aim of this study is to investigate the role of hydrox-ycarbamide on renal function in sickle cell nephropathy.
Methods
This is an observational cohort study consisting of con-secutive patients with clinical and laboratory diagnosis of
SCD undergoing consultation in a public health service in the Northeast Region of Brazil from December 2010 to June 2012. All patients were homozygous for HbS. Exclusion criteria were: patients under 18 years or older than 65 years, use of nephrotoxic drugs, hypertension (systolic blood pressure C140 or diastolic blood pressure C90 mmHg), diabetes mellitus, chronic blood transfusion or transfusion in the last 6 months, and other conditions which could affect kidney function. The protocol of this study was approved by the Ethical Committee of the Walter Cantidio University Hospital, Federal University of Ceara, Fortaleza, Brazil. Patients were included in the study after signing the informed consent form.
All patients had a definitive diagnosis of SCD with hemoglobin electrophoresis. All of them were homozygous and presented haemoglobin S (HbSS). All patients were treated with folic acid 5 mg/day and 12 with hydroxycar-bamide 1 g/day. Patients’ treatment was conducted by the assistant haematologist according to standard guidelines [13]. Patients included in the study were not using any other medication. A comparison of the studied parameters was done between hydroxycarbamide and non-hydroxy-carbamide groups.
Microalbuminuria was determined by 24 h urine col-lection and was considered abnormal with values between 30 and 300 mg/day. Macroalbuminuria was considered as urine albumin[300 mg/day.
Estimated GFR was obtained by CKD-EPI—Chronic Kidney Disease Epidemiology Collaboration [14]. All patients were considered non-black due to great miscege-nation of the Brazilian population (i.e. mixing of different racial groups). Glomerular hyperfiltration was considered as GFR[120 mL/min/1.73 m2.
All patients underwent food and water deprivation for 12 h. Urinary concentration ability was evaluated through the ratio between urinary and serum osmolality (Uosm/Posm) after 12 h water deprivation. Urinary acidification was evaluated through the measure of urinary pH before and after administration of oral CaCl2 2 mEq/kg, with an interval of 4 h (T0and T4), CaCl2was used as it is more tolerable than ammonium chloride (HN4Cl) [7]. Acidifi-cation defect was determined by the inability to decrease UpHto\5.5 after the administration of the alkaline load, as
described before.
by colorimetric glucose oxidase method (Labtest). The results were expressed in mg/dL. Arterial pH and bicar-bonate (HCO3-) were determined through ‘‘blood gas analyzer’’ machine (Chiron Diagnostic 238—Bayer). The results were expressed in mEq/L for bicarbonate. Urinary pH (UpH) was measured by pHmeter Digital pG1000, model GEHAKALT. Urinary osmolality was determined by the pressure steam technique in osmometer model 5100C (Wescor Inc., USA). The results were expressed in mOsm/kg H2O. Albuminuria was measured through im-munoturbidimetry methods, using Tina-quantkit (Roche) and the results were expressed in mg/day.
Fisher’s exact test andv2test were used to analyse allele frequencies in the patient group. Differences between two independent variables were evaluated using Student’sttest or Mann–Whitney test as appropriate. Data were expressed as mean±SD, and p\0.05 was considered statistically
significant. The SPSS software for Windows, release 10.0 (SPSS Inc., Chicago, Ill., USA) was used in all analysis.
Results
Of 150 patients with SCD, 26 agreed to participate to the study. The mean age was 32.1±9.9 years (range 20–62 years), and 16 (61 %) were males. All patients had sickle cell anemia (HbSS) and a mean HbF of 10.9±6.9 % at the time of the last medical consultation. Patients had started using Hydroxycarbamide from 1 to 2 years ago (mean 17±4 months). Patients’ demographic characteris-tics are summarised in Table1.
Glomerular hyperfiltration was found in nine patients with SCD (34.6 %). GFR\60 mL/min/1.73 m2 was
observed in three cases (11.5 %). Microalbuminuria (30–300 mg/day) was found in seven cases (27 %) and
macroalbuminuria ([300 mg/day) in one patient (3.8 %).
All patients presented urinary concentrating deficit, and inability to acidify urine was found in five cases (19.2 %). The comparison of patients according to the use of hydroxycarbamide showed lower levels of serum creatinine in those using the drug (0.6±0.1 vs. 0.8±0.3 mg/dL, p =0.03), as well as lower levels of 24 h-proteinuria (226 ±16 vs. 414±76 mg/dL, p=0.0001). There was no difference regarding the other study parameters (Table2).
Discussion
Sickle cell disease (SCD) is a public health problem pre-senting important morbidity and mortality with high prevalence in some parts of Brazil and other developing countries [15]. One of the most important interventions in SCD is the use of hydroxycarbamide. Recent studies have shown its benefits not only in the improvement of hae-matological parameters but also in the treatment of dif-ferent organ dysfunctions including kidney abnormalities [16].
A recent study with 23 children with SCD using hydroxycarbamide showed that after 3 years of treatment, glomerular filtration rate, measured by 99mTc-DTPA, decreased significantly from 167±46 to 145±27 mL/ min/1.73 m2 (p=0.016), and this decrease was signifi-cantly associated with increase in foetal hemoglobin (p =0.042). Microalbuminuria, however, did not change significantly [17]. Alvarez et al. [18], showed, in the BABY-HUG study, that hydroxycarbamide use was asso-ciated with improvement in renal concentration ability, but had no effect on glomerular filtration rate. There was no difference between patients using and not using hydroxy-carbamide regarding renal concentrating and acidification defects. In the present study the levels of proteinuria were lower among patients using hydroxycarbamide but the levels of microalbuminuria showed no significant differ-ence. This could be due to tubular proteinuria.
Treatment for reducing proteinuria in SCD can be done with angiotensin converting enzyme inhibitors (ACEi) or angiotensin-II receptors blockers (ARB), as is common practice in other proteinuric nephropathies [19]. However, a recent meta-analysis found no significant difference between the use of captopril and placebo in the reduction of microalbuminuria in SCD [20]. It is possible that hydrox-ycarbamide also prevents the progression of kidney disease in SCD by decreasing the levels of proteinuria and allevi-ating glomerular hyperfiltration [21] but its effect on renal function still needs to be investigated in larger randomised-controlled trials. In the present study, patients using hydroxycarbamide presented lower levels of creatinine and Table 1 Comparison of demographic and clinical characteristics of
patients with SCD according to the use of hydroxycarbamide
Hydroxycarbamide (n=12)
No-hydroxycarbamide (n=14)
p
Age (years) 29.3±7.4 34±11 0.19
Gender
Male 4 (34 %) 6 (43 %) 0.70
Female 8 (66 %) 8 (57 %)
SBP (mmHg) 118±15 116±5.7 0.64
DBP (mmHg) 70±11 76±5.7 0.08
Weight (kg) 58±11 58±11 1.0
Foetal Hb (%) 11±6.8 8.7±4.8 0.32
Data are shown as mean±SD or numbers with percentages in brackets
SBPsystolic blood pressure,DBPdiastolic blood pressure
proteinuria, which suggests a protective factor regarding renal function in SCD.
The possible mechanisms for the renal-protective action hydroxycarbamideinclude the increase in HbF, which would increase oxygenation in renal tissue, including renal medulla, which in turn would decrease the vaso-occlusive events within renal circulation. The lack of influence of hydroxycarbamide in GFR observed in our study suggests that the drug does not act on glomerulus haemodynamics. The effect on decreasing proteinuria could point to an improvement in renal tubular function, since proteinuria in SCD could have a tubular origin. Tubular proteinuria can be more pronounced than glomerular proteinuria in SCD. Recent studies evidence important tubular impairment in SCD without important glomerular changes [22], which
justifies the finding that hydroxycarbamide decreases pro-teinuria without significantly influencing glomerular fil-tration rate.
Conclusion
In conclusion, SCD is associated with important renal abnormalities. Urinary concentrating and acidification deficits are found in a significant number of cases, as well as proteinuria. Hydroxycarbamide seems to protect kidney function in SCD by decreasing proteinuria. Further studies, as randomised controlled trials are required to better establish the benefits of hydroxycarbamide as a renal pro-tecting agent.
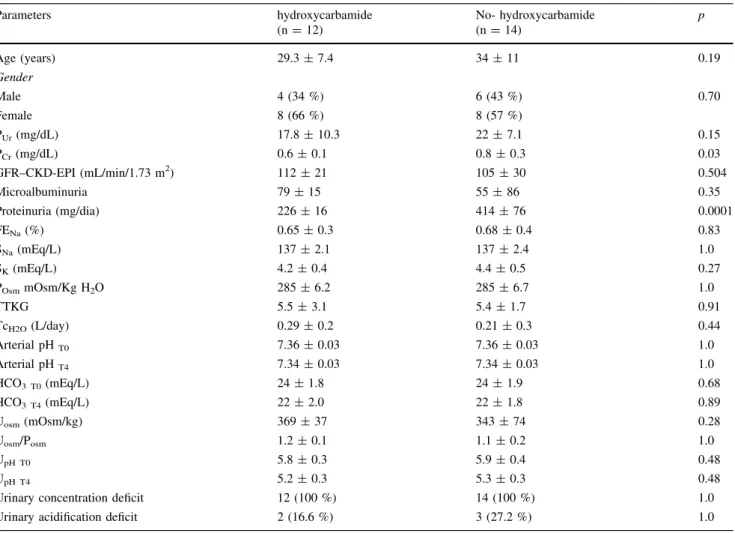
Table 2 Comparison of renal function parameters among patients with SCD according to the use of hydroxycarbamide
Parameters hydroxycarbamide No- hydroxycarbamide p
(n=12) (n=14)
Age (years) 29.3±7.4 34±11 0.19
Gender
Male 4 (34 %) 6 (43 %) 0.70
Female 8 (66 %) 8 (57 %)
PUr(mg/dL) 17.8±10.3 22±7.1 0.15
PCr(mg/dL) 0.6±0.1 0.8±0.3 0.03
GFR–CKD-EPI (mL/min/1.73 m2) 112±21 105±30 0.504
Microalbuminuria 79±15 55±86 0.35
Proteinuria (mg/dia) 226±16 414±76 0.0001
FENa(%) 0.65±0.3 0.68±0.4 0.83
SNa(mEq/L) 137±2.1 137±2.4 1.0
SK(mEq/L) 4.2±0.4 4.4±0.5 0.27
POsmmOsm/Kg H2O 285±6.2 285±6.7 1.0
TTKG 5.5±3.1 5.4±1.7 0.91
TcH2O(L/day) 0.29±0.2 0.21±0.3 0.44
Arterial pHT0 7.36±0.03 7.36±0.03 1.0
Arterial pHT4 7.34±0.03 7.34±0.03 1.0
HCO3 T0(mEq/L) 24±1.8 24±1.9 0.68
HCO3 T4(mEq/L) 22±2.0 22±1.8 0.89
Uosm(mOsm/kg) 369±37 343±74 0.28
Uosm/Posm 1.2±0.1 1.1±0.2 1.0
UpH T0 5.8±0.3 5.9±0.4 0.48
UpH T4 5.2±0.3 5.3±0.3 0.48
Urinary concentration deficit 12 (100 %) 14 (100 %) 1.0
Urinary acidification deficit 2 (16.6 %) 3 (27.2 %) 1.0
Data are shown as mean±SD or numbers with percentages in brackets
PCrplasma creatinine,PUrplasma urea,UProt24 h-urinary protein,GFRglomerular filtration rate,CKD-EPIchronic kidney disease epide-miology collaboration,FENasodium excretion fraction,SNaserum sodium,POsmplasma osmolality,TTKGtranstubular potassium gradient, TcH2Osolute free water reabsorption,Uosmurinary osmolality,U/Posmratio urinary and plasmatic osmolality,UpH T0urinary pH in T0,UpH T4 urinary pH in T4
Acknowledgments We are very grateful to the team of physicians, residents, medical students, and nurses from the Walter Cantı´dio University Hospital, Federal University of Ceara´, for providing technical support for the development of this research and for the exceptional assistance provided to the patients.
Funding Prof. E.F.D., A.M.C.M. and A.B.L. received a grant from the Brazilian Research Council (Conselho Nacional de Desenvolvi-mento Cientı´fico e Tecnolo´gico—CNPq, bolsa de produtividade em pesquisa).
Conflicts of interest None.
References
1. Loureiro MM, Rozenfeld S. Epidemiology of sickle cell disease hospital admissions in Brazil. Rev Sau´de Pu´blica. 2005;39(6):943–9. 2. Josephs H. Clinical aspects of sickle cell anemia. Bull Johns
Hopkins Hosp. 1928;43:397–8.
3. Keitel HG, Thompson D, Itano HA. Hyposthenuria in sickle cell anemia: a reversible renal defect. J Clin Invest. 1956;35(9): 998–1007.
4. Crosley AP, Strickland WH. Renal function in sickle cell ane-mia—a case report and review of the literature. J Natl Med As-soc. 1961;53(1):39–40.
5. Tsaras G, Owusu-Ansah A, Boateng FO, Amoateng-Adjepong Y. Complications associated with sickle cell trait: a brief narrative review. Am J Med. 2009;122(6):507–12.
6. Abo-Zenah H, Moharram M, El Nahas AM. Cardiorenal risk prevalence in sickle cell hemoglobinopathy. Nephron Clin Pract. 2009;112(2):c98–106.
7. Da Silva GB Jr, Libo´rio AB, Daher Ede F. New insights on pathophysiology, clinical manifestations, diagnosis, and treat-ment of sickle cell nephropathy. Ann Hematol. 2011;90(12): 1371–9.
8. Wang WC. Sickle cell anemia and other sickling syndromes. In: Greer JP, Foerster J, Rodgers GM, Paraskevas F, Glader B, Arber DA, Means Jr RT. Wintrobe’s clinical hematology, 12th edition. Philadelphia: Lippincott Williams and Wilkins, p. 1038–1082, 2009. ISBN: 978-0-7817-6507-7
9. Saunthararajah Y, Vichinsky EP. Sickle cell disease—clinical features and management. In: Hoffman—Hematology: basic
principles and practice. Oxford: Churchill Livingstone, 5th edn, p. 577–601, 2008. ISBN: 978-0443067150.
10. Rees DC, Williams TN, Gladwin MT. Sickle-cell disease. Lancet. 2010;376(9757):2018–31.
11. Brandow AM, Panepinto JA. Hydroxycarbamide use in sickle cell disease: the battle with low prescription rates, poor patient compliance and fears of toxicities. Expert Rev Hematol. 2010;3(3):255–60.
12. Ware RE. How I use Hydroxycarbamide to treat young patients with sickle cell anemia. Blood. 2010;115(26):5300–11. 13. Brawley OW, Cornelius LJ, Edwards LR, Northington Gamble
V, Green BL, Inturrisi C, et al. National institutes of health consensus development conference statement: hydroxycarbamide treatment for sickle cell disease. Ann Intern Med. 2008;148(12): 932–8.
14. Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF III, Feldman HI, et al. A new equation to estimate glomerular fil-tration rate. Ann Intern Med. 2009;150(9):604–12.
15. Lobo C. Sickle cell disease—a serious problem for public health worldwide. Rev Bras Hematol Hemoter. 2010;32(4):280–1. 16. Bartolucci P, Galacte´ros F. Clinical management of adult
sickle-cell disease. Curr Opin Hematol. 2012;19(3):149–55.
17. Aygun B, Mortier NA, Smeltzer MP, Shulkin BL, Hankins JS, Ware RE. Hydroxycarbamide treatment decreases glomerular hyperfiltration in children with sickle cell anemia. Am J Hematol. 2013;88(2):116–9.
18. Alvarez O, Lopez-Mitnik G, Zilleruelo G. Short-term follow-up of patients with sickle cell disease and albuminuria. Pediatr Blood Cancer. 2008;50(6):1236–9.
19. Fitzhugh CD, Wigfall DR, Ware RE. Enalapril and hydroxycar-bamide therapy for children with sickle nephropathy. Pediatr Blood Cancer. 2005;45(7):982–5.
20. Sasongko TH, Nagalla S, Ballas SK. Angiotension-converting enzyme (ACE) inhibitors for proteinuria and microalbuminuria in people with sickle cell disease. Cochrane Datab Syst Rev. 2013;3:009191.
21. Aleem A. Proteinuria in adult Saudi patients with sickle cell disease is not associated with identifiable risk factors. Saudi J Kidney Dis Transpl. 2010;21(5):903–8.