SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
article
Biomechanical
evaluation
of
the
long
head
of
the
biceps
brachii
tendon
fixed
by
three
techniques:
a
sheep
model
夽
Carlos
Henrique
Ramos
∗,
Júlio
Cezar
Uili
Coelho
UniversidadeFederaldoParaná,Curitiba,PR,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received22February2016 Accepted18March2016
Availableonline30December2016
Keywords:
Bicepsbraquii
Humerus Biomechanic Tendons
a
b
s
t
r
a
c
t
Objective:Toevaluatethebiomechanicalpropertiesofthefixationofthelongheadofthe bicepsbrachiiintothehumeralbonewithsutureanchors,interferencescrew,andsofttissue suture,comparingstrength,highesttractionload,andtypesoffixationfailure.
Methods:Thirtyfresh-frozensheepshoulderswereused,separatedintothreegroupsoften foreachtechnique.Afterfixation,thetendonsweresubjectedtolongitudinalcontinuous loading,obtainingload-to-failure(N)anddisplacement(mm).
Results:The mean load-to-failure for suture anchors was 95±35.3N, 152.7±52.7N for interferencescrew,and104.7±23.54Nforsofttissuetechnique.Therewasastatistically sig-nificantdifference(p<0.05),withinterferencescrewdemonstratinghigherload-to-failure thansutureanchorfixation(p=0.00307)andsofttissue(p=0.00473).Thestrengthof inter-ferencescrewwasalsosuperiorwhencomparedwiththeothertwomethods(p=0.0000127 andp=0.00000295,respectively).Therewerenodifferencesbetweensutureanchorsand softtissuetechniqueregardingload-to-failure(p=0.9420)andstrength(p=0.141).
Conclusion:Tenodesisofthelongheadofthebicepsbrachiiwithinterferencescrewwas strongerthanthesutureanchorsandsofttissuetechniques.Theothertwotechniquesdid notdifferbetweenthemselves.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Avaliac¸ão
biomecânica
da
fixac¸ão
do
tendão
da
cabec¸a
longa
do
bíceps
braquial
por
três
técnicas:
modelo
em
ovinos
Palavras-chave:
Bícepsbraquial Úmero
r
e
s
u
m
o
Objetivo:Avaliarbiomecanicamenteafixac¸ãodacabec¸alongadobícepsbraquialnoúmero comâncorasósseas,parafusodeinterferênciaesuturaempartesmolesecomparar resistên-cia,forc¸amáximadetrac¸ãoetiposdefalhanafixac¸ão.
夽
StudyconductedattheCentroUniversitário(UniBrasil),atthePontifíciaUniversidadeCatólicadoParaná,andattheUniversidade FederaldoParaná,Curitiba,PR,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](C.H.Ramos).
http://dx.doi.org/10.1016/j.rboe.2016.12.008
Biomecânica Tendões
Métodos: Foramusados30ombrosdeovinosfrescos,divididosemtrêsgruposdedezpara cadatécnica.Apósfixac¸ão,ostendõesforamsubmetidosatrac¸ãolongitudinalcontínuaaté falhadosistemaeobtiveram-seforc¸amáximadetrac¸ão(N)edeslocamento(mm).
Resultados: A forc¸a máxima de trac¸ão foi em média 95±35,3N para âncoras ósseas, 152,7±52,7Nparaparafusode interferênciae104,7±23,54Nparapartesmoles. Houve diferenc¸aestatisticamentesignificativa(p<0,05):oparafusodeinterferênciademonstrou forc¸amáximadetrac¸ãosuperioràsfixac¸õescomâncorasósseas(p=0,00307)epartesmoles (p=0,00473).Aresistênciacomparafusodeinterferênciatambémfoisuperioràdos out-rosdoismétodos(p=0,0000127ep=0,0000029,5respectivamente).Âncorasósseasepartes molesnãoapresentaramdiferenc¸as,tantoparaforc¸amáximadetrac¸ão(p=0,9420)quanto pararesistência(p=0,141).
Conclusão: Atenodesedacabec¸alongadobícepsbraquialcomparafusodeinterferência demonstramaiorresistênciaquandocomparadacomastécnicascomâncorasóssease partesmoles.Asduasúltimastécnicasnãodiferem.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Disordersofthelongheadofbicepsbrachiitendon(LHBBT)are frequentcausesofshoulderpain.Treatmentshouldbe conser-vative (analgesics, anti-inflammatories, and physiotherapy, among others); however, when conservative treatment is unsuccessful,surgeryisindicated.Therecommended proce-dureistenotomyofthelongheadofthebiceps(sectioning the tendonatthe level ofits insertion inthe glenoid cav-ity)withorwithouttenodesisofthelongheadofthebiceps (fixating the biceps tendoninto the bicipital groove ofthe humerus). Tenodesis has been suggested as advantageous over isolated tenotomy, as it maintains the length/tension ratioand theflexion andsupination strengthoftheelbow, preventing atrophy, pain at the site, and cosmetic defor-mity.Recentadvanceshaveallowedtenodesistobepreferably performedarthroscopically,which,despitepromotingresults similar toopen surgery, offersadvantagessuch assmaller surgical wound, lower post-operative pain, preservation of the deltoid muscle, and earlier return to activities, espe-ciallywhenassociatedwithsimultaneousrepairoftherotator cuff.1–3 Amongthearthroscopicfixationmethods,themost frequently used are bone anchors, interference screw (IS), and softtissue suturewithout the needforimplants.1,2,4–8 Earlypostoperativemobilizationoftheupperlimbis impor-tantforrecovery,butmayendangertenodesiswithpossible releaseofthetendon.Toavoidthisissue,thesystemthat pro-videsthehighestresistanceshouldbeused.Anotheraspect is the increased cost ofthe procedure when implants are used; soft tissue technique is cheaper. Identifying which method is more resistant would justify the use or non-useofimplants,definingthemostcost-effectivetechnique. Thereisnoconsensusintheliteratureregardingwhich fix-ation method is more resistant.9–24 This study aimed to comparethree techniquesforfixation oftheLHBBT inthe humerus(boneanchors,IS,andsofttissuesuture)regarding
resistance ofthe fixation, load-to-failure(LTF), and system failure.
Materials
and
methods
AfterapprovalbytheResearchEthicsCommitteeofthe Hospi-taldoTrabalhadorofUniversidadeFederaldoParaná,30fresh shoulder specimensfromskeletally immatureTexelsheep, agedbetweensixand12months,wereacquiredfroma spe-cialized company.Thespecimenswere frozenimmediately afterslaughterandwerekeptat−20◦Cuntil24hbefore
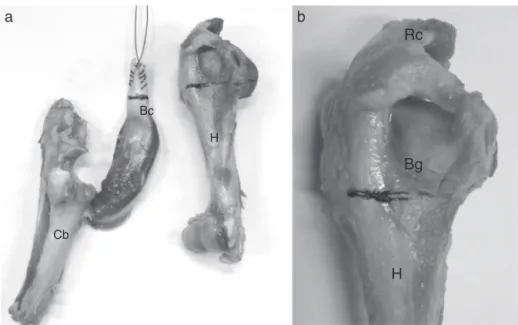
prepa-ration.Samples werethen thawed atroom temperatureto undergotenodesis.Sampleswerepreparedwithdissectionof thehumeralbone;onlythe bicepsand theanteriorportion oftherotatorcuffinsertedintothegreatertuberosityofthe humerus were preserved.Theproximal bicepstendon was sectionedattheglenoidlabrumintheupperportionofthe glenoidcavity(scapularbone),maintainingitsdistalinsertion into the cubitus bone(Fig.1).Thespecimens weredivided intothreegroupsoften,accordingtothetypeoftenodesis; tenpieceswerethawedatatime,withanintervalof15days betweeneachtest.
Tenodesiswithboneanchors
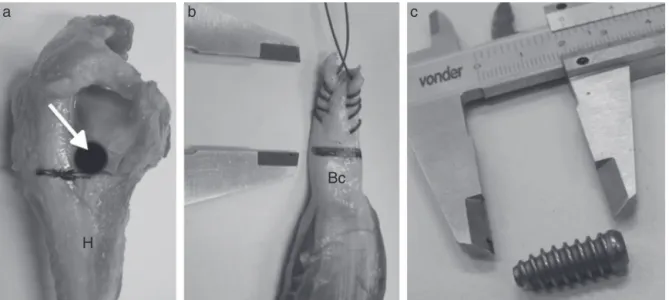
Aftertwoholesweremadeinthehumeralmetaphysealregion (bicipitalgroove),twoboneanchorscrews,madeoftitanium, withadiameterof4.0mm,positionedwithanEthibond2® suture(braided polyester)were inserted withadistanceof 5mmbetweenthem(Fig.2).Then,thebicepstendonwas fix-ated into thehumerus witha singlestitch ineach anchor (Fig.3).
Tenodesiswithinterferencescrew
Cb
Bc
H
Bg
H
b
a
Rc
Fig.1–Photographofthepartsobtainedbydissection;thedistalinsertionofthebicepsinthecubitusbone(a)andthe rotatorcufftothehumerus(b)weremaintained,Cb,cubitalbone;Bc,biceps;Bg,bicipitalgroove;H,humerus;Rc,rotatorcuff.
(7×20mm).Thefreeendofthetendonwasrepairedusing continuous suturewith Ethibond 2® and inserted into the humeralorificeforfixationwithIS,paralleltothetendonfibers (Figs.4and5).Duringscrewinsertion,thetendonwaskeptin tractionagainsttheoppositecortexthroughprior transfixa-tionoftherepairwirewithafenestratedsteelguidewireto keepitwithinthebonehole.
Bicepstenodesisinsofttissue
Thebicipitaltendonsuturewasmadeontheremaining por-tion oftherotator cuffthat wasmaintainedinthe greater tuberosityofthehumerus,withthreesimplestitchesusing Ethibond2®sutures(Fig.6).
MeasurementsweremadewithaVonder®precision metal-liccaliper (150mm-6′′). After surgicalpreparation, material
wassenttotheBiomechanicsLaboratoryoftheUniversidade TecnológicaFederaldoParaná(UTFPR)fortesting.
Foraxialtraction,theuniversalMTS810(100KN)hydraulic equipmentfortensiletestswasused,withasecondactuator
(MTS242.02)adaptedwithaloadcell(model661.19F-02,MTS SystemsCorporation,withacapacityof10KN,andappliedat aspeedof5mm/min.
Modelswerefittedsothatthetractiontobeexertedinthe longitudinaldirectioninrelationtotheaxesofthetendon andhumeruswouldsimulatethenormaldirectionof contrac-tionbythebiceps.Irondevicesweredevelopedandplacedon thetensileequipmenttofixatetheendsofthespecimen.At thetop,theulnarbonewassupportedonthisdeviceandthe tendonwaspassedthroughthecenterhole.Forlower stabi-lization,acylindricaladapterwasfixedonthetractiontable. Thispiecehadinteriorlateralperforationsforhumeral sta-bilization,withtwostrongsteelwiresofadiameter(5mm), cross-transfixated inthe metaphyseal region. Thedistance betweentheextremitiesvariedaccordingtothelengthofthe muscle/tendonpair.Forabetterfit,thelengthofthehumerus wascutatthemiddlethirdduringassembly(Fig.7).Withthe helpofMTS-TestStarIIsoftware,790.90,TestWorks–1994, graphicsindicatingtheLTF(N)weremade.LTFwasdefined
Bg
H Bc
Ba
Bg
b
a
H Bc
Fig.3–Drawing(a)andspecimenphotograph(b)showing thefixationtechniquewithboneanchors.Ba,bone anchors;Bc,biceps;Bg,bicipitalgroove;H,humerus.
astheforce requiredtobreakthe fixation(systemfailure), obtainedwithpeakofthecurve,representedbythevertical axisofthegraph.Thesystemwasconsideredtohavefailed whenitlosttensilestrength,whetherbytendonslipor loosen-ingorruptureofthefixation,evenincaseswithoutcomplete separationofthetendon-bonesystem.Thedislocationuntil failurewasrepresentedbythehorizontalaxis.Resistancewas calculatedbydividingtheLTFbythedislocation(Fig.8).
TheresultswerestatisticallyanalyzedwithKaplan–Meier non-parametricestimationofthesurvivalfunction.The95% confidenceintervalsfortheprobabilityofthesystemnot fail-inguntilacertainforce(LTFandresistance)werecomparedfor everymethod.Forquantitativeevidence,thelogrank signifi-cancetestwasusedandthep-valuewascalculated(significant atp<0.05).
Bg
Bg H
H
Bc
Bc Bc
Is Is
Is
b
a
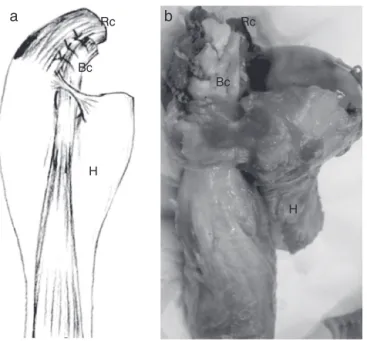
Fig.5–Drawing(a)andspecimenphotograph(b)showing thefixationtechniquewithinterferencescrew.Bc,biceps; Bg,bicipitalgroove;Is,interferencescrew;H,humerus.
ThetestsweredonewithMicrosoft® ExcelXPandOrigin 6.1Pro®programs.Forthestatisticalanalysisandadjustment ofthe reliability/survivalmodels, thestatistical softwareR, whichisopensource,wasused.
Results
TheLTF and resistanceresultsforthethreemethods, pre-sentedasmaximums,minimums,andmeans,aredescribed inTables 1and2. Thecentraldatavalues, dispersion,and possibleoutliersareshowninbox-plotgraphsforthesame variables(Fig.9).ThemeanLTFforthethreemethodswas: 95±35.3N(range50–156N) forboneanchors; 52.7±152.7N (57–212N)forIS;104.7±23.54N(75.9–145N)forsofttissues.In thetechniquewithboneanchors,failureoccurredmainlyat thejunctionofthesutureinthetendon(ninetests),withfiber tearinthelongitudinaldirectionwithoutreleaseofthebone
H
Bc
c
b
a
Rc Rc
Bc
Bc
H
H
a
b
Fig.6–Drawing(a)andspecimenphotograph(b)showing thefixationtechniqueinsofttissue.Bc,biceps;Rc,rotator cuff;H,humerus.
anchor(s)(Fig.10).Inonetest,asutureatthedistalanchor failed,andatendonrupturewasobservedinthesuture.In thetestswithIS,failureoccurredmainlyduetotendonslip (eighttests), andtherewere nocasesofimplant loosening (Fig.11).Intwocases,thefailureoccurredduetoarupture inthemyotendinousjunction,withoutlooseningoffixation. Alltestswithsofttissuefixationpresentedfailurebytendon slip;thesuturesinthebicepsandrotatorcufffibersremained intact. The Kaplan–Meier curves and the logrank p-values appliedtothethreemethodsstudieddemonstratedthatthe fixation withIS is significantly different(p<0.05) from the
200.00
150.00
100.00
50.00
0.00
36 000 41 000 46 000
Peak force
Actuator2 (mm) Dislocation (mm)
Traction force
51 000 56 000
Fig.8–Valuesrecordedforpeakforceanddisplacement untilsystemfailure.
othermethods,presentinghigherLTFwhencomparedwith fixationwithboneanchors(p=0.00307)andsofttissuesuture (p=0.00473).ISresistancewasalsosuperiortotheothertwo methods(p=0.0000127andp=0.00000295,respectively).Bone anchorsandsofttissuesuturedidnotdiffersignificantlyfor bothLTF(p=0.9420)andresistance(p=0.141).
Discussion
Tenodesisofthelongheadofthebicepshasbeenpreferably performedbyarthroscopy,andsafefixationmustensureearly return topostoperativemobilization withoutrelease ofthe tendon.2Amongthemostcommonlyusedfixationmethods (softtissuesuture,bonefixationwithboneanchors,andIS)
Bc
H
a
b
c
4
Bone anchors Interference screws
Resistance (N / mm)
Soft tissue 6
8 10 12 14
Fig.9–Centraldatavalues,dispersion,andpossible outliersofthelongheadofthebicepsstrengthafter tenodesisbyboneanchors,interferencescrew,andsoft tissuefixationwithoutimplant(n=30).
Bc
H
Fig.10–Specimenphotographshowingsutureslipinthe tendonduetotearinthetestwithboneanchors(arrow). Bc,biceps;H,humerus;Arrow,tendontear.
Table1–Load-to-failureofthetendonofthelonghead ofthebicepsaftertenodesiswithboneanchors, interferencescrew,andsoftpartssuturewithout implant(n=30).
Bone anchors
N
IS N
Softtissue N
Mean 95 152.7 104.7
Maximum 15 212 145
Minimum 50 57 75.9
SD 35.3 52.7 23.5
SD,standarddeviation;n,numberoftests;N,Newton;IS, interfer-encescrew.
Bc
H
Fig.11–Specimenphotographshowingtheslipofthe
tendonfixatedwithinterferencescrew(arrow).Bc,biceps;
H,humerus;Arrow,tendonslip.
Table2–Resistanceofthetendonofthelongheadofthe bicepsaftertenodesiswithboneanchors,interference screw,andsoftpartssuturewithoutimplant(n=30).
Bone anchors
N/mm
IS N/mm
Softtissue N/mm
Mean 4.7 9.9 4.1
Maximum 7.7 13.9 5.6
Minimum 2.8 6.4 3.2
SD 1.5 2.3 0.6
SD,standarddeviation;n,numberoftests;N,Newton/mm;IS, inter-ferencescrew.
moreresistant.14 Anchorsprepared withdouble wire have alsoshowedgreaterresistance.21Anotherfactoristhe differ-enceobservedbetweencyclical orcontinuous tensiletests. Thepresentstudyfollowedasimilarmodeltothatdescribed byBradburyetal.,18whotestedbicepsresistancewith con-tinuous traction and justified that fixation failures would occurpostoperativelyinasingle,suddenflexionorsupination movementoftheforearm,unliketheplasticdeformation sim-ulatedbycyclictesting.Nonetheless,thoseauthorssuggested thatcyclictestsshouldbeusedforcomparingtechniques,due tothepossibilityofvariation.Thiscanbeconsideredoneof thelimitationsofthepresentstudy.Althoughsomeauthors includedothertechniquesintheirstudies,somecomparisons betweenIS and boneanchors were retrieved in the litera-ture.Mostshowedastatisticallysignificant difference.This suggeststhatfixationwithISprovidesgreaterresistance com-paredwithboneanchors.10,12,15,16,22 Otherstudies observed no statistical differencebetween these techniques, despite the fact that the LTF was always higher for fixation with
IS.11,14,19–21,23Regardingsofttissuefixation,two
biomechani-calstudiesthatcomparedboneanchorswithISwereretrieved inthe literature,and no statistical differencein resistance was observedin both studies.Nevertheless, in the second study,thesofttissuesuturewasmadeinthetendonofthe pectoralismajormusclewithmorethantwostitches,which mayexplainthehigherLTFwhencomparedwithIS.17,24The presentstudydemonstratedthatISfixationismoreresistant and presents higherLTF than the other twomethods. The mainmechanismoffailureintheISmethodinthepresent studywastendonslipwithoutscrewloosening,observedin 80%ofthetests.Inonlytwosituationswasthesystem resis-tancehigher,withfailureatthemyotendinousjunction.This situationissimilartotheliterature,whichindicatesthat fail-uresintheimplant-bonesystemarerare.26Inthemethods withboneanchorsandsofttissue,failureoccurredmainlyin thetendon-suturejunction,withoutwireruptureorimplant release.Failuresoccurredinthelongitudinaldirectionofthe tendonfibersandofthetensileforces,whichproducedtear. Lopez-Vidrieroetal.17observedthesameeffectandconcluded thatthequalityofthetendonisimportantforthesetwotypes offixation.Anotherpossiblefailureisduetoawirerupture atthejunctionwiththeanchor;otherauthorsindicatedthat theserepresentthe majorityofcases.Inthese,failuremay occurduetolowerresistanceandqualityofthesutureordue tothequalityoftheanchor,asirregularitiesinthewire pas-sageholewouldcausegreaterfrictionandwouldmakethe wirefragile.10,12,27,28Forpracticalcomparisonsregardingthe safetyoftenodesis,theobservationsbyJazrawietal.shouldbe added29:thoseauthorsdefined52Nasthemeanforceexerted onthebicepstendontokeepthearminflexionwithout resis-tance,and110Nastheforcetosustain1kg.Whenperforming tenotomywithoutfixation,thepossibilityofretractionofthe tendonishigh,asdemonstratedbyWolfetal.aftermean trac-tionofonly110Ncausedmigration.13Evenwiththearticular portionofthethickenedtendon(thecommondegenerative process), failure occurs on average after traction of33N.30 Attemptstoincreaseresistancewithpreservationofthe supe-riorportionofthelabrumatthebicepsduringtenotomywere notshowntobesafe,withmediumstrengthofonly73N.18
Therefore, tenodesis should beperformedwhen the objec-tive istoprevent retractionofthe tendon. With this data, evenwiththelowerresistancevaluesobservedinthepresent study whencomparedwiththeliterature,theauthors sug-gestthatallthreetechniqueswouldbesafeforearlyactive postoperativemobilizationofthe upperlimb,providedthat this mobilization is made no weight or resistance. Never-theless,significantfluctuationswereobserved;inonestudy with bone anchors, fixation failed at50Ntraction, and in one study withIS, failed at 57N. Fixationwith IS, despite demonstratinggreater meanresistance,presentedahigher standard deviation with greater variation of high and low values.Perhapsthistechniqueismoresusceptibletoerrors undergreater influenceoffactors suchasvariationsinthe ratioofscrewdiameter/tendonand/orbonehole,aswellas boneand/ortendonquality.Otherfactorstobeconsideredare variationsthatcanoccurinsurgicalprocedures,including sur-gicaltechniqueandsurgeon’sexperience.Thiscouldjustify the oscillations; however, inthe present study’s methodol-ogy,thesevariableswerecarefullykeptequal.Brandetal.31 demonstratedthatbonedensitymayinterferewiththe resis-tance ofISfixation.Thisfactor shouldbetaken intoif the fixationismadeatthesupraorsub-pectorallevel,especially if performed inpatients withosteoporosis. Moreover, vari-ablediametersofthetendon,ofthescrew,andofthebone drilling, as well as the nature ofthe implant (metallic or bioabsorbable),donotappeartointerferewiththeultimate resistance.32,33 Thetechniqueswithbone anchorsand soft tissues, albeitofferingless resistance,weremoreconstant. Otherstudiesareneededtoexplainthisfinding.Some consid-erationscanbemadeabouttheuseofthethreetechniques: inelderlypatientsorpatientswithosteoporosis,fixationof LHBBTinthesofttissuesmay bemoreresistantthanbone anchors andIS, whichdependon good bonequality. Simi-larly,softtissuesutureshouldperhapsbeavoidedinsituations inwhichtendonsareaffectedbydegeneration,thus present-ingpoorquality.Youngpatientswithgoodbonequalityand higher functional demands would be favorable candidates forthe use ofimplants.Thisprofileincludespatients who need greater security in the fixation, cases in which IS is preferredtoboneanchors.Ifthecostfactorisrelevant,soft tissue fixationcould bejustified iftendon quality is favor-able.
Conclusion
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
ToProfessorMauroAlbanoandEdmarStievenFilhoforthe guidanceprovidedduringthisstudy.ToProfessorDr.Paulo Borges and to the mechanical engineering undergraduate RobertoLuisdeAssumpc¸ãofortechnicalsupportinthetests performedinthelaboratoryoftheUniversidadeTecnológica FederaldoParaná.
r
e
f
e
r
e
n
c
e
s
1. ChecchiaSL,DoneuxPS,MiyazakiAN,SilvaLA,FregonezeM, OssadaA,etal.Bicepstenodesisassociatedwitharthroscopic repairofrotatorcufftears.JShoulderElbowSurg.
2005;14(2):138–44.
2. ChecchiaSL,SantosPD,MiyazakiAN,FregonezeM,SilvaLA, LeiteFSF,etal.Avaliac¸ãodosresultadosdatenodese artroscópicadobíceps,utilizando-separafusode interferênciabioabsorvível.RevBrasOrtop.2007;42(8): 237–43.
3. GurnaniN,vanDeurzenDF,JanmaatVT,vandenBekerom MP.Tenotomyortenodesisforpathologyofthelongheadof thebicepsbrachii:asystematicreviewandmeta-analysis. KneeSurgSportsTraumatolArthrosc.2016;24(12):3765–71.
4. BoileauP,KrishnanSG,CosteJS,WalchG.Arthroscopicbiceps tenodesis:anewtechniqueusingbioabsorbableinterference screwfixation.Arthroscopy.2002;18(9):1002–12.
5. GartsmanGM,HammermanSM.Arthroscopicbiceps tenodesis:operativetechnique.Arthroscopy.2000;16(5): 550–2.
6. SekiyaJK,ElkousyHA,RodoskyMW.Arthroscopicbiceps tenodesisusingthepercutaneousintra-articulartranstendon technique.Arthroscopy.2003;19(10):1137–41.
7. GuminaS,CarboneS,PerugiaD,PerugiaL,PostacchiniF. Ruptureofthelongheadbicepstendontreatedwith tenodesistothecoracoidprocess.Resultsatmorethan30 years.IntOrthop.2011;35(5):713–6.
8. LoIK,BurkhartSS.Arthroscopicbicepstenodesisusinga bioabsorbableinterferencescrew.Arthroscopy.
2004;20(1):85–95.
9. JayamoorthyT,FieldJR,CostiJJ,MartinDK,StanleyRM,Hearn TC.Bicepstenodesis:abiomechanicalstudyoffixation methods.JShoulderElbowSurg.2004;13(2):160–4.
10.OzalayM,AkpinarS,KaraeminogullariO,BalcikC,TasciA, TandoganRN,etal.Mechanicalstrengthoffourdifferent bicepstenodesistechniques.Arthroscopy.2005;21(8):992–8.
11.MazzoccaAD,BicosJ,SantangeloS,RomeoAA,ArcieroRA. Thebiomechanicalevaluationoffourfixationtechniquesfor proximalbicepstenodesis.Arthroscopy.2005;21(11):1296–306.
12.RichardsDP,BurkhartSS.Abiomechanicalanalysisoftwo bicepstenodesisfixationtechniques.Arthroscopy. 2005;21(7):861–6.
13.WolfRS,ZhengN,WeichelD.Longheadbicepstenotomy versustenodesis:acadavericbiomechanicalanalysis. Arthroscopy.2005;21(2):182–5.
14.KilicogluO,KoyuncuO,DemirhanM,EsenyelCZ,AtalarAC, OzsoyS,etal.Time-dependentchangesinfailureloadsof3 bicepstenodesistechniques:invivostudyinasheepmodel. AmJSportsMed.2005;33(10):1536–44.
15.KusmaM,DienstM,EckertJ,SteimerO,KohnD.Tenodesisof thelongheadofbicepsbrachii:cyclictestingoffivemethods offixationinaporcinemodel.JShoulderElbowSurg. 2008;17(6):967–73.
16.GolishSR,CaldwellPE3rd,MillerMD,SinganamalaN, RanawatAS,TremeG,etal.Interferencescrewversussuture anchorfixationforsubpectoraltenodesisoftheproximal bicepstendon:acadavericstudy.Arthroscopy.
2008;24(10):1103–8.
17.Lopez-VidrieroE,CosticRS,FuFH,RodoskyMW.
Biomechanicalevaluationof2arthroscopicbicepstenodeses: double-anchorversuspercutaneousintra-articular
transtendon(PITT)techniques.AmJSportsMed. 2010;38(1):146–52.
18.BradburyT,DunnWR,KuhnJE.PreventingthePopeye deformityafterreleaseofthelongheadofthebicepstendon: analternativetechniqueandbiomechanicalevaluation. Arthroscopy.2008;24(10):1099–102.
19.PatzerT,SantoG,OlenderGD,WellmannM,HurschlerC, SchoferMD.Suprapectoralorsubpectoralpositionforbiceps tenodesis:biomechanicalcomparisonoffourdifferent techniquesinbothpositions.JShoulderElbowSurg. 2012;21(1):116–25.
20.TashjianRZ,HenningerHB.Biomechanicalevaluationof subpectoralbicepstenodesis:dualsutureanchorversus interferencescrewfixation.JShoulderElbowSurg. 2013;22(10):1408–12.
21.BaleaniM,FrancesconiD,ZaniL,GianniniS,SnyderSJ. Suprapectoralbicepsabiomechanicalcomparisonofanew softanchortenodesistechniqueversusinterferencescrew bicepstendonfixation.ClinBiomech(Bristol,Avon). 2015;30(2):188–94.
22.PatzerT,RundicJM,BobrowitschE,OlenderGD,HurschlerC, SchoferMD.Biomechanicalcomparisonofarthroscopically performabletechniquesforsuprapectoralbicepstenodesis. Arthroscopy.2011;27(8):1036–47.
23.PappDF,SkelleyNW,SutterEG,JiJH,WierksCH,BelkoffSM, etal.Biomechanicalevaluationofopensutureanchor fixationversusinterferencescrewforbicepstenodesis. Orthopedics.2011;34(7):e275–8.
24.AhmedM,YoungBT,BledsoeG,CutukA,KaarSG.
Biomechanicalcomparisonoflongheadofbicepstenodesis withinterferencescrewandbicepsslingsofttissue techniques.Arthroscopy.2013;29(7):1157–63.
25.LafosseL,VanRaebroeckxA,BrzoskaR.Anewtechniqueto improvetissuegrip:thelasso-loopstitch.Arthroscopy. 2006;22(11):1246.e1–3.
26.KochBS,BurksRT.Failureofbicepstenodesiswith interferencescrewfixation.Arthroscopy.2012;28(5): 735–40.
27.MeyerDC,NyffelerRW,FucenteseSF,GerberC.Failureof suturematerialatsutureanchoreyelets.Arthroscopy. 2002;18(9):1013–9.
28.DeakinM,StubbsD,BruceW,GoldbergJ,GilliesRM,Walsh WR.Suturestrengthandangleofloadapplicationinasuture anchoreyelet.Arthroscopy.2005;21(12):1447–51.
29.JazrawiLM,RokitoAS,BirdzellMG,ZuckermanJD.
Biomechanicsoftheelbow.In:NordinM,FrankelVH,editors. Basicbiomechanicsofthemusculoskeletalsystem.
Philadelphia:LippincottWilliams&Wilkins;2001. p.340–57.
30.AhmadCS,DiSipioC,LesterJ,GardnerTR,LevineWN, BiglianiLU.Factorsaffectingdroppedbicepsdeformityafter tenotomyofthelongheadofthebicepstendon.Arthroscopy. 2007;23(5):537–41.
mineraldensityandinsertiontorque.AmJSportsMed. 2000;28(5):705–10.
32.SlabaughMA,FrankRM,VanThielGS,BellRM,WangVM, TrenhaileS,etal.Bicepstenodesiswithinterferencescrew fixation:abiomechanicalcomparisonofscrewlengthand diameter.Arthroscopy.2011;27(2):161–6.
33.CabornDN,CoenM,NeefR,HamiltonD,NylandJ,Johnson DL.Quadrupledsemitendinosus-gracilisautograftfixationin thefemoraltunnel:acomparisonbetweenametalanda bioabsorbableinterferencescrew.Arthroscopy.