REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
SCIENTIFIC
ARTICLE
Comparison
of
bolus
and
continuous
infusion
of
esmolol
on
hemodynamic
response
to
laryngoscopy,
endotracheal
intubation
and
sternotomy
in
coronary
artery
bypass
graft
Esra
Mercanooglu
Efe
∗,
Basak
Atabey
Bilgin,
Zekeriyya
Alanoglu,
Murat
Akbaba,
Cigdem
Denker
DepartmentofAnesthesiologyandReanimation,AnkaraUniversityMedicalFaculty,Ankara,Turkey
Received16April2013;accepted15July2013 Availableonline25October2013
KEYWORDS Esmolol; Laryngoscopy; Endotracheal intubation; Sternotomy hemodynamics;
Coronaryartery;
Bypassgraftsurgery
Abstract
Backgroundandobjective: Theaimofthisrandomized,prospectiveanddoubleblindedstudy istoinvestigateeffectsofdifferentesmololuseonhemodynamicresponseoflaryngoscopy, endotrachealintubationandsternotomyincoronaryarterybypassgraftsurgery.
Methods:Afterapprovaloflocalethicscommitteeandpatients’writteninformedconsent,45 patientswererandomizedintothreegroupsequally.InInfusionGroup;from10minbefore intu-bationupto5thminuteaftersternotomy,0.5mg/kg/minesmololinfusion,inBolusGroup;2min beforeintubationandsternotomy1.5mg/kgesmololIVbolusandinControlGroup;%0.9NaCl wasadministered.Alldemographicparameterswererecorded.Heartrateandbloodpressure wererecordedbeforeinfusionuptoanesthesiainductionineveryminute,duringendotracheal intubation,everyminutefor10minutesafterendotrachealintubationandbefore,duringand aftersternotomyatfirstandfifthminutes.
Results:Whileareaundercurve(AUC)(SAP×time)wasbeingfoundmoreinGroupBandC thanGroupI,AUC(SAP×Tint andTst)andAUC(SAP×T2)wasfoundmoreinGroupBandC
thanGroupI(p<0.05).MoreoverAUC(HR×Tst)wasfoundlessinGroupBthanGroupCbutno
significantdifferencewasfoundbetweenGroupBandGroupI.
Conclusion: Thisstudy highlightsthatesmololinfusionismoreeffective thanesmololbolus administration on controlling systolic arterial pressure during endotracheal intubation and sternotomyinCABGsurgery.
© 2013SociedadeBrasileirade Anestesiologia.Publishedby ElsevierEditoraLtda.Allrights reserved.
∗Correspondingauthor.
E-mail:[email protected](E.M.Efe).
PALAVRAS-CHAVE Esmolol;
Laringoscopia; Intubac¸ão endotraqueal;
Hemodinâmicaem
esternotomia;
Artériacoronária;
Cirurgiade
revascularizac¸ão
Comparac¸ãodeesmololemboluseinfusãocontínuanarespostahemodinâmicaà
laringoscopia,intubac¸ãoorotraquealeesternotomiaemcirurgiaderevascularizac¸ão coronária
Resumo
Justificativaeobjetivo:o objetivo deste estudo prospectivo, randômico e duplo-cego foi investigarosefeitosdousodiferentedeesmololnarespostahemodinâmicaàlaringoscopia, intubac¸ãoorotraquealeesternotomiaemcirurgiaderevascularizac¸ãocoronária.
Métodos: apósobteraaprovac¸ãodoComitêdeÉticalocal econsentimentoinformado assi-nadopelospacientes,45pacientesforamrandomicamentedivididosemtrêsgrupos.OGrupoI (infusão)recebeu0,5mg/kg/mindeesmololeminfusãoapartirde10minantesdaintubac¸ão até5minutosapósaesternotomia;oBrupoB(bolus)recebeu1,5mg/kgdeesmololembolus
IVapartirde2minantesdaintubac¸ãoeesternotomia;ogrupoC(controle)recebeuNaCla 0,9%.Todososparâmetrosdemográficosforamregistados.Osvalores defrequênciacardíaca epressãoarterialforamregistradosdesdeantesdainfusãoatéainduc¸ãodaanestesiaacada minuto,duranteaintubac¸ãoendotraqueal,acadaminuto durante10minapósaintubac¸ão endotraquealeantes,duranteeapósaesternotomianoprimeiroequintominutos.
Resultados: enquantoaáreasobacurva(ASC)(SAP×tempo)foimaiornosgruposBeCqueno GrupoI,aASC(SAP×TinteTst)eASC(SAP×T2)forammaioresnosgruposBeCquenoGrupo
I(p<0,05).Alémdisso,aASC(FC×Tst))foimenornoGrupoBquenoGrupoC,masnãohouve diferenc¸asignificanteentreosgruposBeI.
Conclusão:este estudo destaca que a administrac¸ão de esmolol em infusão é mais eficaz queemboluspara controlarapressãoarterialsistólicaduranteaintubac¸ãoendotraqueale esternotomiaemCRC.
©2013SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
Patients undergoing coronary artery bypass graft (CABG)
surgeryareat risk for perioperative myocardial ischemia.
Tachycardiaasapredictorforincreasedmyocardialoxygen
consumption which doubles the incidence of myocardial
ischemia. During the operative procedure for coronary
revascularization, some maneuvers, such as intubation,
sternotomyandmediastinalpreparation,maybeassociated
withtachycardiaandincreasesinbloodpressuredespitethe
adequatelevelofanesthesia.1
Some drugs (IV opioids, vasodilators, calcium channel and-blockers) areavailable for theclinicians tocontrol thehemodynamicresponsetolaryngoscopyandintubation.2
-adrenoceptorblockerswereshown todecreasethe inci-denceofpostoperativemyocardialischemia.3
Esmolol (metil-3[4-(2-hidroxy-3[izopropylamino]propxy) fenyl] is a specific cardioselective beta 1-blocker and it is hydrosoluble, without intrinsic sympathetic activity or membranestabilizingactivityattherapeuticdosages. Distri-butionandeliminationhalf-lifeis2and9min,respectively. Esmololishydrolyzedbythebloodesterasesandasuitable agentfortheperioperativeperiod.4
Esmololasabolusorinfusionwasshowntoprevent tachy-cardiaandhypertensionduringlaryngoscopyandintubation inameta-analysisandpreviousstudies.5---7
Sofar,esmololbolusandinfusionadministrationhasnot been previously compared in cardiac patients. The pur-poseofthisrandomized,prospective,doubleblindedstudy, wastoevaluatetheeffectof1.5mg/kgesmololbolusand 0.5mg/kg/minesmololinfusion onhemodynamicresponse
oflaryngoscopy,endotrachealintubationandsternotomyin coronaryarterybypassgraft(CABG)surgery.
Methods
Fortyfivepatients,agingbetween18and80years,ejection fraction >40%, in ASA II---IV status, scheduled for elec-tive CABG surgery, between February and April 2006, in Ankara University Medical Faculty were enrolled to the study after obtaining approval from the Local Research Ethics Committeeand written informed consent.Patients withasthma,first-degreeatrioventricularblock,heartrate <50beats/min, acute myocardial infarction, Mallampati scoremorethantwoandunder-blockertreatmentor con-traindicated for -blocker agent were excluded from the study.
ethomidate, 5g/kg fentanyl vs. 0.1mg/kg vecuronium patients were intubated by the same clinician who were blind tothe study drugs.Anesthesia was maintainedwith 3g/kgfentanyland0.01mg/kgmidazolamIVbolus injec-tionevery30min.Patientswereventilatedtonormocapnie with50% air-oxygen in approximately 0.5MAC isoflurane. 0.03mg/kg vecuronium IV was administered as needed. Patients were randomly assigned according to computer-generated random number sequence into one of three groups.InInfusionGroup(GroupI);0.5mg/kg/minesmolol infusionwasstarted10minbeforetheendotracheal intuba-tionup to5thminute after sternotomy,and 2min before both intubation and sternotomy %0.9 NaCl was admin-istered, in Bolus Group (Group B); 2min before both endotrachealintubationandsternotomy1.5mg/kgesmolol bolus IV and from 10min before endotracheal intubation upto5thminuteaftersternotomy%0.9NaClwas adminis-teredandinControlGroup(GroupC);%0.9NaClinfusionand boluswasadministeredinsteadofesmolol.Heartrate(HR) andsystolicarterialpressure(SAP),diastolicarterial pres-sure(DAP)andmeanarterialpressure(MAP)wererecorded beforeinfusion(baseline)uptoanesthesiainduction, dur-ingandsoonafteranesthesiainduction,duringendotracheal intubation„everyminutefor10minafterendotracheal intu-bationandbefore,duringandatfirstandfifthminutesafter sternotomy.Alldemographicparameterswererecorded.
SPSS10.0for Windows(SPSSInc,Chicago,IL,USA)was usedfor all data analyses.For ˛=0.05and ˇ=0.20, sam-plesizewascalculated15subjectsforeachgroups.ANOVA andChi-squaretestswereusedforanalysisofdemographic variables.Areaundercurve(AUC)(heartrate,systolic, dia-stolicandmeanarterialpressurextime)wascalculatedand comparedwith one-wayANOVA test between groups. A p
valueof<0.05wasconsideredstatisticallysignificant.
Results
Nosignificantdifferencewasfoundbetweengroups accord-ingtodemographicparameters(Table1).
AUC (heart rate, systolic, diastolic and mean arte-rial pressure×time) between groups were compared and accordingtoTable2,GroupIwassignificantlymoreeffective thanothertwogroupsincontrollingsystolicarterialpressure (SAP)butnosignificantdifferenceonotherparameterswas found.
AUC (heart rate, systolic, diastolic and mean arterial pressure×T1(timebetweenthebeginningofinfusion and thebeginningofanesthesiainduction)andT2(timebetween
the beginningof anesthesiainduction andthe 5thminute after sternotomy)) were compared. According to Table 3
infusion groupwassignificantly moreeffective thanother twogroupsincontrollingSAPafterinductionbutno signifi-cantdifferencewasobservedonotherparameters.
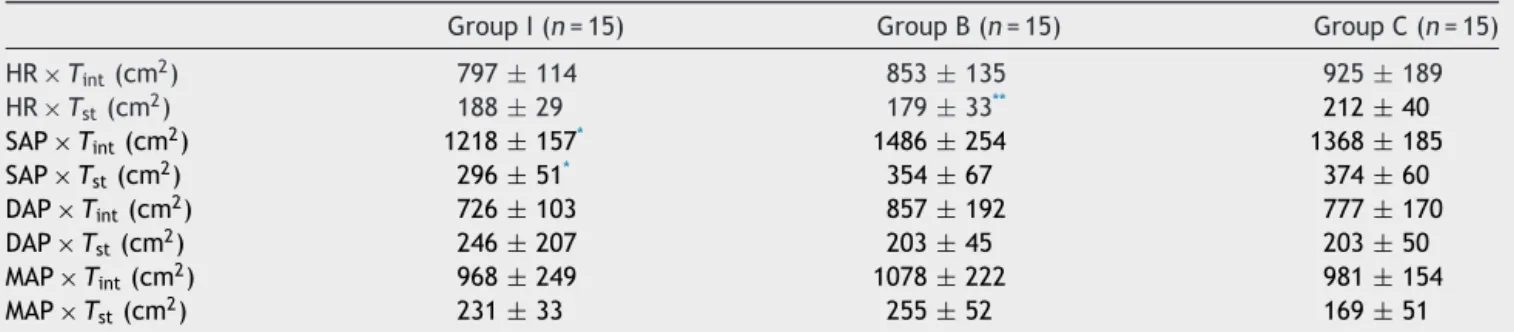
AUC (heart rate, systolic, diastolic and mean arterial pressure×Tint(timefromendotracheal intubationto ster-notomy)andTst (timefrombeginningofsternotomyto5th minaftersternotomy)werecompared.AccordingtoTable 4,infusiongroupwassignificantlymoreeffectivethanother twogroupsoncontrollingSAPduringsternotomyand intuba-tion.Moreoverbolusgroupwassignificantlymoreeffective thancontrolgroupincontrollingheartrate(HR)during
ster-notomybutnosignificantdifferencewasobservedbetween infusionandbolusgroup.
Noadverseorsideeffectswererecordedinbothgroups.
Discussion
This prospective, randomized, double blinded trial was designedtodeterminethehemodynamiceffectsofdifferent use of esmolol during laryngoscopy, intubation and ster-notomyinCABGsurgeriesandasaresultofthisstudy we foundoutthatwhileesmololinfusionwassignificantlymore effectivethanesmololbolusoncontrollingSAPduringboth intubationandsternotomy,esmolol bolus wassignificantly more effective on controlling HR only during sternotomy when compared to control group but no significant dif-ference was found when compared to infusion group. No significantsideeffectswereobserved.
Cardiovascularchangessuchashypertensionand tachy-cardiaduringtrachealintubationarepotentially detrimen-taltopatients withischemicheart disease.Esmololisthe
-selectiveadrenergic blockeravailableandwithitsrapid onsetandextremelyshortdurationofaction,wouldappear tobeanidealdrugforpreventingacuteincreasesinHRand SAP.8
However, we would advise caution when using bolus andinfusion doses ofesmolol but nopatient in ourstudy requiredtreatmentforhypotension,bradycardia,or signifi-cantarrhythmias.Nosideeffectswereobservedinanygroup ofpatients.
Sinceesmolol has been used clinically, itsinfusion use beforeCABGsurgeryorotherproceduresforpreventing car-diacischemiawasstudied andshown tobe effective.9 As
clinical use of esmolol became more common, due to its shortacting,simpleandeffectivebolususeofesmololhad increased.10---14
According to our knowledge, the bolus and infusion administrationofesmololhasnotbeencomparedbeforein apreviousstudy,sowedecidedtodesignthisstudy.
Asanoptimalintravenous(IV)esmololdoseforuse dur-inganesthesiainduction(laryngoscopyandintubation)and emergence(extubation)hasbeenpreviouslydeterminedto be1.5mg/kg,weusedthesamebolusdoseinourstudy.15---16
Aswecouldnotfindanoptimalinfusiondoseofesmololwe usedan average infusion dose that was0.5mg/kg/min in ourstudy.17WhileParnassetal.13werefoundnodifference
between 100 and 200mg esmolol on controlling hemody-namicresponseduring intubation,Yuan etal.12 found out
that200mgesmololpresentedabetterhemodynamic sta-bilitythan100mgesmololduringinductionofanesthesiain theirstudy.Moreover,inanothermulticenterstudy,whileIV bolusadministrationof100mgesmololwasbeingshownto beeffectiveincontrollinghemodynamicresponseof endo-trachealintubation,200mgdosagewasshowntocausemore hypotensionwithoutdesiredeffect.18
Table1 Demographicdataofgroups.
GroupI(n=15) GroupB(n=15) GroupC(n=15) p
Age(years) 61±6 63±7 64±7 NS
Gender(M/F) 10/5 11/4 10/5 NS
Weight(kg) 84±12 87±10 81±15 NS
Height(cm) 171±6 175±8 172±9 NS
ASAClassification(I/II/III/IV) 0/1/14/0 0/2/13/0 0/3/12/0 NS
ChronicDisease(±) 15/0 15/0 15/0 NS
Medication(±) 15/0 15/0 15/0 NS
Dataispresentedasmean±SD.
GroupI:EsmololinfusiongroupGroupB:EsmololbolusgroupGroupC:Controlgroup;NS:Statisticallynotsignificant.
Table2 Areaundercurve(AUC)ofgroups.(HR,SAP,DAPandMAP×T).
GroupI(n=15) GroupB(n=15) GroupC(n=15)
HRXTIME(cm2) 1729±208 1893±304 1973±304
SAPXTIME(cm2) 2843±360* 3297±548 3151±397
DAPXTIME(cm2) 1635±364 1767±348 1650±304
MAPXTIME(cm2) 2189±366 2404±399 2225±293
Dataispresentedasmean±SD.
HR,heartrate;SAP,systolicarterialpressure;DAP,diastolicarterialpressure;MAP,meanarterialpressure;T,time;GroupI,Esmolol infusiongroup;GroupB,EsmololbolusgroupGroupC,controlgroup.
* p<0.05comparedwithGroupBandC.
Table3 Areaundercurve(AUC)ofgroups.(HR,SAP,DAPandMAP×T1andT2).
GroupI(n=15) GroupB(n=15) GroupC(n=15)
HRxT1(cm2) 743±91 861±167 835±153
HRxT2(cm2) 986±136 1032±150 1136±224
SAPxT1(cm2) 1329±215 1456±298 1408±252
SAPxT2(cm2) 1514±193* 1840±299 1743±224
DAPxT1(cm2) 661±143 706±161 669±113
DAPxT2(cm2) 973±275 1061±223 981±211
MAPxT1(cm2) 989±161 1070±199 973±146
MAPxT2(cm2) 1200±265 1334±259 1251±191
Dataispresentedasmean±SD.
HR,heartrate;SAP,systolicarterial pressure;DAP, diastolicarterial pressure;MAP, meanarterial pressure;T1, timebetween the beginningofinfusionandthebeginningofanesthesiainduction;T2,timebetweenthebeginningofanesthesiainductionandthe5th minuteaftersternotomy;GroupI,Esmololinfusiongroup;GroupB,Esmololbolusgroup;GroupC,Controlgroup.
* p<0.05comparedwithGroupBandC.
Table4 AUC(HR,SAP,DAPandMAP×TintandTst)ofgroups.
GroupI(n=15) GroupB(n=15) GroupC(n=15)
HR×Tint(cm2) 797
±114 853±135 925±189
HR×Tst(cm2) 188±29 179±33** 212±40
SAP×Tint(cm2) 1218±157* 1486±254 1368±185
SAP×Tst(cm2) 296±51* 354±67 374±60
DAP×Tint(cm2) 726±103 857±192 777±170
DAP×Tst(cm2) 246±207 203±45 203±50
MAP×Tint(cm2) 968±249 1078±222 981±154
MAP×Tst(cm2) 231±33 255±52 169±51
Dataispresentedasmean±SD.
HR,heartrate;SAP,systolicarterialpressure;DAP,diastolicarterialpressure;MAP,meanarterialpressure;T˙Int,timefromendotracheal intubationtosternotomy;Tst,timefrombeginningofsternotomyto5thminuteaftersternotomy;GroupI,Esmololinfusiongroup;Group B,Esmololbolusgroup;GroupC,controlgroup.
blind to thestudy drug,to standardize the noxious stim-uliduringlaryngoscopyandintubation.Moreoverpatients’ medications and Mallampati scores were similarbetween groups.
Insomepreviousstudiespatientswereincludedintothe study according to their medications with or without  -blocker agents.17,19 The results of these studies revealed
thatpatientswhoenrolledtothethesestudiesshouldhave been chosenupon their treatmentof -blockeragents. In ourstudythepatientson-blockeragentswerenotincluded assimilartoKorenagaetal’sstudy.Theyexcludedpatients on-blockertherapyfromtheirstudyandreportedaslight butstatisticallyinsignificantdecreaseinheartratefrom83 to 70beat/min during infusion of esmolol 500g/kg/min prior to anesthetic induction.17 The same dose was used
in our study and we also did not observe any significant decreaseinHR.
Butunlikeourstudy,Brujinetal19investigatedthe
hemo-dynamiceffectsofesmololinchronically-blockedpatients undergoing coronary artery bypass surgery and they con-cludedthatinpatientswhomchronic-blockertherapywas continueduntilthetimeofsurgery,esmololdidnotfurther attenuatedtheheartrateresponsebutdidattenuatedthe increaseinbloodpressure.
Therearedifferentdosesofesmololstudiedinprevious studies andthe choice ofoptimal dose of esmolol is very importanttobalancebetweenthedesiredandsideeffects. Although we preferred 1.5mg/kg bolus dose of esmolol andmany studiesshowedtheeffectiveness oflarge doses of esmolol, Bensky et al.20 compared 0.2 and 0.4mg/kg
esmolol and found out that both doses weremore effec-tiveindecreasingtheheartratethancontrolgroupandthe 0.4mg/kg dose significantly blunted theincrease in mean arterialpressureseenincontrolgroup.
However, in another study,21 the result of a
combina-tionofnicardipine(30g/kg)andesmolol(1mg/kg)showed nosignificantchangeinhemodynamicresponsetotracheal intubationwhencomparedtosaline.
Therearealsodifferenttechniquestofindoutthebest one in previous studies. Some clinicians investigated the effect of esmolol bolus followed by esmolol infusion on hemodynamic effectstofindout themost properdose of esmolol.11,22---26 In astudymade bySchäffer etal.,double
bolus ofesmolol wasusedinsteadof onebolus tocontrol thehemodynamic effectandtheyreacheda betterresult withdoublebolusof100mgesmolol.27 Inanotherprevious
studies,28---37esmololwascomparedwithotheragentsalone
orascombination.
Thesetechniques anddifferentdosesofesmololshould bestudiedtousealoneorincombinationtofindoutthemost appropriateone.However,itshouldbekeptinmindthatthe patientcharacteristicsanddifferentproceduresmayaffect theeffectsofEsmololandotherdrugs.
Therearesomelimitationsofthiscurrentstudy.Wedid notcalculate PCWPandcardiac indexinour study.Those parameters would be a better guide for cardiac perfor-mance.Wedidnotmeasurecatecholaminelevelsofpatients whichwouldtakeustomorereliableresultsaboutthe hemo-dynamicandstress response.Moreoverthe samplesizeof the study disabled us to demonstrate other factors that mightenrolltothechangesfor hemodynamicparameters. Asbolusdosewasnotaseffectiveasonbloodpressure,it
mighthavebeenbettertoaddanotherbolusdosegroupor makedoublebolusestoinvestigatetheeffectivenessasthe previousstudies.
Inconclusion,accordingtoourstudythattheeffectof esmololbolusandinfusionadministrationonhemodynamic responsetolaryngoscopy,endotrachealintubationand ster-notomyinCABGsurgerywascompared,both groupswere foundsafeandesmolol infusionwasfound moreeffective thanesmololbolusoncontrollingSAPduringbothintubation andsternotomy.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.KlingD,BoldtJ,ZickmannB,etal.Thehemodynamiceffects of a treatment withbeta-receptor blockers duringcoronary surgery.Acomparisonbetweenacebutololandesmolol. Anaes-thesist.1990;39:264---8.
2.Kovac AL. Controlling the hemodynamic response of laryn-goscopy and tracheal intubation. J Clin Anesth. 1996;8: 63---79.
3.Wallace A, Layug B, Tateo I, et al. Prophylactic atenolol reduces postoperative myocardial ischemia. Anesthesiology. 1998;88:7---17.
4.DengCY,LinSG,ZhangWC,etal.EsmololinhibitsNa+current
inratventricularmyocytes.MethodsFindExpClinPharmacol. 2006;28:697---702.
5.FigueredoE,Garcia-Fuentes:EM.Assessmentoftheefficacyof esmololonthehaemodynamicchangesinducedbylaryngoscopy and tracheal intubation: a meta-analysis. Acta Anaesthesiol Scand.2001;45:1011---22.
6.MionG,RuttimannM,DescraquesC,etal.Bolusesmololprior totrachealintubationoftheelderlypatient.CahAnesthesiol. 1992;40:95---9.
7.ZalunardoMP,ZollingerA,SzelloeP,etal.Cardiovascularstress protectionfollowinganesthesiainduction.Comparisonof cloni-dineandesmolol.Anaesthesist.2001;50:21---5.
8.GorczynskiRJ,ShafferJE,LeeRJ.PharmacologyofASL-8052, a novel beta-adrenergic receptor antagonist with an ultra-short duration of action.J Cardiovasc Pharmacol. 1983;56, 77.
9.Newsome LR, Roth JV, Hug Jr CC, et al. Esmolol atten-uates hemodynamic responses during fentanyl-pancuronium anesthesia for aortocoronary bypass surgery. Anesth Analg. 1986;65:451---6.
10.Kanitz DD, Ebert TJ, Kampine JP. Intraoperative use of bolus doses of esmolol to treat tachycardia. J Clin Anesth. 1990;2:238---42.
11.RevesJG,CroughwellND,HawkinsE,etal.Esmololfor treat-ment of intraoperative tachycardia and/or hypertension in patientshavingcardiacoperations.Bolusloadingtechnique.J ThoracCardiovascSurg.1990;100:221---7.
12.YuanL,ChiaYY,JanKT,etal.Theeffectofsinglebolusdoseof esmololforcontrollingthetachycardiaandhypertension dur-inglaryngoscopyandtrachealintubation.ActaAnaesthesiolSin. 1994;32:147---52.
14.Sharma S, GhaniAA, WinN, etal. Comparison oftwobolus dosesofesmololforattenuationofhaemodynamicresponseto trachealintubation.MedJMalaysia.1995;50:372---6.
15.Fuhrman TM, Ewell CL, Pippin WD, et al. Comparison of the efficacy of esmolol and alfentanil to attenuate the hemodynamicresponsestoemergenceandextubation.JClin Anesth.1992;4:444---7.
16.DysonA,IsaacPA,PennantJH,etal.Esmololattenuates car-diovascular responses to extubation. Anesth Analg. 1990;71: 675---8.
17.KorenagaGM,KirkpatrickA,LordJG,etal.Effectofesmololon tachycardiainducedbyendotrachealintubation.AnesthAnalg. 1985;64:238.
18.MillerDR,MartineauRJ,WynandsJE,etal.Bolusadministration ofesmololforcontrollingthehaemodynamicresponseto tra-chealintubation:thecanadianmulticentretrial.CanJAnaesth. 1991;38:849---58.
19.deBruijnNP,CroughwellN,RevesJG.Hemodynamiceffectsof esmololinchronically-blockedpatientsundergoing aortocoro-narybypasssurgery.AnesthAnal.1987;66:137---41.
20.Bensky KP, Donahue-Spencer L, Hertz GE, et al. The dose-related effects of bolus esmolol on heart rate and blood pressure following laryngoscopy and intubation. AANA J. 2000;68:437---42.
21.Tan PH, YangLC, Shih HC, et al. Combined use of esmolol and nicardipine to blunt the haemodynamic changes fol-lowing laryngoscopy and tracheal intubation. Anaesthesia. 2002;57:1207---12.
22.GoldMI,SacksDJ,GrosnoffDB, etal.Useofesmololduring anesthesiatotreattachycardiaandhypertension.AnesthAnalg. 1989;68:101---4.
23.LiuPL,GattS,GuginoLD,etal.Esmololforcontrolofincreases in heart rate and bloodpressure during tracheal intubation after thiopentone and succinylcholine. Can Anaesth Soc J. 1986;33:556---62.
24.BilottaF,Lam MA,DoronzioA, etal. Esmololblunts postop-erativehemodynamicchangesafterpropofol-remifentaniltotal intravenousfast-trackneuroanesthesiaforintracranialsurgery. JClinAnesth.2008;20:426---30.
25.ChiaYY,ChanMH,KoNH,etal.Roleofb-blockadein anaesthe-siaandpostoperativepainmanagementafterhysterectomy.Br JAnaesth.2004;93:799---805.
26.Cork RC, Kramer TH, Dreischmeier B, et al. The effect of esmolol given duringcardiopulmonary bypass.Anesth Analg. 1995;80:28---40.
27.SchäfferJ,KargC,PiepenbrockS:.Esmololasabolusfor pre-ventionofsympatheticadrenergicreactionsfollowinginduction ofanesthesia.Anaesthesist.1994;43:723---9.
28.EbertJP,PearsonJD,GelmanS,etal.Circulatoryresponsesto laryngoscopy:thecomparativeeffectsofplacebo,fentanyland esmolol.CanJAnaesth.1989;36Pt1:301---6.
29.Hussain AM, Sultan ST. Efficacy of fentanyl and esmolol in the prevention of haemodynamic response to laryngoscopy and endotracheal intubation. J Coll Physicians Surg Pak. 2005;15:454---7.
30.GongZ,LuoA. Effectsofalfentaniland esmololon hemody-namicandcatecholamineresponsetotrachealintubation.Chin MedSciJ.1999;14:189---92.
31.Fernandez-GalinskiS,BermejoS,MansillaR,etal.Comparative assessmentoftheeffects ofalfentanil, esmololor clonidine whenusedasadjuvantsduringinductionofgeneralanaesthesia. EurJAnaesthesiol.2004;21:476---82.
32.BansalS,PawarM.Haemodynamicresponsestolaryngoscopy andintubation inpatientswithpregnancy-induced hyperten-sion:effectofintravenousesmololwithorwithoutlidocaine. IntJObstetAnesth.2002;11:4---8.
33.Atlee JL, Saeed Dhamee M, Olund TL, et al. The use of esmolol,nicardipine, ortheir combinationto blunt hemody-namic changes after laryngoscopy and tracheal intubation. AnesthAnalg.2000;90:280---5.
34.ColomaM, ChiuJW, White PF, et al. The useof esmolol as analternativetoremifentanilduringdesfluraneanesthesiafor fast-trackoutpatientgynecologiclaparoscopicsurgery.Anesth Analg.2001;92:352---7.
35.FengCK,ChanKH,LiuKN,etal.Acomparisonoflidocaine, fen-tanyl,andesmololforattenuationofcardiovascularresponse tolaryngoscopyandtrachealintubation.ActaAnaesthesiolSin. 1996;34:61---7.
36.GuptaS, Tank P.Acomparative studyofefficacyof esmolol andfentanylforpressureattenuationduringlaryngoscopyand endotrachealintubation.SaudiJAnaesth.2011;5:2---8. 37.GaubatzCL,WehnerRJ.Evaluationofesmololandfentanylin