REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologiawww.sba.com.br
REVIEW
ARTICLE
Benefit
of
general
anesthesia
monitored
by
bispectral
index
compared
with
monitoring
guided
only
by
clinical
parameters.
Systematic
review
and
meta-analysis
Carlos
Rogério
Degrandi
Oliveira
a,b,∗,
Wanderley
Marques
Bernardo
c,d,e,
Victor
Moisés
Nunes
daHospitalGuilhermeAlvaro,DepartamentodeAnestesiologia,Santos,SP,Brazil
bHospitalAnaCosta,DepartamentodeAnestesiologia,Santos,SP,Brazil
cUniversidadedeSãoPaulo,FaculdadedeMedicina,MedicinaBaseadaemEvidência,SãoPaulo,SP,Brazil
dCentroUniversitárioLusíada,FaculdadedeMedicinadeSantos,Santos,SP,Brazil
eProgramaDiretrizesdaAssociac¸ãoMédicaBrasileira,Santos,SP,Brazil
Received14July2015;accepted22September2015 Availableonline14April2016
KEYWORDS Generalanesthesia; Anesthetics; Inhalation; Intravenous anesthesia; Bispectral index-monitoring
Abstract
Background: Thebispectralindexparameterisusedtoguidethetitrationofgeneralanesthesia; however,manystudieshaveshownconflictingresultsregardingthebenefitsofbispectralindex monitoring.Theobjectiveofthissystematicreviewwithmeta-analysisistoevaluatetheclinical impactofmonitoringwiththebispectralindexparameter.
Methods:The search for evidence in scientific information sources was conducted during December2013toJanuary 2015,thefollowing primarydatabases:Medline/PubMed,LILACS, Cochrane,CINAHL,Ovid,SCOPUSandTESES.Thecriteriaforinclusioninthestudywere random-izedcontrolledtrials,comparinggeneralanesthesiamonitored,withbispectralindexparameter withanesthesiaguidedsolelybyclinicalparameters,andpatientsagedover18years.The crite-riaforexclusionwerestudiesinvolvinganesthesiaorsedationfordiagnosticprocedures,and intraoperativewake-uptestforsurgeryofthespine.
Results:The use ofmonitoringwith thebispectralindex hasshown benefits reducing time to extubation,orientation in timeand place, anddischarge from boththe operating room andpostanestheticcareunit.Theriskofnauseaandvomitingaftersurgerywasreducedby 12% inpatients monitoredwith bispectralindex.Occurred areductionof3% inthe riskof cognitiveimpairmentpostoperativelyat3monthspostoperativelyand6%reductionintherisk ofpostoperativedeliriuminpatientsmonitoredwithbispectralindex.Furthermore,theriskof intraoperativememoryhasbeenreducedby1%.
∗Correspondingauthor.
E-mail:[email protected](C.R.Oliveira). http://dx.doi.org/10.1016/j.bjane.2015.09.001
Conclusion: Clinically,anesthesiamonitoringwith theBIScanbe justifiedbecauseitallows advantagesfromreducingtherecoverytimeafterwaking,mainlybyreducingtheadministration ofgeneralanestheticsaswellastheriskofadverseevents.
©2016SociedadeBrasileiradeAnestesiologia.Publishedby ElsevierEditoraLtda.Thisisan openaccessarticleundertheCCBY-NC-NDlicense( http://creativecommons.org/licenses/by-nc-nd/4.0/).
PALAVRAS-CHAVE Anestesiageral; Anestésicos; Inalac¸ão; Anestesia intravenosa; Monitorac¸ãodo índicebispectral
Benefíciodaanestesiageralcommonitorac¸ãodoíndicebispectralemcomparac¸ão comomonitoramentoguiadoapenasporparâmetrosclínicos.Revisãosistemáticae metanálise
Resumo
Justificativa: Oparâmetroíndicebispectral(BIS)éusadoparaguiaratitulac¸ãodaanestesia geral;noentanto,muitosestudostêmmostradoresultadosconflitantesquantoaosbenefícios damonitorac¸ãodoBIS. Oobjetivodestarevisão sistemáticacommeta-análisefoi avaliaro impactoclínicodamonitorac¸ãodoparâmetroBIS.
Métodos: Abuscaporevidênciasemfontesdeinformac¸ãocientíficasfoiconduzidadedezembro de2013ajaneirode2015nasseguintesbasesdedados:Medline/PubMed,LILACS,Cochrane, CINAHL,Ovid,SCOPUSeTESES.Oscritériosdeinclusãoforamestudosrandomizadose controla-dos,comparandoanestesiageralmonitoradacomoparâmetroBIScomanestesiaguiadaapenas porparâmetrosclínicosempacientescomidadesuperiora18anos.Oscritériosdeexclusão foramestudosqueenvolveramanestesiaousedac¸ãoparaprocedimentosdediagnósticoeteste dedespertarnointraoperatóriodecirurgiadacolunavertebral.
Resultados: Ousodemonitorac¸ãocomoBISmostroubenefícioscomoareduc¸ãodotempode extubac¸ão,orientac¸ãonotempoenoespac¸o,altadasaladecirurgiaedasaladerecuperac¸ão pós-anestesia.Oriscodenáuseasevômitosnopós-operatóriofoireduzidoem12%empacientes monitorados comoBIS.Ocorreuumareduc¸ãode3%noriscodedisfunc¸ãocognitivaemtrês mesesdopós-operatórioe6%noriscodedelíriopós-operatórioempacientesmonitoradoscom oBIS.Alémdisso,oriscodedespertarcommemóriaintraoperatóriafoireduzidoem1%. Conclusão:Clinicamente, amonitorizac¸ãocomoBISpodeserjustificada,poispermite van-tagens em reduzir o tempo de recuperac¸ão, principalmente reduzindo a administrac¸ão de anestésicosgeraiseoriscodeeventosadversos.
©2016SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Este ´eum artigo OpenAccess sobumalicenc¸aCCBY-NC-ND( http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Bispectral index (BIS) is a multiprocessor EEG parameter
specially developedtomeasure theeffects ofanesthetics
on the brain hypnotic state, making it possible to
mea-sure the depthof anesthesia. The introduction of the BIS
in clinical practice is a reliable method to assess brain
function and allows the titrationof hypnotics on cortical activity.
Duetoanesthesiamayoccurunpredictableresponsesat
different times of surgery with a great variability among
patients,sotheexactdosageof anesthetictobe adminis-teredstillremainsachallenge.However,manystudieshave
shown conflicting results regarding the advantages of BIS
andifthismonitoringimprovesrecoverytimesandhospital discharges,aswellasminimizesadverseevents.
The objective of this systematic review with
meta-analysis was to clinically evaluate the objective BIS
monitoring parameter, comparedwith the clinical
param-etersingeneralanesthesia.
Methods
The research for evidence in scientific sources of
infor-mation was performed by two independent reviewers
(CRDO, WMB) during the period from December 2013
to January 2015, the following primary databases:
Med-line/PubMed, LILACS, Cochrane, CINAHL, Ovid, SCOPUS
and THESES. The search strategy was made with the
following words: (Anesthesia, General OR Anesthetics,
InhalationORAnesthetics,Intravenous)AND(Consciousness MonitorsORMonitoring,IntraoperativeORBispectral
index-monitoring technology OR Bispectral index-monitoring OR
BispectralindexmonitoringORDrugMonitoringOR
Aware-ness OR Monitoring, Physiologic OR BIS monitoring) AND
Random*.
ThecriteriaforinclusioninthestudywereRandomized
ControlledTrials(RCTs)withlevelofevidence1B/2B(Oxford CentreforEvidence-basedMedicine)inEnglish,Spanishor
Portugueselanguages,comparingvenousorinhaledgeneral
Table1 Consideredoutcomes. Timeforspontaneouseyeopening
Timeforeyeopeninguponverbalcommand Timetotrachealextubation
Timefororientationintimeandplace Timeforleavingoperatingroom
Timefordischargefrompostanesthesiacareunit(PACU) Timeforhospitaldischarge
Postoperativenauseaandvomiting(PONV) Cognitivedisordersinthepostoperativeperiod (1weekafterextubation)
Cognitivedisordersinthepostoperativeperiod (3monthsafterextubation)
Postoperativedelirium Intraoperativememory
guidedsolelybyclinicalparameters;patientsagedover18 years.
Thecriteriaforexclusionwerestudiesinvolving anesthe-siaandsedationfordiagnosticprocedures.Studiesinvolving intraoperativewake-up testfor surgery ofthe spinewere excluded. Nor were objects of study the clinical trials of ketamineasvenousanesthetic.
Thissystematicreviewwithmeta-analysiswasrecorded inPROSPEROdatabaseunderthenumberCRD42015017240.
TheoutcomesconsideredaredescribedinTable1.
The results of the meta-analysiswere obtainedby the
RevMan5.2software(Review ManagerComputerprogram.
Version 5.2 Copenhagen: The Nordic Cochrane Centre,
CochraneCollaboration©2014).
Regarding meta-analysis, the difference was
calcu-lated in risk difference for dichotomic variables with
Mantel---Haenszel (M-H) test with95%ConfidenceInterval; andinmeandifferencewithfixedeffectusingInverse
Vari-ance (IV), witha 95% Confidence Interval,for continuous
variables.
An I2 of 0% indicates no heterogeneity among studies,
valuesbelow50%indicatealowheterogeneity,andabove
50%,highheterogeneity.
Whentheheterogeneitywasgreaterthan50%,a sensitiv-ityanalysiswasperformed,removingthestudiesthatwere out ofthe ‘‘forestplot’’. To achievereductionin
hetero-geneityremainedoutofthestudymeta-analysis.
Results
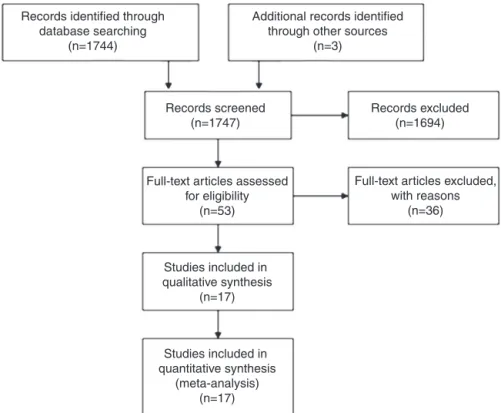
Initially,thesearchresultedin1.747scientificarticles.After applyingtheinclusionandexclusioncriteriawereselected 17RCT(Fig.1).
Table2showsthetrialsselectedwiththerespective
lev-elsofevidence,Jadadscale,numberofpatientsrandomized andanalyzed,patientnumbersintheinterventionand con-trolgroupsandPICOstrategy.Atotalof10,761patientswere
analyzed, 5668 in the intervention groupand 5093 in the
controlgroup.
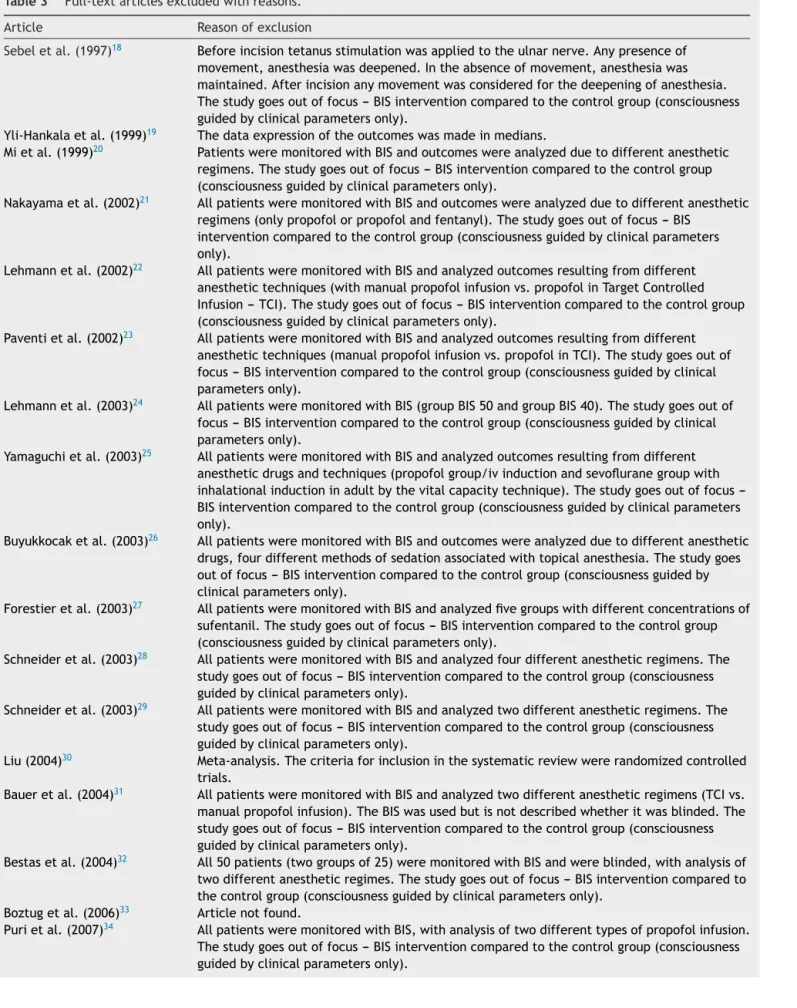
Table3showsthe36full-textarticlesexcludedwith
rea-sons.
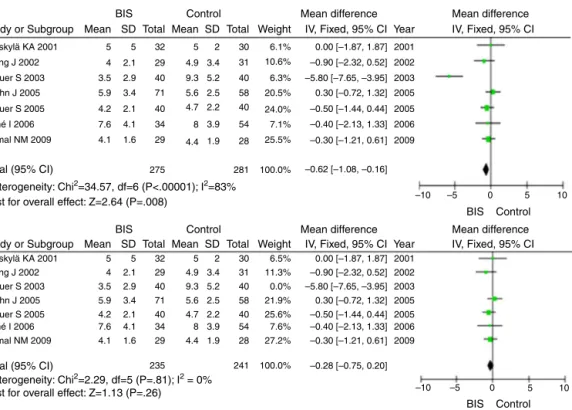
Thetimefor spontaneouseye openingis countedfrom
theendofthelastsuture,whentheninhaledorintravenous
anesthetic is discontinued. The monitoring with the BIS,
compared exclusively with clinical parameters, showed a
reduction in the time for spontaneous opening 0.62min
eye (95% CI−1.08, −0.16), withan I2=83%.In sensitivity
analysis, when removed the study Kreuer et al.7 was
removed we have an I2=0%, with reduction of time for
Records identified through database searching
(n=1744)
Additional records identified through other sources
(n=3)
Records excluded (n=1694) Records screened
(n=1747)
Full-text articles assessed for eligibility
(n=53)
Full-text articles excluded, with reasons
(n=36)
Studies included in qualitative synthesis
(n=17)
Studies included in quantitative synthesis
(meta-analysis) (n=17)
Table2 Selectedrandomizedclinicaltrials(RCT).
RCT EL J R/A I/C P I C O
Nelskyläetal. (2001)1
2B 0 62/62 32/30 ASAIorII,
between18and50 years,
gynecological surgery.
BISbetween50 and60years
‘‘Blinded’’ monitor. Anesthesiawas adjustedaccording toclinical parameters. Timefor spontaneouseye opening, extubation, orientationintime andplace,hospital dischargeand PONV. Wongetal.
(2002)2
1B 3 68/60 29/31 >60years,ASA
I---III,orthopedic surgery.
BISbetween50 and60. ‘‘Blinded’’ monitor. Anesthesiawas adjustedaccording toclinical parameters. Timefor spontaneouseye opening, orientationintime andplaceand PACUdischarge. Luginbühl
etal. (2003)3
2B 2 160/160 80/80 >18years,
gynecological surgery.
BISbetween45 and55.
Anesthesiawas adjustedaccording toclinical parameters.
Timetotracheal extubation.
Ahmadetal. (2003)4
1B 3 99/97 49/48 >18years,
gynecological surgery.
BISbetween50 and60.
Anesthesiawas adjustedaccording toclinical parameters.
Timeforhospital discharge.
Bas¸aretal. (2003)5
2B 0 60/60 30/30 >18years,ASAIor II,abdominal surgery.
BISbetween40 and60. ‘‘Blinded’’ monitor. Anesthesiawas adjustedaccording toclinical parameters.
Timeofeye openingupon verbalcommand.
Puriand Murthy (2003)6
2B 2 30/30 14/16 >18years,
myocardial revascularization orvalve replacementwith cardiopulmonary bypass,18---70 years.
BISbetween45 and55. ‘‘Blinded’’ monitor. Anesthesiawas adjustedaccording toclinical parameters.
Timeofeye openingupon verbalcommand andextubation, intraoperative memory.
Kreueretal. (2003)7
2B 2 120/120 40/40 >18years,ASA I-III,orthopedic surgery.
BIS50andinthe last15minof60.
Anesthesiawas adjustedaccording toclinical parameters. Timefor spontaneouseye openingand extubation. Mylesetal.
(2004)8
1B 5 2.503/2.463 1.225/1.238 >18yearswithat leastonehighrisk factorto intraoperative awakening.
BISbetween40 and60.
Monitorturnedoff. Anesthesiawas adjustedaccording toclinical parameters. Timefor spontaneouseye opening,timefor dischargefrom PACUand intraoperative memory. Bruhnetal.
(2005)9
2B 2 200/200 71/58 >18years,ASA I-III.
BISof50.Inthe last15minBISof 60. Anesthesiawas adjustedaccording toclinical parameters. Timefor spontaneouseye openingand extubation,PONV andintraoperative memory. Kreueretal.
(2005)10
1B 4 120/120 40/40 >18years,ASA I-III,orthopedic surgery.
BIS50andinthe last15minchange to60. Anesthesiawas adjustedaccording toclinical parameters. Timefor spontaneouseye opening, extubationand timeforleaving operationroom. Vretzakisetal.
(2005)11
1B 3 130/121 36/44 >18years,
myocardial revascularization orvalve replacementwith cardiopulmonary bypass,ejection fraction>45%.
BISunder60. Anesthesiawas adjustedaccording toclinical parameters.
Table2 (Continued)
RCT EL J R/A I/C P I C O
Aiméetal. (2006)12
2B 1 140/125 34/54 Agebetween18
and80years,ASA I-III,urologic, orthopedic, abdominaland gynecological surgery.
BISbetween40 and60.
‘‘Blinded’’ monitor. Anesthesiawas adjustedaccording toclinical parameters.
Timefor spontaneouseye openingand traqueal extubation.
Ibraheimetal. (2008)13
2B 0 30/30 15/15 >18years,morbid obese,gastric bandsurgery.
BISbetween40 and60.
Anesthesiawas adjustedaccording toclinical parameters
Timeofeye openingupon verbalcommand, timefor extubationand dischargefrom PACU. Kamaletal.
(2009)14
2B 1 60/57 29/28 >18years,ASA
I-III,abdominal surgery
BISbetween50 and60.
‘‘Blinded’’ monitor. Anesthesiawas adjustedaccording toclinical parameters.
Timefor spontaneouseye opening, extubation, orientationintime andplace,leaving operatingroom, dischargefrom PACUand intraoperative memory. Zhangetal.
(2011)15
1B 5 5.309/5.228 2.919/2.309 >18years,total intravenous anesthesia
BISbetween40 and60.
‘‘Blinded’’ monitor. Anesthesiawas adjustedaccording toclinical parameters.
Intraoperative memory.
Chanetal. (2013)16
1B 3 921/902 450/452 >60years,elective non-cardiac surgery.
BISbetween40 and60.
Anesthesiawas adjustedaccording toclinical parameters.
Timefor spontaneouseye opening,timefor dischargefrom PACU,cognitive dysfunctioninthe postoperative period(oneweek andthreemonths later)and delirium. Radtkeetal.
(2013)17
1B 3 1.277/1.155 575/580 >60years BISbetween40 and60.
‘‘Blinded’’ monitor. Anesthesiawas adjustedaccording toclinical parameters.
Cognitive dysfunctioninthe postoperative period(oneweek andthreemonths later)and delirium. ASA,AmericanSocietyofAnesthesiologistsPhysicalStatus;RCT,RandomizedClinicalTrial;EL,EvidenceLevel;J,Jadadscore;R/A, patientsrandomizedandanalyzed;I/C,interventiongroup/controlgroup;P,population;I,intervention;C,controlorcomparison;O, outcome.
spontaneouseyeopeningof0.28min(95%CI−0.75,0.20).
However, the statistically significant difference was lost (Fig.2).
The time for eye opening upon verbal command is
countedfromtheendof lastsuture,when theinhaled or
intravenous anesthetic is discontinued and the patient is
askedtoopenhiseyes.Therewasareductionintimetoeye openingatverbalcommandof0.63min(95%CI−1.30,0.05),
withan I2=67%,withnostatisticallysignificant difference
(Fig.3).
The use of BIS reduced 1.18min in the time of
tra-cheal extubation(95% CI −1.65, −0.70), withan I2=79%.
In sensitivity analysis, when the study Kreuer et al.7
was removed, the time to tracheal extubation reduced
0.87min (95% CI −1.36, −0.38), with an I2=59%,
main-taining, therefore, a statistically significant difference (Fig.4).
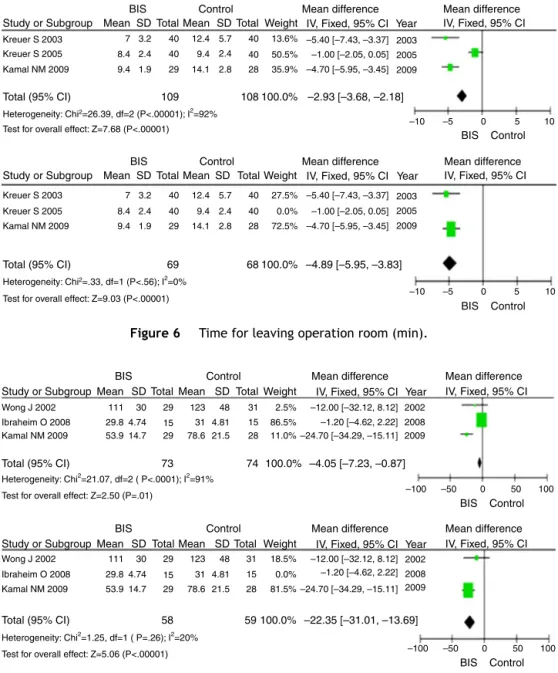
Thecombinationofthreestudies1,2,14demonstratedthat thetimefororientationintimeandplacereduced3.08min (95%CI−3.70,−2.45)withanI2=73%.Insensitivity
analy-sis,whenthestudyNelskyläetal.1wasremovedwehavea reductionof3.76min(95%CI−4.55,−2.97)withanI2=0%,
maintaining,therefore,astatisticallysignificantdifference (Fig.5).
WhenusingtheBIS,thetimeforthepatienttobeable
toget outofthe operatingroomandgotoPACUreduced
2.93min (95%CI−3.68,−2.18),withan I2=92%.In
Table3 Full-textarticlesexcludedwithreasons.
Article Reasonofexclusion
Sebeletal.(1997)18 Beforeincisiontetanusstimulationwasappliedtotheulnarnerve.Anypresenceof
movement,anesthesiawasdeepened.Intheabsenceofmovement,anesthesiawas maintained.Afterincisionanymovementwasconsideredforthedeepeningofanesthesia. Thestudygoesoutoffocus---BISinterventioncomparedtothecontrolgroup(consciousness guidedbyclinicalparametersonly).
Yli-Hankalaetal.(1999)19 Thedataexpressionoftheoutcomeswasmadeinmedians.
Mietal.(1999)20 PatientsweremonitoredwithBISandoutcomeswereanalyzedduetodifferentanesthetic
regimens.Thestudygoesoutoffocus---BISinterventioncomparedtothecontrolgroup (consciousnessguidedbyclinicalparametersonly).
Nakayamaetal.(2002)21 AllpatientsweremonitoredwithBISandoutcomeswereanalyzedduetodifferentanesthetic
regimens(onlypropofolorpropofolandfentanyl).Thestudygoesoutoffocus---BIS interventioncomparedtothecontrolgroup(consciousnessguidedbyclinicalparameters only).
Lehmannetal.(2002)22 AllpatientsweremonitoredwithBISandanalyzedoutcomesresultingfromdifferent
anesthetictechniques(withmanualpropofolinfusionvs.propofolinTargetControlled Infusion---TCI).Thestudygoesoutoffocus---BISinterventioncomparedtothecontrolgroup (consciousnessguidedbyclinicalparametersonly).
Paventietal.(2002)23 AllpatientsweremonitoredwithBISandanalyzedoutcomesresultingfromdifferent
anesthetictechniques(manualpropofolinfusionvs.propofolinTCI).Thestudygoesoutof focus---BISinterventioncomparedtothecontrolgroup(consciousnessguidedbyclinical parametersonly).
Lehmannetal.(2003)24 AllpatientsweremonitoredwithBIS(groupBIS50andgroupBIS40).Thestudygoesoutof
focus---BISinterventioncomparedtothecontrolgroup(consciousnessguidedbyclinical parametersonly).
Yamaguchietal.(2003)25 AllpatientsweremonitoredwithBISandanalyzedoutcomesresultingfromdifferent
anestheticdrugsandtechniques(propofolgroup/ivinductionandsevofluranegroupwith inhalationalinductioninadultbythevitalcapacitytechnique).Thestudygoesoutoffocus ---BISinterventioncomparedtothecontrolgroup(consciousnessguidedbyclinicalparameters only).
Buyukkocaketal.(2003)26 AllpatientsweremonitoredwithBISandoutcomeswereanalyzedduetodifferentanesthetic
drugs,fourdifferentmethodsofsedationassociatedwithtopicalanesthesia.Thestudygoes outoffocus---BISinterventioncomparedtothecontrolgroup(consciousnessguidedby clinicalparametersonly).
Forestieretal.(2003)27 AllpatientsweremonitoredwithBISandanalyzedfivegroupswithdifferentconcentrationsof
sufentanil.Thestudygoesoutoffocus---BISinterventioncomparedtothecontrolgroup (consciousnessguidedbyclinicalparametersonly).
Schneideretal.(2003)28 AllpatientsweremonitoredwithBISandanalyzedfourdifferentanestheticregimens.The
studygoesoutoffocus---BISinterventioncomparedtothecontrolgroup(consciousness guidedbyclinicalparametersonly).
Schneideretal.(2003)29 AllpatientsweremonitoredwithBISandanalyzedtwodifferentanestheticregimens.The
studygoesoutoffocus---BISinterventioncomparedtothecontrolgroup(consciousness guidedbyclinicalparametersonly).
Liu(2004)30 Meta-analysis.Thecriteriaforinclusioninthesystematicreviewwererandomizedcontrolled
trials.
Baueretal.(2004)31 AllpatientsweremonitoredwithBISandanalyzedtwodifferentanestheticregimens(TCIvs.
manualpropofolinfusion).TheBISwasusedbutisnotdescribedwhetheritwasblinded.The studygoesoutoffocus---BISinterventioncomparedtothecontrolgroup(consciousness guidedbyclinicalparametersonly).
Bestasetal.(2004)32 All50patients(twogroupsof25)weremonitoredwithBISandwereblinded,withanalysisof
twodifferentanestheticregimes.Thestudygoesoutoffocus---BISinterventioncomparedto thecontrolgroup(consciousnessguidedbyclinicalparametersonly).
Boztugetal.(2006)33 Articlenotfound.
Purietal.(2007)34 AllpatientsweremonitoredwithBIS,withanalysisoftwodifferenttypesofpropofolinfusion.
Table3 (Continued)
Article Reasonofexclusion
Lindholmetal.(2008)35 ThepaperanalyzesthedegreeofproficiencyinhandlingtheBISbynurses’anesthetists.The
studygoesoutoffocus---BISinterventioncomparedtothecontrolgroup(consciousness guidedbyclinicalparametersonly).
Avidanetal.(2008)36 Inthecontrolgroup,anesthesiawasmaintainedwithBIS‘‘blinded’’butwithanexpired
fractionof0.7---1.3minimumalveolarconcentrationofinhaledanesthetic.
Bejjanietal.(2009)37 AllpatientsweremonitoredwithBISwithmemoryprocessinganalysis.Thestudygoesoutof
focus--- BISinterventioncomparedtothecontrolgroup(consciousnessguidedbyclinical parametersonly).
Delfinoetal.(2009)38 AllpatientsweremonitoredwithBISorcerebralstateindex,withanalysisofpropofolinfusion
withthesetwotypesofmonitoring.Thestudygoesoutoffocus---BISinterventioncompared tothecontrolgroup(consciousnessguidedbyclinicalparametersonly).
Kerssensetal.(2009)39 Studyofintraoperativememoryandretrievalofwordsheardduringthetrans-operative,
throughmemorytestspostoperatively.
Mashouretal.(2009)40 Cohortstudy.Thecriteriaforinclusioninthesystematicreviewwererandomizedcontrolled
trials.
Satishaetal.(2010)41 Cohortstudy.Thecriteriaforinclusioninthesystematicreviewwererandomizedcontrolled
trials.
Meybohmetal.(2010)42 Protocolstudy.Thecriteriaforinclusioninthesystematicreviewwererandomizedcontrolled
trials.
Leslieetal.(2010)43 Retrospectivecohortstudy.Thecriteriaforinclusioninthesystematicreviewwere
randomizedcontrolledtrials.
Avidanetal.(2009)44 Protocolstudy.Thecriteriaforinclusioninthesystematicreviewwererandomizedcontrolled
trials.
Ellerkmannetal.(2010)45 Inhalationorintravenousanesthesia,complementedbyregionalanesthesia(combined
anesthesia).Thestudygoesoutoffocus---BISinterventioncomparedtothecontrolgroup (consciousnessguidedbyclinicalparametersonly).
Yufuneetal.(2011)46 The38patientsweremonitoredwithBISandoutcomeswereanalyzedduetodifferent
anestheticregimens,aswellasdifferentconcentrationsofremifentanil.Thestudygoesout offocus---BISinterventioncomparedtothecontrolgroup(consciousnessguidedbyclinical parametersonly).
Liuetal.(2011)47 AllpatientsweremonitoredwithBISandoutcomeswereanalyzedduetodifferentanesthetic
regimens,targetcontrolledinfusionofpropofolvs.closed-loopmanagement.Thestudygoes outoffocus---BISinterventioncomparedtothecontrolgroup(consciousnessguidedby clinicalparametersonly).
Avidanetal.(2011)48 Thecontrolgroupwasadjustedformaintaininganexpiredfractionof0.7---1.3minimum
alveolarconcentrationofinhaledanesthetic.
Aiméetal.(2012)49 The102patientsweremonitoredwithBISorEntropy,inbothgroups,thevalueswereblinded,
andanesthesiawasconductedbyclinicalparameters.Thestudygoesoutoffocus---BIS interventioncomparedtothecontrolgroup(consciousnessguidedbyclinicalparameters only).
Mashouretal.(2012)50 Thecontrolgroupwasblinded,butadjustedtoaminimumalveolarconcentrationofinhaled
anestheticbyage.
Persecetal.(2012)51 Theresultsofthisstudycannotbemeta-analyzedastheyprovidenostandarddeviation.
Fritzetal.(2013)52 Retrospectivecohortstudy.Thecriteriaforinclusioninthesystematicreviewwere
randomizedcontrolledtrials.
Villafrancaetal.(2013)53 Retrospectivecohortstudy.Thecriteriaforinclusioninthesystematicreviewwere
randomizedcontrolledtrials.
BIS,bispectralindex.
haveareductionof4.89min(95%CI−5.95,−3.83)withan
I2=0%, maintaining,therefore, statisticallysignificant
dif-ference(Fig.6).
The timefor patientstoachieve thedischarge criteria
inthe PACU(Aldrete-Kroulikmodified index)wasreduced
4.05min (95% CI−7.23,−0.87), withI2=91%.In
sensitiv-ity analysis, when removed the study Ibraheim et al.,13
wehaveareductionof22.35min(95%CI−31.01,−13.69)
withI2=20%,maintainingstatisticallysignificantdifference
(Fig.7).
Therewasnostatisticallysignificantdifferencebetween theinterventionandcontrolintheevaluationofthe neces-sarytimetohospitaldischarge(95%CI,−22.08,30.52)with
Study or Subgroup
Nelskylä KA 2001
Nelskylä KA 2001 Wong J 2002
Wong J 2002 Kreuer S 2003
Kreuer S 2003 Kreuer S 2005
Kreuer S 2005 Aimé I 2006
Aimé I 2006 Kamal NM 2009
Kamal NM 2009
Total (95% CI)
Total (95% CI)
Heterogeneity: Chi2=34.57, df=6 (P<.00001); I2=83%
Heterogeneity: Chi2=2.29, df=5 (P=.81); I2 = 0% Test for overall effect: Z=2.64 (P=.008)
Test for overall effect: Z=1.13 (P=.26)
275
235 241
281 100.0%
100.0% Bruhn J 2005
Bruhn J 2005
5
4
3.5 2.9 40 9.3 5.2 40
3.5 2.9 40 9.3 5.2 40
5.6 2.5 58
4.7 2.2 40
3.9 54
1.9 28
–10 –5 0 5 10
–10 –5 0 5 10
58 40 54 28 8
4.4 71 3.4
2.1 40
4.1 34
1.6 29
5.9
5.6 2.5 71
3.4 5.9 4.2
4.7 2.2
2.1 40
4.2 7.6
3.9 8
4.1 34
7.6 4.1
1.9 4.4
1.6 29
4.1
2.1 29
5 32 5
4.9 3.4 31
4 2.1 29 4.9 3.4 31
2 30
5 5 32 5 2 30
6.1% 2001
2002
2003 2005 2005
2006 2009
2001 2002 2003 2005 2005 2006 2009 10.6%
6.3% 20.5%
24.0% 7.1% 25.5%
6.5% 11.3% 0.0% 21.9% 25.6% 7.6% 27.2%
0.00 [–1.87, 1.87] –0.90 [–2.32, 0.52]
–5.80 [–7.65, –3.95] 0.30 [–0.72, 1.32] –0.50 [–1.44, 0.44]
–0.40 [–2.13, 1.33] –0.30 [–1.21, 0.61]
0.00 [–1.87, 1.87] –0.90 [–2.32, 0.52] –5.80 [–7.65, –3.95] 0.30 [–0.72, 1.32] –0.50 [–1.44, 0.44] –0.40 [–2.13, 1.33] –0.30 [–1.21, 0.61] –0.62 [–1.08, –0.16]
–0.28 [–0.75, 0.20]
Mean SDTotal Mean SD Total Weight Year
Year
IV, Fixed, 95% CI IV, Fixed, 95% CI
BIS Control Mean difference
Study or Subgroup Mean SDTotal Mean SD Total Weight IV, Fixed, 95% CI
BIS Control Mean difference
Mean difference
IV, Fixed, 95% CI Mean difference
BIS Control BIS Control
Figure2 Timeforspontaneouseyeopening(min).
TheincidenceofPONVwaslowerinanesthesiaconducted
withBIS,withariskreductionof12%(95%CI−0.22,−0.01)
withI2=61%,whichwasstatisticallysignificant(Fig.9).
Therewasnoriskreductionofcognitivedisordersinthe
post operatorywith 1 week after extubation, in patients
usingBIS(95%CI,−0.06,0.01,I2=0%).Therewasno
statis-ticallysignificant differencebetweentheinterventionand control(Fig.10).
The cognitivedisordersaftersurgeryat 3monthsafter
extubationhadariskreductionof3%(95%CI−0.05,−0.00),
andI2=52%,whichwasstatisticallysignificant(Fig.11).
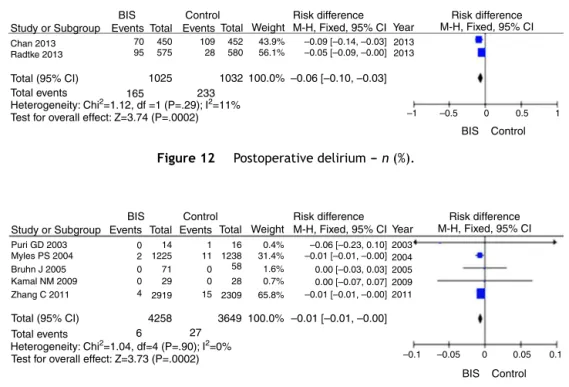
There was a 6% reduction in the risk of delirium in
thepost operatoryin patients monitoredwithBIS(95% CI
−0.10, −0.03) I2=11%, which was statistically significant
(Fig.12).
TheuseofBIShadariskreductionof1%forthe intraoper-ativememory(Recall),astatisticallysignificantdifference (−0.01[95%CI,−0.01,−0.00])withI2=0%.The
intraoper-ativememoryis the awakeningconfirmedby the patient.
Itwasnotmade adifferentiation ofstudies withpatients
classified as low or high risk for intraoperative memory
(Fig.13).
Discussion
The use of monitoring with the BIS showed benefits by
reducingthetimetoextubationin0.87min,orientationin
timeandplacein 3.76min and leavingoperating roomin
4.89min.Patientshadareductionin22.35mintoreachthe
criteriafor PACU discharge. The combined results of the
studiesshowed thatthe incidenceof PONV riskreduction
of12%inpatientsBISmonitoring.
Cognitive disorders in postoperative patients with 1
week after extubation did not show statistically
signifi-cantdifference.However,therewasa3%reductioninthe
risk of cognitive disorders in the postoperative patients
Study or Subgroup
Total (95% CI) 59 61 100.0% –0.63 [–1.30, 0.05]
BIS Control Mean
Basar H 2003 8.25
18.5
6.8 2.1 15 8.66
2.6 15 15.9%
11.5 14 28 16 0.5%–9.50 [–19.00, 0.00]
–1.86 [–3.55, 0.17] 15
1.8 30 8.59 1 30 83.6% –0.34 [–1.08, 0.40] 2003
2008 2003 Puri GD 2003
Ibraheim O 2008
Heterogeneity: Chi2=5.97, df=2 (P=.05); I2=67%
–10 –5 0 5 10
Test for overall effect: Z=1.82 (P=.07)
Mean
SDTotal SDTotal Weight IV, Fixed, 95% CIYear IV, Fixed, 95% CI
BIS Control Mean difference Mean difference
Study or Subgroup
Total (95% CI)
Total (95% CI)
355 315 361 321 100.0% 100.0%
–1.18 [–1.65, –0.70]
–0.87 [–1.36, –0.38]
Nelskylä KA 2001 2
6.8 4.6 40 10.5 5.9 40 4.2%
4.4% 3.0% 6.5% 9.8% 21.8% 2.6% 7.2% 17.4% 40 16 40 40 58 54 15 28 6.1 3.2 5.3 4.4 2.4 9 2.9 2.3 8.3 6 9.7 5.4 6.3 14.2 11.8 4.8 4.1 40 14 40 40 71 34 15 29 4.3 2.9 2.2 3.5 5.1 2 2.1 6.5 7.2 4.1 4.4 6.6 11.1 9.26 4.3
2 32 3 2
2
6.8
4.6
40 10.5
5.9
6.1 3.2 5.3 4.4 2.4 9 2.9 2.3 8.3 6 9.7 5.4 6.3 14.2 11.8 4.8 4.1 40 14 40 40 71 34 15 29 4.3 2.9 2.2 3.5 5.1 2 2.1 6.5 7.2 4.1 4.4 6.6 11.1 9.26 4.3
2
32 3
2 30 40 40 16 40 40 58 54 15 28 30 23.0% 24.6% 4.5% 4.7% 3.2% 0.0% 10.5% 23.4% 2.8% 18.6%
–10 –5 0 5 10
7.7%
–1.00 [–2.00, –0.00]
–1.00 [–2.00, –0.00] –3.70 [–6.02, –138]
–3.70 [–6.02, –138] –1.80 [–4.08, 0.48] 1.20 [–1.54, 3.94]
–5.60 [ –7.47, –3.73] –1.00 [–2.52, 0.52]
0.30 [–0.72, 1.32] –3.10 [–6.05, –0.15] –2.54 [–4.32, –0.76] –0.50 [–1.64, 0.64]
2001 2003 2003 2003 2003 2005 2005 2006 2008 2009 2001 2003 2003 2003 2003 2005 2005 2006 2008 2009 –1.80 [–4.08, 0.48]
1.20 [–1.54, 3.94]
–5.60 [ –7.47, –3.73]
–1.00 [–2.52, 0.52] 0.30 [–0.72, 1.32]
–3.10 [–6.05, –0.15] –2.54 [–4.32, –0.76]
–0.50 [–1.64, 0.64] Luginbühl M, 2003 (a)
Luginbühl M, 2003 (b) Puri GD 2003 Kreuer S 2003 Kreuer S 2005 Bruhn J 2005 Aimé I 2006 Ibraheim O 2008 Kamal NM 2009
Nelskylä KA 2001 Luginbühl M, 2003 (a)
Luginbühl M, 2003 (b)
Puri GD 2003 Kreuer S 2003
Kreuer S 2005 Bruhn J 2005
Aimé I 2006 Ibraheim O 2008
Kamal NM 2009
Heterogeneity: Chi2=42.58, df=9 (P<.00001); I2=79%
–10 –5 0 5 10
Test for overall effect: Z=4.83 (P<.00001)
Heterogeneity: Chi2=19.65, df=8 (P=.01); I2=59% Test for overall effect: Z=3.45 (P=.0006)
Mean SD TotalMean SDTotal Weight IV, Fixed, 95% CI Year IV, Fixed, 95% CI
BIS Control Mean difference Mean difference
Study or Subgroup MeanSD TotalMeanSDTotal Weight IV, Fixed, 95% CIYear IV, Fixed, 95% CI
BIS
Control Mean difference Mean difference
BIS Control
BIS Control
Figure4 Timetotrachealextubation(min).Luginbühl(2003)studiedwithinasingleoutcome,twodifferentanestheticregimens withpropofol(a)anddesflurane(b).
3 months after extubation. There was a 6% reduction in
theriskof deliriumincidenceof postoperativeinpatients
using BIS monitoring. In addition, the memory of the
intraoperative risk had a reduction of 1% after using
BIS.
The 17 studies selected by the pre-established
crite-riashowedaheterogeneitythatwassoonnoticed.Factors
related toanesthetic technique,the patientand the
sur-gical procedure wereobserved. Studiesthat analyzed the
consumptionofanesthetics showednostandardized
meas-Study or Subgroup
Mean
SDTotal MeanSDTotal Weight IV, Fixed, 95% CIYear IV, Fixed, 95% CI
BIS
Control Mean difference Mean difference
Study or Subgroup Mean SDTotal MeanSDTotal Weight IV, Fixed, 95% CIYear IV, Fixed, 95% CI
BIS Control Mean difference Mean difference
Nelskylä KA 2001 Wong J 2002
6 9.5 7.4 2 3.1 1.5 32 29 29 3 2 3.8 13.1 11.2 1.9
30 38.8% –2.00 [–3.00, –1.00] –3.60 [–5.35, –1.85] –3.80 [–4.69, –2.91]
2001 2002 2009 2001 2002 2009 12.6% 48.6%
–10 –5 0 5 10
28 31 Kamal NM 2009
Nelskylä KA 2001 Wong J 2002
2 9.5 7.4 2 3.1 1.5 32 29 29 3 2 3.8 13.1 11.2 1.9
30 0.0% –2.00 [–3.00, –1.00] –3.60 [–5.35, –1.85] –3.80 [–4.69, –2.91] 20.6%
79.4% 28 31 Kamal NM 2009
Total (95% CI) 90 89 100.0%–3.08 [–3.70, –2.45]
Heterogeneity: Chi2=7.36, df=2 (P=.03); I2=73% Test for overall effect: Z=9.71 (P<.00001)
Total (95% CI) 58 59 100.0% –3.76 [–4.55, –2.97]
Heterogeneity: Chi2=.04, df=1 (P=.84); I2=0%
Test for overall effect: Z= 9.28 (P<.00001) –10 –5 0 5 10
BIS Control BIS Control
Study or Subgroup Mean SDTotalMean SDTotal Weight IV, Fixed, 95% CI Year IV, Fixed, 95% CI
BIS Control Mean difference Mean difference
40 40
40
40 Kreuer S 2003
Kreuer S 2005
9.4 8.4 7
9.4 8.4 7
1.9 2.4 3.2
1.9 2.4 3.2
29
40
40 29
14.1 9.4 12.4
14.1 9.4 12.4
2.8 2.4 5.7
2.8 2.4 5.7
–4.70 [–5.95, –3.45] –1.00 [–2.05, 0.05] –5.40 [–7.43, –3.37]
2009 2005 2003
2009 2005 2003
–4.70 [–5.95, –3.45] –1.00 [–2.05, 0.05] –5.40 [–7.43, –3.37] 35.9%
72.5% 0.0% 27.5% 50.5% 13.6%
28 40 40 28 Kamal NM 2009
Kreuer S 2003
Kreuer S 2005 Kamal NM 2009
Total (95% CI) 109 108100.0% –2.93 [–3.68, –2.18]
Heterogeneity: Chi2=26.39, df=2 (P<.00001); I2=92% Test for overall effect: Z=7.68 (P<.00001)
Total (95% CI) 69 68 100.0% –4.89 [–5.95, –3.83]
Heterogeneity: Chi2=.33, df=1 (P<.56); I2=0%
Test for overall effect: Z=9.03 (P<.00001)
Study or Subgroup Mean SDTotalMean SD Total Weight IV, Fixed, 95% CI Year IV, Fixed, 95% CI
BIS Control Mean difference Mean difference
–10 –5 0 5 10
–10 –5 0 5 10
BIS Control BIS Control
Figure6 Timeforleavingoperationroom(min).
Wong J 2002 111 30 29 123 48 31 2.5% –12.00 [–32.12, 8.12]
Wong J 2002 111 30 29 123 48 31 18.5% –12.00 [–32.12, 8.12] 86.5%
15 4.81 31 15 4.74
29.8 –1.20 [–4.62, 2.22]
Ibraheim O 2008
0.0% 15 4.81 31 15 4.74
29.8 –1.20 [–4.62, 2.22]
Ibraheim O 2008
11.0% 28 21.5 78.6 29 14.7
53.9 –24.70 [–34.29, –15.11]
2002 2008 2009
2002 2008 2009 Kamal NM 2009
81.5% 28 21.5 78.6 29 14.7
53.9 –24.70 [–34.29, –15.11]
Kamal NM 2009
Total (95% CI) 73 74 100.0% –4.05 [–7.23, –0.87]
Heterogeneity: Chi2=21.07, df=2 ( P<.0001); I2=91%
Test for overall effect: Z=2.50 (P=.01)
Total (95% CI) 58 59 100.0% –22.35 [–31.01, –13.69]
Heterogeneity: Chi2=1.25, df=1 ( P=.26); I2=20%
Test for overall effect: Z=5.06 (P<.00001)
Study or Subgroup Mean SDTotalMean SD Total Weight IV, Fixed, 95% CI Year IV, Fixed, 95% CI
BIS Control Mean difference Mean difference
Study or Subgroup Mean SDTotalMean SDTotal Weight IV, Fixed, 95% CI Year IV, Fixed, 95% CI
BIS Control Mean difference Mean difference
BIS Control
–100 –50 0 50 100
BIS Control
–100 –50 0 50 100
Figure7 TimefordischargefromPACU(min).
uresthatenabledtheselection ofatleasttwostudiesfor
themeta-analysis.
The study Ibraheim et al.13 involved morbidly obese
patients. Three studies were conducted exclusively with
patientsover60yearsofage.2,16,17
Purietal.6andVretzakisetal.11studiedpatients under-goingcardiacsurgerywithextracorporealcirculation.
Mylesetal.8studiedpatientswithatleastonehigh-risk
factor for awakening with intraoperative memories (high
risk heart surgery, cesarean sections, hypovolemic shock,
rigidbronchoscopy,cardiovascularinstabilityandexpected hypotensionduringsurgery,lungdiseaseinadvancedstages, historicalofawakeningwithintraoperativememories,
dif-ficult airway, high consumption of alcohol, chronic use
Study or Subgroup Mean SDTotal Mean SD Total Weight IV, Fixed, 95% CI IV, Fixed, 95% CI
BIS Control Mean difference Mean difference
Nelskylä KA 2001
Ahmad S 2003
306 85 32 298 124 30 24.4%
203 78 49 200 74 48 75.6%
8.00 [–45.26, 61.26]
3.00 [–27.25, 33.25]
Year
2001
2003
Total (95% CI)
Heterogeneity: Chi2=0.03, df=1 (P=.87); I2=0%
Test for overall effect: Z=0.31 (P=.75)
81 78 100.0% 4.22 [–22.08, 30.52]
–100 –50 0 50 100
BIS Control
Study or Subgroup EventsTotal EventsTotal Weight M-H, Fixed, 95% CI M-H, Fixed, 95% CI
BIS Control Risk difference Risk difference
Nelskylä KA 2001 Bruhn J 2005
5 32 12 30 32.7%
6 71 8 58 67.3%
–0.24 [–0.46, –0.03] –0.05 [–0.16, 0.06]
Year
2001 2005
Total (95% CI)
Total events
Heterogeneity: Chi2=2.59, df=1 (P=.11); I2=61% Test for overall effect: Z=2.22 (P=.03)
103
11
88
20
100.0% –0.12 [–0.22, –0.01]
–1 –0.5 0 0.5 1
BIS Control
Figure9 Postoperativenauseaandvomiting(PONV)---n(%).
Study or Subgroup Events Total Events Total Weight M-H, Fixed, 95% CI M-H, Fixed, 95% CI
BIS Control Risk difference Risk difference
Chan 2013 Radtke 2013
98 70
450 104 452 43.9% –0.01 [–0.07, 0.04]
575 90 580 56.1% –0.03 [–0.07, 0.01]
Total events
Heterogeneity: Chi2=.39, df=1 (P=.53); I2=0% Test for overall effect: Z=1.45 (P=.15)
168 194
–1 –0.5 0 0.5 1
BIS Control
Total (95% CI) 1025 1032 100.0% –0.02 [–0.06, 0.01]
Figure10 Cognitivedisordersinthepostoperativeperiod(1weekafterextubation)---n(%).
Study or Subgroup Events Total Events Total Weight M-H, Fixed, 95% CI M-H, Fixed, 95% CI
BIS Control Risk difference Risk difference
Chan 2013 Radtke 2013
46 21
450 66 452 43.9% –0.04 [–0.09, –0.00]
575 28 580 56.1% –0.01 [–0.03, 0.01]
Total events
Heterogeneity: Chi2=2.08, df=1 (P=.15); I2=52% Test for overall effect: Z=2.21 (P=.03)
67 94
–0.5 –0.25 0 0.25 0.5
BIS Control Total (95% CI) 1025 1032 100.0% –0.03 [–0.05, –0.00]
Figure11 Cognitivedisordersinthepostoperativeperiod(3monthsafterextubation)---n(%).
Study or Subgroup EventsTotal EventsTotal Weight M-H, Fixed, 95% CI M-H, Fixed, 95% CI
BIS Control Risk difference Risk difference
Chan 2013 Radtke 2013
70 95
450 109 452 43.9% –0.09 [–0.14, –0.03] 575 28 580 56.1% –0.05 [–0.09, –0.00]
Year
2013 2013
Total events
Heterogeneity: Chi2=1.12, df =1 (P=.29); I2=11%
Test for overall effect: Z=3.74 (P=.0002)
165 233
–1 –0.5 0 0.5 1
BIS Control
Total (95% CI) 1025 1032 100.0% –0.06 [–0.10, –0.03]
Figure12 Postoperativedelirium---n(%).
Study or Subgroup Events Total Events Total Weight M-H, Fixed, 95% CI M-H, Fixed, 95% CI
BIS Control Risk difference Risk difference
Puri GD 2003 Myles PS 2004 Bruhn J 2005 Kamal NM 2009 Zhang C 2011
0 2 0
14 1 16 0.4% –0.06 [–0.23, 0.10] 1225
71 29 2919 0 4
11 0 0 15
1238 58 28 2309
31.4% 1.6% 0.7% 65.8%
–0.01 [–0.01, –0.00] 0.00 [–0.03, 0.03] 0.00 [–0.07, 0.07] –0.01 [–0.01, –0.00]
2003 2004 2005 2009 2011
Total events
Heterogeneity: Chi2=1.04, df=4 (P=.90); I2=0%
Test for overall effect: Z=3.73 (P=.0002)
6 27
–0.1 –0.05 0 0.05 0.1
BIS Control
Total (95% CI) 4258 3649 100.0% –0.01 [–0.01, –0.00]
Year
of benzodiazepines or opioids and therapy with protease inhibitors).
The outcomes analyzed with continuously variable
relatedtothe timeof recovery anddischarge ofpatients
were:timeforspontaneouseyeopening,timeforeye
open-ing upon verbal command, time for extubation, time for
orientation in time and place, time for leaving operating
room, timefor PACUdischarge and time for hospital
dis-charge.
The outcomes of dichotomous variable, related to
adverseeventswerePONV,cognitivedisordersinthe
post-operative 1 week after extubation, cognitive disordersin
thepostoperative3monthsafterextubation,postoperative
deliriumandintraoperativememory.
Some primary studies contributed only one outcome
analyzed.3---5,11,15
The individualizationof outcomesderivedfromstudies
involvingbalancedanesthesiaortotalintravenous
anesthe-siawasnotmade.
Clinically,thecostofimplementationofBISmonitoring canbejustifiedbyallowingadvantagesinthemaintenance ofambulatorysurgeriesaswellasinthetechniquesofearly
awakening and especially it can reduce the incidence of
adverseevents.
The cost of thedisposable electrodeis a causeof
dis-cussionaboutthevalueinuseofBIS.Thus,itisimportant
the active participation of professionals, primarily with
healthadministrators,indevelopingapolicyplanthat opti-mizeresourcesandgivegreatersafetyandcomfortforthe patients.
Sofar,thereisnogoldstandardtospantheentire spec-trumofanestheticeffectonthecentralnervoussystem,and theBISisundoubtedlythemoststudied,butisoneofmany
monitorsderivedfromEEGusednowadays.Monitoringthe
depthof anesthesiaasnewtechnologyisin itsbeginning. Thenewboundaryistheindividualizationofmonitoringthe hypnoticanditseffectsonthecentralnervoussystem.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.NelskyläKA,Yli-HankalaAM,PuroPH,etal.Sevoflurane titra-tionusing bispectral index decreasespostoperativevomiting inphaseIIrecovery afterambulatory surgery.Anesth Analg. 2001;93:1165---9.
2.WongJ,SongD,BlanshardH,etal.Titrationofisofluraneusing BISindeximprovesearlyrecoveryofelderlypatientsundergoing orthopedicsurgeries.CanJAnaesth.2002;49:13---8.
3.LuginbühlM,WüthrichS,Petersen-FelixS,etal.Different bene-fitofbispectalindex(BIS)indesfluraneandpropofolanesthesia. ActaAnaesthesiolScand.2003;47:165---73.
4.AhmadS,YilmazM,MarcusRJ,etal.Impactofbispectralindex monitoringonfasttrackingofgynecologicpatientsundergoing laparoscopicsurgery.Anesthesiology.2003;98:849---52. 5.Bas¸arH, Ozcan S, Buyukkocak U, et al. Effect ofbispectral
indexmonitoringonsevofluraneconsumption.EurJ Anaesthe-siol.2003;20:396---400.
6.Puri GD, Murthy SS. Bispectral index monitoring in patients undergoingcardiacsurgeryundercardiopulmonarybypass.Eur JAnaesthesiol.2003;20:451---6.
7.Kreuer S, Biedler A, Larsen R, et al. Narcotrend moni-toring allows faster emergence and a reduction of drug consumptioninpropofol-remifentanilanesthesia. Anesthesiol-ogy.2003;99:34---41.
8.MylesPS,LeslieK,McNeilJ,etal.Bispectralindexmonitoringto preventawarenessduringanaesthesia:theB-Awarerandomised controlledtrial.Lancet.2004;363:1757---63.
9.BruhnJ,KreuerS,BischoffP,etal.BispectralindexandA-line AAIindexasguidancefordesflurane-remifentanilanaesthesia comparedwithastandardpracticegroup:amulticentrestudy. BrJAnaesth.2005;94:63---9.
10.KreuerS,BruhnJ,StrackeC,etal.Narcotrendorbispectral indexmonitoringduringdesflurane-remifentanilanesthesia:a comparisonwitha standardpractice protocol.AnesthAnalg. 2005;101:427---34.
11.VretzakisG,FerdiE,ArgiriadouH,etal.Influenceofbispectral indexmonitoringondecisionmakingduringcardiacanesthesia. JClinAnesth.2005;17:509---16.
12.Aimé I, VerroustN, Masson-Lefoll C, et al. Does monitoring bispectral indexor spectral entropy reducesevoflurane use? AnesthAnalg.2006;103:1469---77.
13.Ibraheim O, Alshaer A, Mazen K, et al. Effect of bispec-tral index (BIS) monitoring on postoperative recovery and sevofluraneconsumptionamongmorbidlyobesepatients under-goinglaparoscopicgastricbanding.MiddleEastJAnesthesiol. 2008;19:819---30.
14.KamalNM,OmarSH,RadwanKG,etal.Bispectralindex moni-toringtailorsclinicalanestheticdeliveryandreducesanesthetic drugconsumption.JMedSci.2009;9:10---6.
15.ZhangC,XuL,MaYQ,etal.Bispectralindexmonitoringprevent awarenessduringtotalintravenousanesthesia:aprospective, randomized,double-blinded,multi-centercontrolledtrial.Chin MedJ(Engl).2011;124:3664---9.
16.Chan MT, Cheng BC, Lee TM, et al. BIS-guided anesthesia decreasespostoperativedeliriumandcognitivedecline.J Neu-rosurgAnesthesiol.2013;25:33---42.
17.Radtke FM,FranckM, Lendner J,et al. Monitoringdepthof anaesthesiainarandomizedtrialdecreasestherateof postop-erativedeliriumbutnotpostoperativecognitivedysfunction.Br JAnaesth.2013;110Suppl.1:i98---105.
18.SebelPS,LangE,RampilIJ,etal.Amulticenterstudyof bispec-tral electroencephalogramanalysisfor monitoringanesthetic effect.AnesthAnalg.1997;84:891---9.
19.Yli-HankalaA,VakkuriA,AnnilaP,etal.EEGbispectralindex monitoringinsevofluraneorpropofolanaesthesia:analysisof directcostsandimmediaterecovery.ActaAnaesthesiolScand. 1999;43:545---9.
20.MiWD,SakaiT,SinghH,etal.Hypnoticendpointsvs.the bispec-tralindex,95%spectraledgefrequencyandmedianfrequency duringpropofolinfusionwithorwithoutfentanyl.EurJ Anaes-thesiol.1999;16:47---52.
21.Nakayama M, Ichinose H, Yamamoto S, et al. The effect of fentanyl on hemodynamic and Bispectral Index changes during anesthesia induction with propofol. J Clin Anesth. 2002;14:146---9.
22.LehmannA,BoldtJ,ThalerE,etal.BispectralIndexinpatients withtarget-controlledormanually-controlledinfusionof propo-fol.AnesthAnalg.2002;95:639---44.
23.PaventiS,SantevecchiA,PerilliV,etal.Effectsofremifentanil infusion BIS-titratedon earlyrecovery for obese outpatients undergoinglaparoscopiccholecystectomy.MinervaAnestesiol. 2002;68:651---7.
25.YamaguchiS,EgawaH,MishioM,etal.Bispectralmonitoring duringvital capacityrapidinhalationinduction with sevoflu-rane.JClinAnesth.2003;15:24---8.
26.Buyukkocak U, Ozcan S, Daphan C, et al. A compari-son of four intravenous sedation techniques and Bispectral Indexmonitoringinsinonasalsurgery.AnaesthIntensiveCare. 2003;31:164---71.
27.ForestierF,HirschiM,RougetP,etal.Propofolandsufentanil titration withtheBispectral Index to provide anesthesia for coronaryarterysurgery.Anesthesiology.2003;99:334---46. 28.SchneiderG,GelbAW,SchmellerB,etal.Detectionof
aware-ness in surgical patients with EEG-based indices-bispectral indexandpatientstateindex.BrJAnaesth.2003;91:329---35. 29.Schneider G, Elidrissi C, Sebel PS. Bispectral index-guided
administrationof anaesthesia:comparison between remifen-tanil/propofolandremifentanil/isoflurane.EurJAnaesthesiol. 2003;20:624---30.
30.Liu SS.Effectsof BispectralIndex monitoringonambulatory anesthesia.Anesthesiology.2004;101:311---5.
31.BauerM, Wilhelm W, Kraemer T, etal. Impact ofBispectral Indexmonitoringonstressresponseandpropofolconsumption inpatientsundergoingcoronaryarterybypasssurgery. Anesthe-siology.2004;101:1096---104.
32.BestasA, YasarMA,BayarMK,etal. Theeffectsoftwo dif-ferentanaesthesiatechniquesonbispectralindexvaluesand awarenessduringoff-pumpcoronaryarterybypassgrafting.J ClinMonitComput.2004;18:347---51.
33.Boztug N,BigatZ,Akyüz M,et al.Doesusing theBispectral Index(BIS)duringcraniotomyaffectthequalityofrecovery?J NeurosurgAnesthesiol.2006;18:1---4.
34.PuriGD,KumarB,AveekJ.Closed-loopanaesthesiadelivery sys-tem(CLADS)usingbispectralindex:aperformanceassessment study.AnaesthIntensiveCare.2007;35:357---62.
35.LindholmML,BrudinL,SandinRH.Bispectralindexmonitoring: appreciatedbutdoesnotaffectdrugdosingandhypnoticlevels. ActaAnaesthesiolScand.2008;52:88---94.
36.AvidanMS,ZhangL,BurnsideBA,etal.Anesthesiaawareness andtheBispectralIndex.NEnglJMed.2008;358:1097---108. 37.BejjaniG,LequeuxPY,SchmartzD,etal.Noevidenceof
mem-ory processingduringpropofol-remifentanil target-controlled infusionanesthesiawithBispectralIndexmonitoringincardiac surgery.JCardiothoracVascAnesth.2009;23:175---81. 38.DelfinoAE,CortinezLI,FierroCV,etal.Propofolconsumption
andrecoverytimesafterbispectralindexorcerebralstateindex guidanceofanaesthesia.BrJAnaesth.2009;103:255---9. 39.Kerssens C, Gaither JR, Sebel PS. Preserved memory
func-tion during Bispectral Index-guided anesthesia with sevoflu-rane for major orthopedic surgery. Anesthesiology. 2009; 111:518---24.
40.MashourGA,TremperKK,AvidanMS.Protocolforthe‘‘Michigan Awareness Control Study’’: a prospective, randomized, con-trolled trialcomparing electronic alertsbased on bispectral index monitoringor minimumalveolarconcentrationfor the prevention of intraoperative awareness. BMC Anesthesiol. 2009;9:7.
41.SatishaM, SandersGM, BadrinathMR, et al.Introduction of bispectralindexmonitoringinadistrictgeneralhospital operat-ingsuite:aprospectiveauditofclinicalandeconomiceffects. EurJAnaesthesiol.2010;27:196---220.
42.MeybohmP, GruenewaldM,Höcker J, etal. Correlationand agreementbetweenthebispectralindexvs.stateentropy dur-inghypothermic cardio-pulmonary bypass. Acta Anaesthesiol Scand.2010;54:169---75.
43.LeslieK,MylesPS,ForbesA,etal.TheeffectofBispectralIndex monitoringonlong-termsurvivalintheB-Awaretrial.Anesth Analg.2010;110:816---22.
44.AvidanMS,PalancaBJ,GlickD,et al.Protocol forthe BAG-RECALLclinicaltrial:aprospective,multi-center,randomized, controlledtrialtodeterminewhetherabispectralindex-guided protocolis superiorto ananesthesia gas-guided protocol in reducingintraoperativeawarenesswithexplicitrecallinhigh risksurgicalpatients.BMCAnesthesiol.2009;9:8.
45.EllerkmannRK, Soehle M, Riese G, et al. The Entropy Mod-uleandBispectralIndexasguidanceforpropofol-remifentanil anaesthesiaincombinationwithregionalanaesthesiacompared withastandardclinicalpracticegroup.AnaesthIntensiveCare. 2010;38:159---66.
46.YufuneS,Takamatsu I,MasuiK,et al.Effectofremifentanil onplasmapropofolconcentrationandbispectralindexduring propofolanaesthesia.BrJAnaesth.2011;106:208---14. 47.Liu N, Chazot T, Hamada S, et al. Closed-loop
coadmin-istration of propofol and remifentanil guided by Bispectral Index:arandomizedmulticenterstudy.AnesthAnalg.2011;112: 546---57.
48.AvidanMS,JacobsohnE,GlickD,etal.Preventionof intraoper-ativeawarenessinahigh-risksurgicalpopulation.NEnglJMed. 2011;365:591---600.
49.AiméI,GayatE,FermanianC,etal.Effectofageonthe com-parability ofbispectral and state entropy indices duringthe maintenanceofpropofol---sufentanilanaesthesia.BrJAnaesth. 2012;108:638---43.
50.MashourGA,ShanksA,TremperKK,etal.Preventionof intraop-erativeawarenesswithexplicitrecallinanunselectedsurgical population.Anesthesiology.2012;117:717---25.
51.PersecJ,PersecZ,KopljarM,etal.Effectofbispectralindex monitoringonextubationtimeand analgesic consumptionin abdominalsurgery:arandomisedclinicaltrial.SwissMedWkly. 2012;142:w13689.
52.FritzBA,RaoP,MashourGA,etal.Postoperativerecoverywith BispectralIndexversusanestheticconcentration-guided proto-cols.Anesthesiology.2013;118:1113---22.