REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
Official Publication of the Brazilian Society of Anesthesiology www.sba.com.brSPECIAL
ARTICLE
Brazilian
consensus
on
anesthetic
depth
monitoring
Consenso
brasileiro
sobre
monitorac
¸ão
da
profundidade
anestésica
Rogean
Rodrigues
Nunes
a,b,c,∗,
Neuber
Martins
Fonseca
c,d,e,
Claudia
Marques
Simões
c,f,
Deise
Martins
Rosa
g,h,i,
Enis
Donizete
Silva
j,
Sara
Lúcia
Cavalcante
b,k,
Cristiane
Gurgel
Lopes
b,l,m,
Luciana
Cadore
Stefani
n,oaGraduateCourseinMedicine,CentroUniversitárioChristus(UNICHRISTUS),Fortaleza,CE,Brazil bCET,HospitalGeraldeFortaleza,Fortaleza,CE,Brazil
cSociedadeBrasileiradeAnestesiologia(SBA),RiodeJaneiro,RJ,Brazil
dDisciplineofAnesthesiology,FaculdadedeMedicina,UniversidadeFederaldeUberlândia(UFU),Uberlândia,MG,Brazil eCETFMUFUberlândia,Uberlândia,MG,Brazil
fServic¸odeAnestesiologia,InstitutodoCâncerdoEstadodeSãoPaulo(ICESP),SãoPaulo,SP,Brazil gAnesthesiaServiceUnitII,InstitutoNacionaldoCâncer(INCA),RiodeJaneiro,RJ,Brazil
hCET,InstitutoNacionaldoCâncer(INCA),RiodeJaneiro,RJ,Brazil
iCursoSAVA,SociedadeBrasileiradeAnestesiologia(SBA),RiodeJaneiro,RJ,Brazil jSociedadeBrasileiradeAnestesiologiadoEstadodeSãoPaulo(SAESP),SãoPaulo,SP,Brazil kHospitalSãoCarlos,Fortaleza,CE,Brazil
lHospitalHaroldoJuac¸aba,InstitutodoCâncerdoCeará,Fortaleza,CE,Brazil mServic¸odeOncologia,HospitalSãoCarlos,Fortaleza,CE,Brazil
nDepartmentofSurgery,FaculdadedeMedicina,UniversidadeFederaldoRioGrandedoSul(UFRGS),PortoAlegre,RS,Brazil oCET,ServiceofAnesthesiaandPerioperativeMedicine,HospitaldeClinicasdePortoAlegre,PortoAlegre,RS,Brazil
Availableonline3November2015
Introduction
Oneofthemostimportantgainsinanesthesiawastherecent admissionthatlightanesthesia,awakening,intraoperative awareness,andmemoryareallrealproblemswith delete-riouspsychologicalconsequencesforasignificantportionof patients.1Ontheotherhand,deepanesthesiaappearstobe
associatedwithincreasedmorbidityandmortality.2
Maintaining the adequate level of anesthesia depth
is critical. Very superficial or deep depth levels can be
disastrous in both the short and long run. The patient
expects that the procedure be absolutely painless and
throughoutthesurgeryheisasleep,withoutanyperception
∗Correspondingauthor.
E-mail:[email protected](R.R.Nunes).
ormemoryofwhathappenedduringthatperiod.Itis impor-tanttoemphasize thatthis concept is appliedtogeneral
anesthesia,and apatient shouldalways bewell informed
if the anesthetic approach is a regional anesthesia with
sedation,asituationthatmayhaveawakeningepisodesnot associatedwithpainorimmobility.
Accidentalintraoperative awareness (AIA) is the unde-sirable outcome of insufficient anesthesia. Consciousness researchtakes intoaccounttheabilityof an individualto presentresponsestostimuliand/orcommands.
Cerebralmonitoringisnecessaryincurrentclinical prac-ticeofanesthesiology.Avoidingexcessanestheticdosesisof greatimportance,notonlybecausethereisthepossibility
of reducing the immediate adverse effects of
anesthet-ics,suchascardiovascularandrespiratorydepression,but alsotopreventcognitiveimpairmentin patientswithlow neuronalreserve.AIAisthemostfearedanesthetic compli-cationregardingtheimproperadministrationofanesthetic
http://dx.doi.org/10.1016/j.bjane.2015.10.001
agents.Autonomic signsarenotabletoguidethe adjust-mentofdrugs,astherearemanycomponentsoftheclinical contextthatinterferewithautonomicfunction.
This paper aimsto evaluate concepts related to
anes-thetic depth monitoring, as well as to show the current
evidence and present recommendations for the use of
intraoperative monitoring of brain electrical activity. The
recommendations may beadopted, modified, or rejected
accordingtoclinicalneedsandpossiblerestrictions.
Concepts
In order to prevent unintentional awakening and deep
anesthesia damage, the advancement in the field of
brainmonitoringandmoreadequate understandingofthe
neurobiologicalprocessesinvolvingconsciousnessand
mem-ory were necessary. For a proper understanding of this
approach,someconceptsareimportant:
(a) Awareness----a term with broad meaning. For
neuro-science, it translates the relationship between the
individualandtheenvironment,hisresponsesto exter-nalstimuliandself-perception.Ithastwocomponents: levelofconsciousnessandcontentofconsciousness.3
(b) Levelofconsciousness(arousal/wakefulness)----refersto thewakefulnessorasleepstate.Thereisanintegration ofcertainnucleipresent inbrainstem,hypothalamus, andbasalgangliathatwillinhibitorstimulatethecortex andthalamus,regulatingthesleep-wakecycle.4
(c) Contentofconsciousness(awareness)----referstotheset ofinformationestablishedinfunctionalbasesof corti-calandthalamic-corticalsystem.Whilethesubcortical structuresinteracttokeepthecortexawakeand stim-ulated, specific regions of the cortex have a role to processthecontentsofconsciousness.5
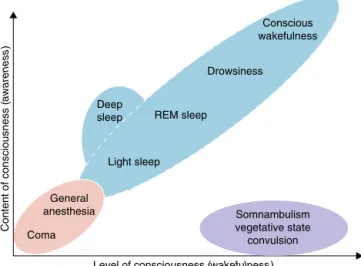
The level of consciousness may not be related to
thecontentofconsciousness.Acomatosepatienthasa reducedlevelandcontentofconsciousness.Patientsin avegetativestatehavetheirsleep-wakecyclesintact,
but compromised contentof consciousness, not being
abletointeractvoluntarily,recognizepeople,orprocess information6(Fig.1).
(d) Memory----itistheacquisition, development, conserva-tion,and retrieval of information. They areclassified accordingtotheduration,function,andcontent.7
(e) Declarativeor explicit memory----refersto information voluntarilyorspontaneouslyredeemed.
(f) Non-declarativeimplicitmemory----referstoinformation thatisnotvoluntarilyorspontaneouslyredeemed,able togeneratebehavioralchanges.8
(g) Amnesia----deficitintheformationorretrievalof mem-ories.Anestheticsmayaffectbothexplicitandimplicit
memory,butexplicitmemoryappearstobemore
sus-ceptibletodrug-inducedamnesia.9
Clinical
monitoring
of
anesthetic
depth
Somephysiological parametersareusedtomeasure
anes-thetic depth and guide the anesthetic choice and dose
titration. Blood pressure, heart rate, breathing pattern
changes,somatic and skeletal motor activities, sweating,
Deep sleep
Light sleep
General anesthesia
Coma
Somnambulism vegetative state convulsion
Level of consciousness (wakefulness)
Content of consciousness (
awareness
)
REM sleep
Drowsiness Conscious wakefulness
Figure1 Componentsofconsciousness:levelandcontentof consciousness.
lacrimation,pupildiameter,andvasomotorskinreflexesare used.10 However,dependingonpatient’sclinical condition
andondrugsused,theseparametersmayhavepoor
repre-sentationinassessinganestheticdepth.11
Tachycardia, hypertension, sweating, and lacrimation
are usually considered inadequate analgesia signs.
How-ever, sympatheticstimulationisnotalwaysaresultofthe painful stimuli perception. There are situations in which theparasympatheticcanbepredominantlystimulated,such asintheautonomicresponseduetonociceptivestimuliin theesophagus.Inthiscase,vagalfibersarepredominantly involved,triggeringaslowheartrate.10
Thepresenceofmovementinresponsetopainful
stim-ulihasbeenoneofthemethodsforassessingthepotencyof anestheticagents.Althoughthemotorresponseismediated byspinalreflexes,itspresenceisanimportantsignof inad-equateanesthesia,whichmakesthepatientsusceptibleto theriskofintraoperativeawakeningandawareness.10
Duringsurgeryundergeneralanesthesia,itisthemotor responsethatmakesitpossibletoknowwhetherthepatient
is abletovoluntarilymeet the commandsandrespondto
painful stimuli. When a neuromuscular blocking agent is
used, it prevents the motor response tovoluntarily
com-plywithcommands,orthemotorreflexresponsetopainful stimuli.
TheuseofneuromuscularblockerisrelatedtoAIA,which rarelyoccurswhenitisnotused.12
Topreservemotorresponses ofsurgical and
pharmaco-logicallyparalyzedpatients,theisolatedforearmtechnique (IFT)isastandardalternative.Itconsistsoftheisolationof aforearmwithapneumaticcuffinflatedbeforethe
intra-venous neuromuscular blocker injection, preventing drug
actioninthetemporarilyischemiclimb.12
TheoccurrenceofmotorresponsewithIFTisratedinfive levels:
Level0:Noresponseorspontaneousmovement.
Level1:Randommovementsunrelatedtoanystimulation.
Level2:Movementsinresponsetotactilestimuli,
includ-ingpainfulmovements(2a: movementnotlocalized,2b:
Level3:Movementindirectresponsetoverbalcommand.
Level 4:Movement in response toquestions or response
options.
Level5:Spontaneousandpurposefulmovements,showing
thepatient’sintentiontocommunicate.
Althoughthemostfrequentlyfoundresponselevelsare 0and 3,it is observedthat evenifAIAdoes not occurin
level 3, which was demonstrated in a study by Kerssens
etal.,13 where hemodynamic parameterswerenot
corre-latedwiththepresenceorabsenceofresponse,buttheEEG
parameterssuchasBISandSEF95%, whichshowedbetter
integrationbetweentheirvaluesand theclinical observa-tionbytheIFT.13
Electrical
monitoring
of
anesthetic
depth
Raw electroencephalogram (EEG) has characteristic
fre-quencybands,classifiedaccordingtofluctuationbandsas:
Gamma,Beta,Alpha,Theta,DeltaandSlow(Fig.2).14,15
When assessed without processing, they hamper the
analysisofintraoperativeparametersrelatedtoanesthetic
depth. With increased anesthetic depth, high amplitude
electrical activityis observedat lowfrequencies andmay havesurgesuppressionornoactivity(isoelectrical)patterns withhigherdosesofanesthetics(Fig.3).16
Thepatternofelectricalactivityusuallyshows frequen-ciesupto70Hzandamplitudes of±50V.Thisactivityis
superimposedonelectromyography, which hasamplitudes
andsimilarfrequencies butwithgreater representationin
valuesgreaterthan50Hz.However,equipmentsdeveloped
Gamma 25 to 40 Hz
Beta 12 to 25 Hz
Alpha 8 to 12 Hz
Theta 4 to 8 Hz
Delta 1 to 4 Hz
Slow <1 Hz
Figure2 Frequencybands.
Vegetative state, coma
Burst suppression (coma)
Isoelectrical (coma, brain death)
Figure 3 Deep anesthesia standards (isoelectrical orburst suppression).
Raw signal EE/EMG
Digitalization
Filter artifacts
Detection suppression
BSR & QUAZI Beta ratio
BIS Fast fourier
transform Bispectrum
Synchslow
Figure4 SubparametersgeneratingBIS.
to assess anesthetic depth show, independently, indexes
related to electromyography, evaluated in different
fre-quency bands (e.g., BIS: 70---110Hz and CSM: 75---85Hz). Eachoftheanestheticdepthevaluationequipmenthasits ownalgorithmwithseveralwindowsandbandsofdifferent analyses.17---19
BISVista® (AspectMedicalSystems,Newton,MA)
Forthecalculationoftheindicesrelatedtoequipment, fre-quenciesupto47Hz(nervoussystemandelectromyography) and70---110Hzareusedforelectromyography(EMG),where thesignalispickedupat2-swindows(epochs).Theindices are:
(a)Bilateralbispectral
BIS number is obtained from the weighted analysis of 4
subparameters:burstsuppressionratio,Quazisuppression, betarelativepower,andfast/slowsynchronization(Fig.4), whereamultivariatestatisticalmodelisappliedusinga non-linearfunction.Thedelaytimeis7.5sandtherefreshrate is1s.19
(b)Suppressionrate
Burstsuppressionisdefinedasintervalsgreaterthan0.5s, inwhich the EEGvoltage is below ±5Vin the last60s. Thus,normalsuppressionrateisequaltozero.14,19
(c)Electromyographicpower
This variable is calculated as the sum of all RMS (root
mean square) in the range of 70---110Hz, normalized to
0.01VRMSand expressed in decibels (dB). Forexample,
Figure5 Electromyography(EMG)inred.
(d)Asymmetry
It represents power variation between the right and left
sides of the brain, with a white spectral signalizing the higherpowerside.Inadults,variationsupto20%are con-siderednormal19(Fig.6).
(e)Spectraledgefrequency95%(SEF95%)
SEF95%isthefrequencybelowwhich95%ofthepowerisin therangeupto30Hz.However,spectralanalysis (spectro-gram)hasshowntobeofgreatimportanceforitsabilityto highlight the alpha-hypersyncronization (thalamocortical) andslowfluctuation(corticocortical)(Fig.7), characteris-ticsofadequatedepthofanesthesiainadults.20
Characteristicsofmonitoringequipmentavailable
inBrazil
The raw signal of electrical activity is picked up by sur-faceelectrodes(non-invasive),adaptedaccordingtopoints definedinneurologybythe system10/10 withreferential montages(Fig.8).15Table1showsthemainfeaturesofeach
equipment.18,19,21,22
Description
of
the
evidence
collection
method
The search strategy used for this recommendation was
by research in OvidMedline, Ovid Embase, and Cochrane
Library:{CochraneDatabaseofSystematicReviews(CDSR); CochraneCentral Registerof Controlled Trials(CENTRAL); Databaseof Abstracts of Reviews of Effects(DARE)}. The
references were crossed with the collected material for
identification of itemswithbetter methodologicaldesign, followedbycriticalevaluationofitscontentsand classifica-tionaccordingtothestrengthoftheevidence.
ThesearchesweremadebetweenJune andSeptember
2015.Theclinicalmonitoringsurveybeganinyear1990.For
BIS, Entropy, PSA 4000 (Patient State Analyzer), and CSM
(CerebralStateMonitor), thesurveyusedwas from2000.
The review waslimitedtoprospectivestudies, preferably systematicreviewswithrelevancetothetopicdiscussed.
The descriptors used in the search were: monitoring
intraoperative; and/or consciousness monitors/ and or sedation monitor/ and or sedation measurement/and or anesthesia,general/andoranesthesia,intravenous/andor anesthetics,inhalation/andorperioperativeperiod/and orperioperativeevaluation/andorsignalprocessing/and orcomputer-assisted/andorintraoperativecomplications/ perioperative care/ and or monitoring, physiologic/ and or electroencephalography/and ormentalrecall/ andor wakefulness/ and or consciousness/ and or perception/ intraoperativeawareness/orawareness/andordeep seda-tion/andorconscioussedation/andordepthofanesthesia monitor/andorpostoperativeperiod/andorEEGorEMG/ andorBIS/andorEntropy/andorPSA4000/CSM.
Thequalityofevidenceandstrengthofrecommendation
adopted for these consensus decisions was from GRADE
(Grading of Recommendations, Assessment, Development
andEvaluation),accordingtothefollowingdescriptions:
Qualityofevidence:
A----High: Level of evidence from well-planned and
con-ducted randomized clinical trials, with parallel groups, adequatecontrols,adequatedataanalysis,andconsistent findings,targetingtheclinicaloutcomeofinteresttothe physicianandthepatient.
B----Moderate: Evidence from randomized controlled
tri-als with important problems in conducting, inconsistent
results,assessmentofasurrogateendpointratherthanan outcomeofinteresttothephysicianandpatient, assess-mentimprecision,andpublicationbiases.
C----Low: Results from cohort studies and case control,
highlysusceptibletobias.
08:38 Esquerda SEF 17
22 Mai 2008 08:56:50 Ad8P
SEF 16 Direita
ASYM
08:43
08:48
08:53
08:58
09:03
09:08
30 Hz 20 Hz 10 Hz 100% 20% 100% 10 Hz 20 Hz 30 Hz
16:08
16:13
16:18
16:23
16:28
16:33
16:38
30 Hz 20 Hz 10 Hz 100% 20% 100% 10 Hz 20 Hz 30 Hz SEF 18
Left ASYM SEF 16 Right
07 Jul 2015 16:38:27 dj9v
Figure7 SEF95%bilateralandbilateralspectrogramwithalphahypersynchronization.
Figure8 Positioningofthesensorsaccordingtothemanufacturer:A,BIS;B,Entropy;C,CSM;andD,SEDLine.
Table1 Mainparametersofeachequipment.
Equipment Anesthesia/limits TS/limits EMG/limits Asymmetry SEF95% Spectrogram Delaytime
BISbilateralview 40---60 ±5V 70---110Hz Yes Yes Yes 7.5s
SEDLine-PSIbilateral 25---50 NA NA No Yes Yes 6.4s
Entropyresponse 40---60 NA NA No No No Variable
CSM 40---60 ±3.5V 75---85Hz No No No 15s
D----Verylow:Resultsfromuncontrolledobservational stud-iesandunsystematicclinicalobservations.
Strengthofrecommendation:
1----Strong:Theadvantagesclearlyoutweighthe disadvan-tages;orelse,thedisadvantagesoutweightheadvantages. 2----Weak: There is uncertainty between advantages and disadvantage.
Strategies
and
recommendations
Becausetheaimofthisstudywastoevaluatetheimpactof monitoringthebrainelectricalactivityingeneralanesthesia ondifferentoutcomes,weconsideredthefollowingtopics:
Anestheticconsumption
Excessiveadministrationofanestheticagentsisoftenused unnecessarily.Thiseffectoccursbecausethedepthof anes-thesiais usuallyguidedbysomaticand autonomicclinical signs.However,these signsdonothavereliable measures toensureunconsciousness.23Somestudieshaveshownthat
propermonitoringofanestheticdepthcouldreduce exces-siveadministrationofanestheticagents,reducingrecovery
timefromanesthesia,nauseaandvomiting,headache,and
cognitivedysfunction,especiallyintheelderly.23,24
The monitoring of anesthetic agent measurements,
especially of inhaled gases, has become routine because
of the units incorporated into multiparameter monitors.
Studiesusing thequantification ofexpired gas concentra-tionsshowedsignificantreductioninthetotalconsumption
of agents, compared to clinical monitoring.25,26
How-ever, it does not guarantee the absenceof consciousness
and, when compared withthe assessment instruments of
brainelectrical activity,it results in increasedanesthetic consumption.27---29
Thereisacloserelationshipbetweeninhaledanesthetic agent titrationand electrical activity monitoring.25,26,30,31
Thus, consciousness monitors began to be used to guide
anestheticadministration.
The studieschosen for thisevaluationhave high scien-tificconsistency;GradesAandB,wereselectedfromamong thosewithlowevidence ofbias, despitethe impossibility of blindness by the professional usingthe monitor in the study.The inclusioncriteriaincluded comparisonof anes-theticdepth monitoring,such asBIS,Entropia, PSA4000, andCSM,comparedwithclinicalsignsorfractionalexpired anestheticgases.Agentsusedinthestudieswerepropofol, desflurane,sevofluraneorisoflurane.25,27---61
The studies showed that these monitors, especially
BIS,when properlyused, provide reduction of anesthetic
consumption.38,39,51,55,62---66
Recent meta-analysis by Cochrane23 showed that in
10 studies with intravenous anesthesia involving 672
par-ticipants, there was a significant reduction in propofol
consumptionwhentheanestheticdepthwasguidedbythe
BIS.The meanreductionwas1.32mgkgh−1 (95%CI −1.91 to−0.73).Thesamemeta-analysisshowedthatin14 stud-iesofbalancedanesthesia,involving985participants,there wasasignificantreductioninanestheticconsumptionwith
anaveragedecreaseof0.65MAC(95%CI−1.01to−0.28). Regardinganalgesicconsumption,thestudiesevaluated fen-tanyl, remifentanil,andsufentanil consumptions,showing reducedconsumption.OnlyinthestudybyHacheroetal.,40
asignificantincreasewasfoundintheuseoffentanylwith BIScontrol.Thecombiningresultsshowednosignificant dif-ferenceintheuseofnarcotics.
Recommendation
Theuseofdevicestomonitoranestheticdepth,suchasBIS,
Entropia, PSA 4000, and CSM, is associated with reduced
inhaledandintravenousanestheticconsumptions,aswellas
reducedanestheticrecoverytime,comparedtothemethod
ofclinicalsignsandsymptomsmonitoring(1Aand1B).
Intraoperativeawakening
Studies have shown variability in the incidence of
intra-operative awakeningduetodifferentsurveymethods and
differences in the studied population. Some studies with
populationsconsideredtobeathigherriskreportedan
intra-operative awakening incidence of 1:100, especially when
repeated questionnairesare used.67 Othersreported very
lowincidenceof1:15,000whenthereportisdone sponta-neouslybythepatient,asintheprojectNAP5.68
Whileitseemsreasonable thatthemonitoringof brain electrical activity can prevent intraoperative awakening, theavailableevidenceshowsresultsthatdependonthe pop-ulation,ontheanesthetictechnique,andontheevaluated monitoring.
Itisworthnotingthepopulationsthatareatincreased riskofintraoperativeawakening.Therearethreesituations commonly associatedwiththisevent:(i)thepatientdoes not tolerate adequate doses of anesthetic (e.g., critical
patients); (ii) there is inadequate anesthesia masking
signals(useofneuromuscularblockers);(iii)thenatureof theoperationorthepatient’sconditionrequiringdifferent doses.67,69
OtherriskfactorsforintraoperativewakeincludetheASA status (indicating patients with more comorbidities),70,71
useof totalintravenousanesthesia, historyof depression, absenceofpremedication,previoushistoryofawakening,72
andemergencyoperation.71
SomestudieshaveinvestigatedtheimpactofusingBISin theincidence ofintraoperative awakening. Mylesetal.,73
showed a significant reductionof the event in ahigh-risk population(absoluteriskreductionof0.73%)withBIS, com-paredtostandardcare.Itisnoteworthythattheincidence ofmemorywashighinthecontrolgroupinthisstudy:0.89%. However,it hasnot been confirmed in laterstudies, such as the B-Unaware30 and Bag-Recall.31 These studies
com-paredtheincidenceofintraoperativeawakeninginhigh-risk patientsrandomizedintotwogroups:theuseofBISbetween
40 and60 versus MACmaintenance between 0.7and 1.3.
Therewasnodifferencebetweenthegroups;however,the
studypowerwascalculatedbasedonanincidenceof1%and 0.5%,respectively.Zhangetal.74conductedasimilar
inves-tigationwithtotalintravenousanesthesia,showingthatthe incidence of explicit memorydecreased significantly with BISmonitoring(0.65---0.14%).
B-Unaware30wasthefirststudytoassesstheuse
surveyed 1941 patients and found an incidence of intra-operative awakeningof 0.21%(95%CI,0.08---0.53)without reducingtheeventusingBIS.
AsestimatedbythestudyBag-Recall,31itwouldbe
nec-essarytostudy3333high-risk patientsinordertoprevent oneepisodeofawarenessusingBIS.Theresultsofthe Bag-RecallstudydonotsupportthesuperiorityofBISprotocol overend-tidalanesthetic-agentconcentrationprotocolsto preventintraoperativeawakeningeveninhigh-riskpatients.
This studysought tocorrectsome flawsoftheB-Unaware
study, such as being multicenter, international, having a largersample,anddiscardinglow-riskcriteriasuchas fac-torsforinclusionofpatients.However,thestudyhadseveral limitationsthat maynotberuled out,suchasconsidering theresultsinpatientsreceivingpotentinhalationanesthetic agents,unabletoextrapolatethemtootheragents. Further-more,thestudyusedonlyoneofthecommerciallyavailable technologiesformonitoringawareness.
Mashour etal.25 evaluated21,601 patientsand didnot
demonstrate increased efficacy of using monitoring (BIS), comparedtotheuseofanestheticprotocolstoreducethe
incidenceof intraoperative awakeningwithexplicit
mem-ory (0.08 vs. 0.12%, p=0.48). However, post hoc analysis
has demonstratedthat the use of BIS maybe superior to
theabsenceofmonitoring toreduceintraoperative
awak-ening.These data are consistent withthosedescribed by
the Cochranesystematic review;75 however, therewasno
benefitinanesthesiarecovery.
According tothe analysisandreview of the literature,
we observed that the recommendations of the American
Society of Anesthesiologists Task Force on intraoperative awakening76 corroboratethecurrentstudies.
Recommendation
Topreventintraoperativeawakening,theuseofbrain elec-trical activity monitors is suggested for high-risk patients underbalancedgeneralanesthesia(2B).Forpatientsunder totalintravenousanesthesia,asitisariskfactorfor intra-operative awakening, the use of brain electrical activity
monitoringishighlyrecommended(1A).
Morbidityandmortality
Ifononehand themaintenance ofinadequateanesthesia
is associated with intraoperative awakening and its seri-ousconsequences,ontheotherhand,ageneralanesthesia deeperthannecessarytokeepthepatientunconscioushas beenconsideredamarkerofseverity,especiallyinelderly andcritically illpatients.However,studies evaluatingthe
association between anesthetic depth and mortality are
secondaryanalyses ofoutcomesdesignedfor another
pur-pose,oraremultivariateanalysisofinstitutionaldatabases that,despitehavingalargeobservationalsample,collidein theweaknessofthemultivariatemodelconclusions,which
are legitimate proponents of hypotheses, but lack robust
prospectivestudiesforcausalconfirmationofthefindings. ThestudybyMonketal.77identifiedtheBIScumulative
time<45 (relative risk=1.244h−1; p=0.0121) as an inde-pendentpredictorofmortalityinuptooneyearafterthe operation.However,itwasnotconfirmedinanotherstudy withsimilardesignandpresenceofcancerasacovariate.78
Patientswithoutcancershowednoincreasedmortality,even withconsiderablylowcumulativelevelsofBIS.
Secondary analysis of the B-Aware study79 evaluating
intraoperativeawakeningshowednodifferenceinmortality betweenthegroupundergoinganesthesiaguidedbyBISand thestandardcaregroup.However,intheanalysisofthe sub-groupmonitoredwithBIS,therewashighermortalitywithin fouryearsin the group withdeepanesthesia (BIS<40 for morethan5min).Asimilarresultwasfoundinthesecondary analysisofpatientsundergoingcardiacsurgeryinthestudy B-Unware.80BISlevels<45wereassociatedwithhigher
mor-tality,alongwithotherseveritycriteria,suchastransfusion, ICUstay,anduseoftranexamicacid.Theauthors hypothe-sizethatlowBISvaluesareanepiphenomenon,thatis,they arenotresponsiblefortheprimaryoutcome,asinthe anal-ysisofpatientsundergoingnon-cardiacsurgeryinthesame study;thisassociationcouldnotberelated.81
Sessler et al.82 found that the combination of
intra-operative variables, with hypotension, low levels of BIS, andlowlevelsofinhaledanestheticsconcentration(Triple Low),isassociatedwithmorefragile patients,susceptible tocomplications.This study linked theassociation of low MAP(<75mmHg),lowMAC(<0.8),andlowlevelsofBIS(<45) withincreased30-daymortality.Thegeneratedhypothesis wasthatthesecombinedvariablesaremarkersofaprofile ofpatients‘‘sensitive’’toperioperativestressratherthan potentialtherapeutictargetsthatmaybeinvolvedin redu-cingadverseevents.Kertaietal.,83usingthe‘‘TripleLow’’
criteria,found thatthese variableswerenot independent predictorswhenclinicalandsurgicalvariablesareincluded inthestatisticalmodel.
Evidenceof mortalityand lowlevels ofBIS association or‘‘Triplelow’’areconflicting.Nevertheless,theyindicate thatsusceptiblepatientsdeservespecialcare,withthe pos-sibilityofoptimizationofresultsintheshort,mediumand long run. Willinghamet al.,84 in a retrospective
observa-tionalstudy including 13,198 patients from three clinical
trials: B-Unaware, BAG-RECALL and Michigan Awareness
ControlStudy,showedthattherisk ofmortalityat30and 90dayspostoperativelywasincreasedbyapproximately10%
for every 15 cumulative minutes in the triple low state,
suggestingthatthisisnotanepiphenomenon.Randomized, prospective,controlledstudiesinprogress,suchasthe Bal-ancedtrial(www.anzctr.org.au,ACTRN12612000632897),85
comparingtheeffectsofdifferentlevelsofanestheticdepth inmortalityuptooneyear,probablywillclarify the influ-enceofthedepthofanesthesiaandpostoperativemortality.
Recommendation
ElectricalnervousactivityevaluatedmostlybytheBIS
(dis-regardingother possible components, suchas suppression
rate,spectrogram or both), alone or in combination with
othervariablessuchasMAPandCAMpercentage,hasaweak associationwithmortality(2B).
Postoperativedelirium(POD)andpostoperative
cognitivedysfunction(POCD)
Intheelderlypopulation,cognitivechangessuchasdelirium
andPOCDafter anesthetic-surgical procedureshave older
PODisanacuteonsetsyndromecharacterizedbychanges inconsciousnessandfloatingvariationinmemory,attention, cognitive,andperceptualdisorders.87
COPDisasubtledisorderofthoughtprocessesthatcan influenceisolatedareasof cognition,suchasverbal mem-ory,visualmemory,languagecomprehension,visual-spatial abstraction,attentionorconcentration.88
PODisthemostimportantfactorforCOPDinhospitalized geriatricpatients.87
The brain ofan elderly personrequires lower dosesof
anestheticagentscomparedtothatofayoungpersonand
is more likely topresent burst suppression in the EEG.89
Brainmonitors,suchastheBIS,allowadequateanesthetic depth,dosetitration,andminimizestheresidualeffectson cognition.76,90---94
There is correlation between surface anesthesia and
post-traumatic stress syndrome and between deep
anes-thesiaandcognitivedysfunction.94 Randomizedcontrolled
trials show reduced incidence of POD when patients are
monitoredwithBIS.90---93
Chanet al., ina randomized studywith patients aged
60years or more, comparingpatients monitored withBIS
or routinecare, found that the BIS group (40-60)showed
reducedriskofdevelopingdeliriumintheimmediate
post-operative period and POCD in the evaluation at three
months.91
Recommendation
Monitoring the depth of anesthesia with BIS monitor
facilitatesanesthetic titration, decreases brain exposure, especially in the elderly, to high doses of the anesthetic
agents, and thus can contribute to reduce POD (1A) and
POCD(2Aand2B).
Conflicts
of
interest
TheauthorsareconsultantsMedtronic.
References
1.Aceto P, Perilli V, Lai C, et al. Update on post-traumatic stresssyndromeafteranesthesia.EurRevMedPharmacolSci. 2013;17:1730---7.
2.Monk TG,Saini V,WeldonBC,et al.Anestheticmanagement andone-yearmortalityafternoncardiacsurgery.AnesthAnalg. 2005;100:4---10.
3.Mashour GA, Orser BA, Avidan MS. Intraoperative aware-ness from neurobiology to clinical practice. Anesthesiology. 2011;114:1218---33.
4.PurdonPL,PierceET,MukamelEA,etal.Electroencephalogram signaturesoflossandrecoveryofconsciousnessfrompropofol. PNAS.2013;110:E1142---51.
5.Koch C, Mormann F. The neurobiology of consciousness. In: MashourGA,editor.Consciousness,awareness,andanesthesia. 1sted.Cambridge:CambridgeUniversityPress;2010.p.24---46.
6.LaureysS.Theneuralcorrelateof(un)awareness:lessonsfrom thevegetativestate.TrendsCognSci.2005;9:556---9.
7.IzquierdoI.Memória.2nded.SãoPaulo:ArtmedEditora;2011. p.11.
8.KerssensC,AlkireM.Memoryformationduringgeneral anes-thesia.In:MashourGA,editor.Consciousness,awareness,and anesthesia.1sted.NewYork:CambridgeUniversityPress;2010. p.47---73.
9.Moore J, Kelz M. Brain anatomy of relevance to the anes-thesiologist.In:MashourGA,LydicR,editors.Neuroscientific foundationofanesthesiology.1sted.NewYork:Oxford Univer-sityPress;2011.p.7---16.
10.GuinardB.Monitoringanalgesia.BestPractResClin Anaesthe-siol.2006;20:161---80.
11.Nunes RR. Componentes da atividade anestésica-uma nova visão.RevBrasAnestesiol.2003;53:145---9.
12.Pandit JJ, Russell IF, Wang M. Interpretations of response usingtheisolated forearmtechniqueingeneral anaesthesia: adebate.BrJAnaesth.2015;115Suppl.1:i32---45.
13.Kerssens C, Klein J, Bonke B. Awareness: monitoring versus rememberingwhathappened.Anesthesiology.2003;99:570---5.
14.RampillIJ. Aprimerfor EEGsignalprocessinginanesthesia. Anesthesiology.1998;89:980---1002.
15.MontenegroMA,CendesF,GuerreiroMM,etal.EEGnaprática clínica.2nded.RiodeJaneiro:Revinter;2012.
16.Brown EM, Lydic R, Schiff ND. General anestesia, sleep and coma.NEnglJMed.2010;363:2638---50.
17.ZouridakisG,PapanicolaouAC.Aconciseguideto intraopera-tivemonitoring.BocaRaton:CRCPress;2001.
18.JensenEW,LitvanH,RevueltaM,etal.Cerebralstateindex duringpropofolanesthesia.Anesthesiology.2006;105:28---36.
19.NunesRR, Chaves IMM, Alencar JCG, et al. Bispectral index andotherprocessedparametersofelectroencephalogram:an update.RevBrasAnestesiol.2012;62:105---17.
20.PurdonPL,PierceET,MukamelEA,etal.Electroencephalogram signaturesoflossandrecoveryofconsciousnessfrompropofol. PNAS.2013:E1142---51.
21.DroverDR,LemmensHJ,PierceET,etal.Patientstateindex. Tritationofdeliveryandrecoveryfrompropofol,alfentaniland nitrousoxideanestesia.Anesthesiology.2002;97:82---9.
22.Nunes RR, Almeida MP, Sleigh JW. Spectral entropy: a new method for anesthetic adequacy. Rev Bras Anestesiol. 2004;54:404---22.
23.Punjasawadwong Y, Phongchiewboon A, Boonjeungmonkol N. Bispectralindexforimprovinganaestheticdeliveryand post-operative recovery (Review). Cochrane Database Syst Rev. 2014;6:CD003843.
24.HudsonAE,HemmingsHC.Areanaestheticstoxictothebrain? BrJAnaesth.2011;107:30---7.
25.Mashour GA, Shanks A, Tremper KK, et al. Prevention of intraoperativeawarenesswithexplicitrecallinanunselected surgicalpopulation:a randomized comparativeeffectiveness trial.Anesthesiology.2012;117:717---25.
26.AvidanMS,MashourGA.Preventionofintraoperativeawareness withexplicitrecall:makingsenseoftheevidence. Anesthesiol-ogy.2013;118:449---56.
27.Ahmad S, Yilmaz M, Marcus RJ, et al. Impact of bispec-tralindexmonitoringonfasttrackingofgynecologicpatients undergoing laparoscopic surgery. Anesthesiology. 2003;98: 849---52.
28.BasarH, Ozcan S, Buyukkocak U, et al. Effect of bispectral indexmonitoringonsevofluraneconsumption.EurJ Anaesthe-siol.2003;20:396---400.
29.RecartA,GasanovaI,WhitePF,etal.Theeffectofcerebral monitoring on recovery after general anesthesia:a compar-ison of the auditory evoked potential and bispectral index deviceswithstandardclinicalpractice.AnesthAnal.2003;97: 1667---74.
30.AvidanMS,ZhangL,BurnsideBA,etal.Anesthesiaawareness andthebispectralindex.NEnglJMed.2008;358:1097---108.
32.AimeI, Verroust N, Masson-Lefoll C,et al. Does monitoring bispectralindex or spectralentropy reducesevoflurane use? AnesthAnalg.2006;103:1469---77.
33.AnezC,PapaceitJ,SalaJM,etal.Theeffectofencephalogram bispectralindexmonitoringduringtotalintravenousanesthesia withpropofolinoutpatientsurgery.RevEspAnestesiolReanim. 2001;48:264---9.
34.AssareH,AndersonRE,JakobssonJ.Sevofluranerequirements duringambulatorysurgery:aclinicalstudyofbispectralindex andauditoryevokedpotentialguidedanaesthesia.AmbulSurg. 2002;9:207---11.
35.BoztugN,Bigat Z,AkyuzM,et al.Does usingthebispectral index(BIS)duringcraniotomyaffectthequalityofrecovery?J NeurosurgAnesthesiol.2006;18:1---4.
36.BruhnJ,KreuerS,BischoffP,etal.BispectralindexandA-line AAIindexasguidancefordesflurane-remifentanilanaesthesia comparedwithastandardpracticegroup:amulticentrestudy. BrJAnaesth.2005;94:63---9.
37.ChiuCL,Ong G, Majid AA. Impact ofbispectral index mon-itoring on propofol administration in patients undergoing cardiopulmonary bypass. Anaesth Intensive Care. 2007;35: 342---7.
38.EllerkmannRK,SoehleM,KreuerS.TheEntropyModule® and BispectralIndex®asguidanceforpropofol-remifentanil anaes-thesiaincombinationwithregionalanaesthesiacomparedwith a standard clinical practice group. Anaesth Intensive Care. 2010;38:159---66.
39.GanTJ,GlassPS,WindsorA,etal.BispectralIndexmonitoring allowsfasteremergenceandimprovedrecoveryfrompropofol, alfentanilandnitrousoxideanesthesia.BISUtilityStudyGroup. Anesthesiology.1997;87:808---15.
40.HacheroA,AlamoF,CabaF,etal.-Influenceofbispectralindex monitoringonfentanylrequirementsduringtotalintravenous anesthesiaformajorgynecologicalsurgery.RevEspAnestesiol Reanim.2001;48:364---9.
41.Ibraheim O, Alshaer A, Mazen K, et al. Effect of bispec-tral index (BIS) monitoring on postoperative recovery and sevofluraneconsumptionamongmorbidlyobesepatients under-goinglaparoscopicgastricbanding.MiddleEastJAnesthesiol. 2008;19:819---30.
42.KamalNM,OmarSH,RadwanKG,etal.Bispectralindex moni-toringtailorsclinicalanestheticdeliveryandreducesanesthetic drugconsumption.JMedSci.2009;9:10---6.
43.Kreuer S, Biedler A, Larsen R, et al. Narcotrend moni-toring allows faster emergence and a reduction of drug consumptioninpropofol-remifentanilanesthesia. Anesthesiol-ogy.2003;99:34---41.
44.KreuerS,BruhnJ,StrackeC,etal. Narcotrendorbispectral indexmonitoringduringdesflurane-remifentanilanesthesia:a comparisonwithastandardpracticeprotocol.Anesth Analg. 2005;101:427---34.
45.LeslieK, MylesPS,ForbesA,et al.Recoveryfrombispectral index-guidedanaesthesiainalargerandomizedcontrolledtrial ofpatientsathighriskofawareness.AnaesthIntensiveCare. 2005;33:443---51.
46.Luginbuhl M, Wuthrich S, Petersen-Felix S, et al. Different benefitofbispectralindex(BIS)indesfluraneandpropofol anes-thesia.ActaAnaesthesiolScand.2003;47:165---73.
47.MasudaT,Yamada H,TakadaK, etal. Bispectralindex mon-itoring is useful to reduce totalamount of propofol and to obtainimmediate recovery afterpropofolanesthesia. Masui. 2002;51:394---9.
48.MorimotoY, Oka S,Mii M,etal. Efficacyofbispectralindex monitoringinimprovinganestheticmanagement,economics, anduseoftheoperatingtheater.Masui.2002;51:862---8.
49.MuralidharK,BanakalS,MurthyK,etal.Bispectralindex-guided anaesthesiaforoff-pumpcoronaryarterybypassgrafting.Ann CardiacAnaesthesia.2008;11:105---10.
50.MylesPS,LeslieK,McNeilJ,etal.Bispectralindexmonitoringto preventawarenessduringanaesthesia:theB-Awarerandomised controlledtrial.Lancet.2004;363:1757---63.
51.NelskylaKA,Yli-HankalaAM,PuroPH,etal.Sevoflurane titra-tion using bispectral indexdecreases postoperativevomiting inphase IIrecovery afterambulatorysurgery. AnesthAnalg. 2001;93:1165---9.
52.PaventiS,SantevecchiA,MettaE,etal.Bispectralindex mon-itoringinsevofluraneandremifentanilanesthesia.Analysisof drugsmanagementandimmediaterecovery.Minerva Anesthe-siol.2001;67:435---9.
53.Puri GD, Murthy SS. Bispectral index monitoring in patients undergoingcardiacsurgeryundercardiopulmonarybypass.Eur JAnaesthesiol.2003;20:451---6.
54.Samarkandi AH, Abdel-Meguid ME, Abdullah KM, et al. Bis-pectralindex monitoringandtitrationofanaestheticsduring off-pump coronary artery bypass surgery. Egypt J Anaesth. 2004;20:357---61.
55.SongD,JoshiGP,WhitePF.Titrationofvolatileanestheticsusing bispectralindexfacilitatesrecoveryafterambulatory anesthe-sia.Anesthesiology.1997;87:842---8.
56.Struys MM, DeSmet T, Versichelen LF, et al. Comparison of closed-loopcontrolledadministrationofpropofolusing Bispec-tralIndexasthecontrolledvariableversus‘‘standardpractice’’ controlledadministration.Anesthesiology.2001;1:6---17.
57.TufanoR,PalombaR,LambiaseG,etal.Theutilityof bispec-tralindexmonitoringingeneralanesthesia.MinervaAnestesiol. 2000;66:389---93.
58.WhitePF,MaH,TangJ,etal.Doestheuseof electroencephalo-graphic bispectral index or auditory evoked potential index monitoringfacilitaterecoveryafterdesfluraneanesthesiainthe ambulatorysetting?Anesthesiology.2004;100:811---7.
59.WongJ,SongD,BlanshardH,etal.Titrationofisofluraneusing BISindeximprovesearlyrecoveryofelderlypatientsundergoing orthopedicsurgeries.CanJAnaesth.2002;49:13---8.
60.ZhangC,XuL,MaYQ,etal.Bispectralindexmonitoringprevent awarenessduringtotalintravenousanesthesia:aprospective, randomized,double-blinded,multi-centercontrolledtrial.Chin MedJ.2011;124:3664---9.
61.ZoharE,LubanI,WhitePF,etal.Bispectralindexmonitoring doesnotimproveearlyrecoveryofgeriatricoutpatients under-goingbriefsurgicalprocedures.CanJAnaesth.2006;53:20---5.
62.BannisterCF,BrosiusKK,SiglJC,etal.Theeffectofbispectral index monitoringonanesthetic useand recovery inchildren anesthetizedwithsevofluraneinnitrousoxide.AnesthAnalg. 2001;92:877---81.
63.Bhardwaj N, YaddanapudiS. A randomizedtrial of propofol consumptionand recovery profilewithBIS-guided anesthesia comparedtostandardpracticeinchildren.PaediatrAnaesth. 2010;20:160---7.
64.Chan MTV,ChengB, GinT,etal. Cognitivedysfunctionafter anesthesia:a randomizedcontrolledtrial.JNeurosurg Anes-thesiol.2010;22:408---9.
65.Kerssens C, Gaither JR, Sebel PS. Preserved memory func-tionduringbispectralindex-guidedanesthesiawithsevoflurane for major orthopedic surgery. Anesthesiology. 2009;111: 518---24.
66.MessiehaZS,AnandaRC,HoffmanWE,etal.BispectralIndex System(BIS)monitoringreducestimetodischargeinchildren requiringintramuscularsedationandgeneralanesthesiafor out-patientdentalrehabilitation.PediatrDent.2004;26:256---60.
67.LeslieK,DavidsonAJ.Awarenessduringanesthesia:aproblem withoutsolutions?MinervaAnestesiol.2010;76:624---8.
anaes-thesia:summaryofmainfindingsandriskfactors.BrJAnaesth. 2014;113:549---59.
69.Ghoneim MM, Block RI, Haffarnan M, et al. Awareness during anaesthesia: risk factors, causes and sequelae: a review of reported cases in the literature. Anesth Analg. 2009;108:527---35.
70.Sebel PS, BowdleTA, Ghoneim MM, et al. The incidence of awareness during anaesthesia: a multicenter United States study.AnesthAnalg.2004;99:833---9.
71.ErrandoCL,SiglJC,RoblesM,etal.Awarenesswithrecallduring generalanaesthesia:aprospectiveobservationalevaluationof 4001patients.BrJAnaesth.2008;101:178---85.
72.AranakeA,GradwohlS,Ben-AbdallahA,etal.Increasedriskof intraoperativeawarenessinpatientswithahistoryof aware-ness.Anesthesiology.2013;119:1275---83.
73.MylesPS,LeslieK,McNeilJ,etal.Bispectralindexmonitoringto preventawarenessduringanaesthesia:theB-Awarerandomised controlledtrial.Lancet.2004;363:1757---63.
74.ZhangC,LiangMA,Ya-qunMA,et al.Bispectralindex moni-toringpreventawarenessduringtotalintravenousanesthesia: aprospective,randomized,double-blinded,multi-center con-trolledtrial.ChinMedJ.2011;124:3664---9.
75.Punjasawadwong Y, Phongchiewboon A, Bunchungmongkol N. Bispectral index for improving anaesthetic delivery and postoperative recovery. Cochrane Database Syst Rev. 2014;6:CD003843.
76.Practice Advisory for Intraoperative Awareness and Brain Function Monitoring. A report by the American Society of AnesthesiologistsTaskForceonIntraoperativeAwareness. Anes-thesiology.2006;104:847---64.
77.MonkTG,SainiV,WeldonBC,SiglJC.Anestheticmanagement andone-yearmortalityafternoncardiacsurgery.AnesthAnalg. 2005;100:4---10.
78.Lindholm ML, Traff S, Granath F, et al. Mortality within 2 yearsaftersurgeryinrelationtolowintraoperativebispectral indexvaluesandpreexistingmalignantdisease.AnesthAnalg. 2009;108:508---12.
79.LeslieK,Myles PS,ForbesA, ChanMT.Theeffectof bispec-tralindexmonitoringonlong-termsurvivalintheB-awaretrial. AnesthAnalg.2010;110:816---22.
80.KertaiMD,PalN,PalancaBJ,etal.Associationof periopera-tiveriskfactorsandcumulativedurationoflowbispectralindex withintermediate-termmortalityaftercardiacsurgeryinthe B-UnawareTrial.Anesthesiology.2010;112:1116---27.
81.KertaiMD,PalancaBJ,PalN,etal.Bispectralindexmonitoring, durationofbispectralindexbelow45,patientriskfactors,and intermediate-termmortalityafternoncardiacsurgeryinthe B-UnawareTrial.Anesthesiology.2011;114:545---56.
82.Sessler DI,Sigl JC, Kelley SD, et al. Hospitalstay and mor-tality are increased in patients having a ‘‘triple low’’ of low bloodpressure,low bispectral index, and low minimum alveolarconcentrationofvolatileanesthesia.Anesthesiology. 2012;116:1195---203.
83.KertaiM,WhiteWD,GanTJ. Cumulativeduration of‘‘triple low’’stateoflow bloodpressure,lowbispectralindex, and low minimum alveolar concentration of volatile anesthesia is not associated with increased mortality. Anesthesiology. 2014;121:18---28.
84.Willingham MD, KarrenE,Shanks AM, et al. Concurrence of intraoperativehypotension,lowminimumalveolar concentra-tion,andlowbispectralindexisassociatedwithpostoperative death.Anesthesiology.2015;123:775---85.
85.ShortTG,LeslieJ,ChanMTV,etal.Rationaleanddesignofthe balancedanesthesiastudy:a prospectiverandomizedclinical trialoftwolevelsofanestheticdepthonpatientoutcomeafter majorsurgery.AnesthAnalg.2015;121:357---65.
86.NunesRR,Lopes CGD.Deliriumedistúrbio cognitivono pós-operatório. In: Pires OC, Albuquerque MAC, Fernandes CRF, etal.,editors.Educac¸ãoContinuadaemAnestesiologia, vol. 7.RiodeJaneiro:SociedadeBrasileiradeAnestesiologia(SBA); 2015.p.47---54.
87.Ahmed S, Laurent B, Sampson EL. Risk factors for inci-dent deliriumamong olderpeople inacute hospital medical units: a systematic review and meta-analysis. Age Ageing. 2014;43:326---33.
88.BrysonGL,WyandA.Evidence-basedclinicalupdate:general anesthesiaandtheriskofdeliriumandpostoperativecognitive dysfunction.CanJAnesth.2006;53:669---77.
89.Purdon PL, Pavone KJ, Akeju O, et al. The ageing brain: age-dependent changes in the electroencephalogram during propofol and sevoflurano generalanaesthesia. Br J Anaesth. 2015:i46---57.
90.SieberFE,ZakriyaKJ,BluteMR,etal.Sedationdepthduring spinalinelderlypatientsundergoinghipfracturerepair.Mayo ClinProc.2010;85:18---26.
91.Chan MT, Cheng BC, Lee TM, et al. CODA Trial Group. BIS-guidedanesthesiadecreasepostoperativedeliriumand cog-nitivedecline.JNeurosurgAnesthesiol.2013;25:33---42.
92.RadtkeFM, FranckM,Lendner J, et al.Monitoringdepth of anaesthesiainarandomizedtrialdecreasestherateof postop-erativedeliriumbutnotpostoperativecognitivedysfunction.Br JAnaesth.2013;110:i98---105.
93.WhitlockEL,TorresBA,NanLin,etal.Postoperativedelirium inasubstudyofcardiothoracic surgicalpatientsinthe BAG-RECALLclinicaltrial.AnesthAnalg.2014;118:809---17.