REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
Publicação Oficial da Sociedade Brasileira de Anestesiologiawww.sba.com.br
SCIENTIFIC
ARTICLE
The
relationship
between
preoperative
anxiety
levels
and
vasovagal
incidents
during
the
administration
of
spinal
anesthesia
Mürsel
Ekinci
a,∗,
Birzat
Emre
Gölboyu
a,
Onur
Dülgero˘
glu
b,
Murat
Aksun
c,
Pınar
Karaca
Baysal
a,
Erkan
Cem
C
¸elik
d,
Ays
¸e
Nur
Yeksan
eaKarsStateHospital,DepartmentofAnesthesiologyandReanimation,Kars,Turkey bKarsStateHospital,DepartmentofGeneralSurgery,Kars,Turkey
cKatipCelebiSchoolofMedicine,DepartmentofAnesthesiologyandReanimation, ˙Izmir,Turkey dPalandokenStateHospital,DepartmentofAnesthesiologyandReanimation,Erzurum,Turkey eKafkasUniversitySchoolofMedicine,DepartmentofAnesthesiologyandReanimation,Kars,Turkey
Received15January2016;accepted29July2016 Availableonline9September2016
KEYWORDS
Anxiety;
Spinalanesthesia; Syncope;
Vasovagal
Abstract
Background: Itwas aimedtoinvestigate therelationshipbetween preoperativeanxietyand vasovagalsymptomsobservedduringtheadministrationofspinalanesthesiainpatients under-goingsurgeryintheperianalandinguinalregions.
Methods:Thestudyincludedpatientswithplannedsurgeryforinguinalherniarepair,anal fis-sure,hemorrhoidandpilonidal sinusexcision.The studyincludedatotalof210patientsof ASAI---II,aged18---65years.Patientswereevaluatedinrespectofdemographiccharacteristics, smokingandalcoholconsumption,ASAgradeandeducationallevel.Correlationswere evalu-atedbetweenthenumberofattemptsatspinalanesthesiaandanesthesiahistorywithvasovagal symptomsandeducationallevel,gender,smokingandalcoholconsumptionandanesthesia his-torywithanxietyscores.Theinstant(transient)stateanxietyinventorypartoftheTransient State/TraitAnxiety Inventory(State Trait AnxietyInventory ---STAI) was used todetermine theanxiety levelsofthe participants.Clinical findings ofperipheral vasodilation, hypoten-sion,bradycardia andasystoleobservedduringtheadministrationofspinal anesthesiawere recorded.
Results:Vasovagal incidences during the administration of spinal anesthesia were seen to increase incasesofhighanxietyscore,malegender, andanabsenceofanesthesiahistory. Educationallevelandthenumberofspinalneedlepunctureswerenotfoundtohaveanyeffect onvasovagalincidents.
∗Correspondingauthor.
E-mail:[email protected](M.Ekinci).
http://dx.doi.org/10.1016/j.bjane.2016.07.017
Conclusion: Thedeterminationofcausestriggeringvasovagalincidentsseenduringthe applica-tionofspinalanesthesia,betterpatientinformationofregionalanesthesiaimplementationsand anxietyreliefwithpreoperativeanxiolytictreatmentwillhelptoeliminatepotentialvasovagal incidents.
©2016SociedadeBrasileiradeAnestesiologia.Publishedby ElsevierEditoraLtda.Thisisan openaccessarticleundertheCCBY-NC-NDlicense(
http://creativecommons.org/licenses/by-nc-nd/4.0/).
PALAVRAS-CHAVE
Ansiedade; Raquianestesia; Síncope; Vasovagal
Arelac¸ãoentreosníveisdeansiedadenoperíodopré-operatórioeosincidentes vasovagaisduranteaadministrac¸ãoderaquianestesia
Resumo
Justificativa: Oobjetivo desteestudofoiinvestigar arelac¸ãoentreaansiedadenoperíodo pré-operatórioeossintomasvasovagaisobservadosduranteaadministrac¸ãoderaquianestesia apacientessubmetidosàcirurgianasregiõesperianaleinguinal.
Métodos: Oestudoincluiupacientescomcirurgiasagendadasparacorrec¸ãodehérniainguinal, fissuraanal,hemorroidaseexcisãodefístulapilonidal.Foramincluídos210pacientesentre 18-65anoseestadofísicoASAI-II.Aavaliac¸ãodospacientescompreendeuhistóriadetabagismo econsumodeálcool,classificac¸ãoASAeníveldeescolaridade.Ascorrelac¸õesforamavaliadas entreonúmerodetentativasdeaplicac¸ãodaraquianestesiaehistóriadeanestesiacomsintoma vasovagal,níveldeescolaridade,sexo,tabagismoeconsumodeálcool,históriaanestésicae escoresdeansiedade.Oinventáriodoestado(transitório)deansiedade,partedoInventário deAnsiedadeTrac¸o-Estado(StateTraitAnxietyInventory-IDATE),foiusadoparadeterminaros níveisdeansiedadedosparticipantes.Achadosclínicosdevasodilatac¸ãoperiférica,hipotensão, bradicardiaeassistoliaobservadosduranteaadministrac¸ãodaraquianestesiaforam registra-dos.
Resultados: Observamos aumento dos incidentes vasovagais durante a administrac¸ão da raquianestesia emcasoscomescoreselevadosdeansiedade,pacientesdosexomasculinoe pacientessemhistóriaanestésica.Oníveldeescolaridadeeonúmerodepunc¸õescomagulha espinhalnãomostraramterqualquerefeitosobreosincidentesvasovagais.
Conclusão:Determinar as causas que desencadearam os incidentes vasovagais observados duranteaaplicac¸ãodaraquianestesia,fornecerboainformac¸ãoaopacientesobreaanestesia regional epromover alívioda ansiedadecom tratamentoansiolítico nopré-operatório con-tribuirãoparaeliminarpossíveisincidentesvasovagais.
©2016SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Este ´eum artigo OpenAccess sobumalicenc¸aCCBY-NC-ND(
http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Vasovagal syncope, which is also known as vasodepressor
syncope, of neurocardiogenic originsis thought tobe the
resultofabnormalinteractionsoftheneurocardiovascular
mechanismcomplexwhichisnecessaryforthemaintenance
ofsystemicandcerebralperfusion,isoneofthemost
fre-quentlyseensyncopetypes.1
Clinically,syncopehasfourmainparameterswhichmay
beindicators;lossofconsciousness,lossofposturaltonus,
spontaneousrecoveryandcardiovascularfindingsadditional
tomultiple etiologies. In theclassic formof
neurocardio-genicsyncope,cardiovascularfindingssuchashypotension,
bradycardia,palenessandsweatingareseentogetherwith
theclassicsyncopefindings.Eachparameterof
neurocardio-genicsyncopeisrelatedtoanincreaseinvasovagalactivity
andisevaluatedasavasovagalsymptom.2
Although the etiology is not fully known, an increase
in afferent signals to the central nervous system, when
thevagus dorsal motornucleus andthe nucleus ambiguus
responsible for parasympathetic activity in the medulla
arestimulated,inhibitionofsympatheticactivityfollowing
suppressionof the rostral ventromedial and ventrolateral
nucleiresponsibleforsympatheticactivityandthe
activa-tionofparasympatheticactivitycausesyncopebycreating
bradycardiaand/orhypotension.3---7Insyncopeof
neurocar-diogenic origin, severe anxiety may be the origin of the
syncope.
Anxiety is a spontaneous and ambiguous low mood
feeling,thereasonforwhichisunknownandmaybe
expe-riencedwiththesensesoffear,distressandimpendingbad
events.Itisanaturalreactionthatpeopledevelopagainst
situations where they do not feel secure and a kind of
feelingof alertness when a situation is perceived as
life-threatening.Theanxietyincidenceamonghospitalpatients
isbetween 10%and 30%in general.8 Preoperativeanxiety
incidenceinadult patientshasbeen reportedasbetween
Anxietyis healthyandfunctionaluptoacertainlevel.
Therefore, the target related to anxiety in patients
pre-paredpreoperativelyisa‘‘medium’’or‘‘healthy’’levelof anxiety.9
Preoperative anxiety is a situation characterized by
unrest and concern arising from any illness,
hospitaliza-tion, anesthesia and surgery or not knowing what is to
happen.10Anxietyincreasesthestressresponseby
activat-ingthereleaseofneuroendocrinemediatorsinpatients.This
hasanegativeeffectonsurgery,anesthesiaand
postopera-tiverecovery.11
Although bradycardia and cardiac arrestdependent on
vagalreflexesarerarelyconfrontedingeneralandregional
anesthesia, the seriousness of these rare complications
requiresmaximumprecautionstobetaken.
Inpreviousstudies,syncopehasbeenreportedtooccur
atleastoncein3%ofthegeneralpopulationandthisrate
increasesto6%intheelderly.12,13Syncopehasbeen
deter-minedin3%ofallemergencypolyclinicpresentationsandin
1%ofhospitalizedpatients.14 However,withtheexception
ofcase reports,tothebestofourknowledge,therehave
beennostudiesinliteratureonpreoperativeor
periopera-tivesyncopeandtheetiologyhasnotbeencomprehensively
researched.
Inthisstudy,itwasaimedtoinvestigatethefactors
caus-ing reflex bradycardia, seen during the administration of
regionalanesthesiainpatientsundergoingplannedelective
surgeryintheperianalandinguinalregions,andtoevaluate
therelationshipwithpreoperativeanxiety.
Material
and
method
Thestudyincluded210ASA I---IIpatientsaged18---65 years withplannedsurgeryforinguinalherniarepair,analfissure,
hemorrhoid andpilonidal sinus excision. Approval for the
study was granted by the hospital ethics committee and
informed consent was obtained from all patients. Any
patientswhowereilliterateorcouldnotunderstandTurkish
or hadsightandhearingproblems orpsychiatricdisorders
wereexcludedfromthestudy.Theinstant(transient)state
anxietyinventorypartoftheTransientState/TraitAnxiety
inventory(StateTraitAnxietyInventory---STAI)whichis
vali-datedforTurkishpeoplebyÖmerandLeComptein1976was
usedtodeterminetheanxietylevelsoftheparticipants.15
This test comprisestwodifferent subunits,each involving
20itemsthatmeasuretraitandstateanxietiesseparately.
Thetraitanxietysectionwasdesignedtomeasurefeelings
withinthelast7days,andtheothersubunitwasdesigned
to measure current feelings. Participants were requested
to mark one of the options of ‘‘never’’, ‘‘sometimes’’,
‘‘frequently’’ or ‘‘almost always’’, for each item in the
survey.Positivescoresweregivenforitems3,4,6,7,9,12,
13,14,17and18,andnegativescoresweregivenforitems
1,2,5,8,10,11,15,16,19and20inthesurvey.Thescores
weremarkedbyhand.Scoresbetween1(or−1)and4(or
−4)weregivenforeachitemaccordingtothepositiveand
negativecharacteristicsand50wasaddedtothetotalscores
obtained.Thehighestandlowestscoreswereacceptedas
80and20respectively(Fig.1).Thepatientswereevaluated
tohavelow,moderateandhighanxietywhentheyhadSTAI
valuesof20---37as,38---44asand45---80,respectively.
Inthepremedicationroom,beforetheadministrationof
premedication,theSTAIanxietyscalewasappliedtoallthe
patients by an anesthetist and the results were noted. A
recordwasmadeofthepatientage,gender,height,weight,
historyofsmokingandalcoholconsumption,ASAgradeand
educationallevel. An intravascular route wasopened and
the patient wastransferred to the operating theatre.On
Spielberger state trait anxiety inventory Never
(1)
1. Calmed down 2. Safe 3. Tense 4. Annoyed 5. Comfortable 6. Upset
8. Relaxed 9. Anguished 10. At ease
12. Nervous 13. Restless 14. Downhearted 15. Rested 16. Satisfied 17. Concerned 18. Stunned 19. Happy 20. I fell good 11. Self-confidence 7. Concerned with future misfortunes
(2) (3)
Frequently Sometimes
(4) Almost always
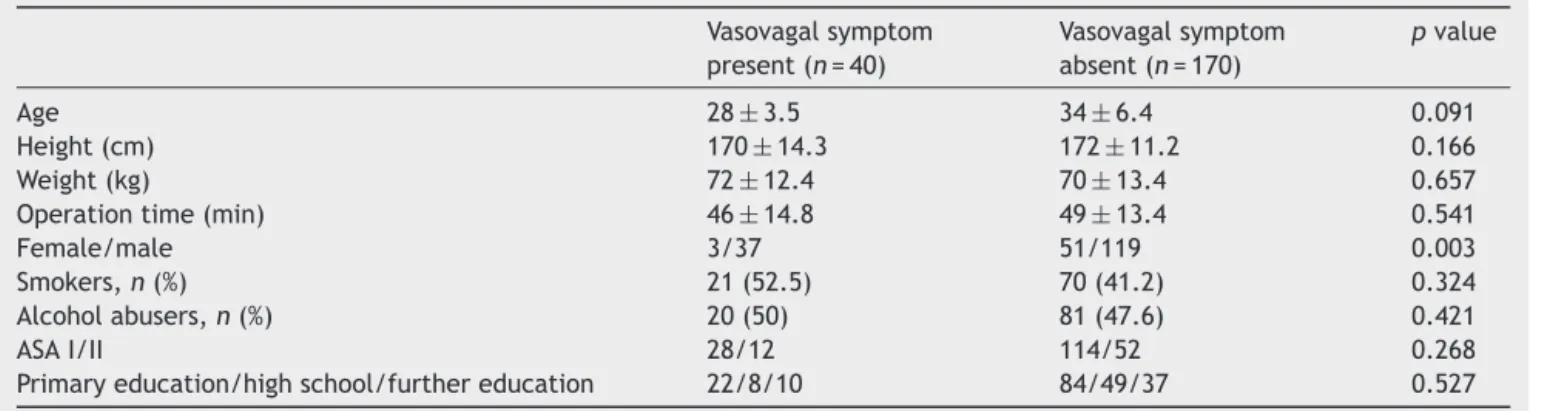
Table1 Demographicfeaturesofthepatients.
Vasovagalsymptom present(n=40)
Vasovagalsymptom absent(n=170)
pvalue
Age 28±3.5 34±6.4 0.091
Height(cm) 170±14.3 172±11.2 0.166
Weight(kg) 72±12.4 70±13.4 0.657
Operationtime(min) 46±14.8 49±13.4 0.541
Female/male 3/37 51/119 0.003
Smokers,n(%) 21(52.5) 70(41.2) 0.324
Alcoholabusers,n(%) 20(50) 81(47.6) 0.421
ASAI/II 28/12 114/52 0.268
Primaryeducation/highschool/furthereducation 22/8/10 84/49/37 0.527
Independentt-test,Pearsonchi-squaretest. SD,standarddeviation.
the operating table, heart rate and rhythm were moni-toredwithelectrocardiography,non-invasivebloodpressure (NIBP)andperipheral oxygensaturation(SpO2)monitoring
were applied. After the monitorization, the patient was moved into a sitting position and the lumbar area was cleaned3timeswithpovidoneiodinethensterile draped. Entry was made with a 26G pencil point spinal needle betweenL4---L5or L3---L4,located withpalpation,and the numberof entriesattemptedfor theapplication ofspinal anesthesiawasrecorded.Thespinalanesthesiawasapplied to all the patients in a sitting position and no anxiolytic wasappliedtoanypatient.Duringtheprocedure,systolic pressure observed <90mmHg and diastolic <60mmHg was evaluatedashypotension,<60bpmasbradycardiaand0bpm as asystole and these values were recorded. In cases of bpm<40,1mgatropinewasadministered.
Statisticalmethods
Thepowerofthestudywasdeterminedas0.99ina confi-dence interval of 95% and at significance level of 0.05. Thisfindingindicatedthatthesamplewassufficient(effect size=0.27).
SPSS 15.0 program wasused in the data analysis. The Shapiro---WilkandLeneve testswereused respectivelyfor theconformityofthedatatonormaldistributionand vari-ancehomogeneity.Parametricandnonparametricmethods wereusedintheanalysisofthevariableswithandwithout homogeneousvarianceandnormaldistributionrespectively. The independent-samples t-test wasusedinthe compari-sonof 2 independentgroups. The Pearsonchi-squaretest was used in the comparison of categorical data. Quanti-tative data were expressed as mean±standard deviation (SD)inthetables.Categoricaldatawereexpressedas num-ber(n)andpercentage(%).Thedatawereanalyzedat95% confidenceintervalandavalueofp<0.05wasacceptedas statisticallysignificant.
Results
Atotalof210patientswereincludedaged18---65yearsof ASA grade I---II. No statistically significant difference was
determinedbetween thoseshowingandnotshowing vaso-vagalsymptomsinrespectofage,height,weight,smoking, alcoholconsumptionorASAgrade(p>0.05)(Table1).
Vasovagal symptoms were observed in a total of 40
patients.Preoperatively,vasovagalsymptomswereseenin
mean19%ofthepatients(Table1).
Therewerenocasesineithergroupwhowereilliterateor hadnotreceivedanyeducation.Nostatisticallysignificant
differencewasseenbetweenthegroupsinrespectof
vaso-vagalsymptomsandlevelofeducation(p>0.05)(Table1).
Themostfrequentlyobservedvasovagalsymptomswere
sweating and dizziness. Cardiogenic origin findings were
observedin27patientsandinoneoftheseanasystolictable
formed.Insomepatients,severalsymptomswereobserved
atthesametime(Table2).
Ofthe40patientsshowingvasovagalsyncopesymptoms,
onehad a history of spinal anesthesia and six of general
anesthesia.Astatisticallysignificantdifferencewas
deter-minedbetweenthegroups inrespectofhistoryofgeneral
andspinalanesthesia(p<0.05)(Table3).
Typeofsurgeryandnumberofspinalpunctureattempts
did not have statistically significant effect on vasovagal
symptomoccurrence(p>0.05)(Table3).
Thepatientshavingvasovagalsymptomshadhighdegree
ofanxiety(STAI>45)atasignificantlyhigherratethanthe patientshavingnosymptoms(p<0.001)(Table4).
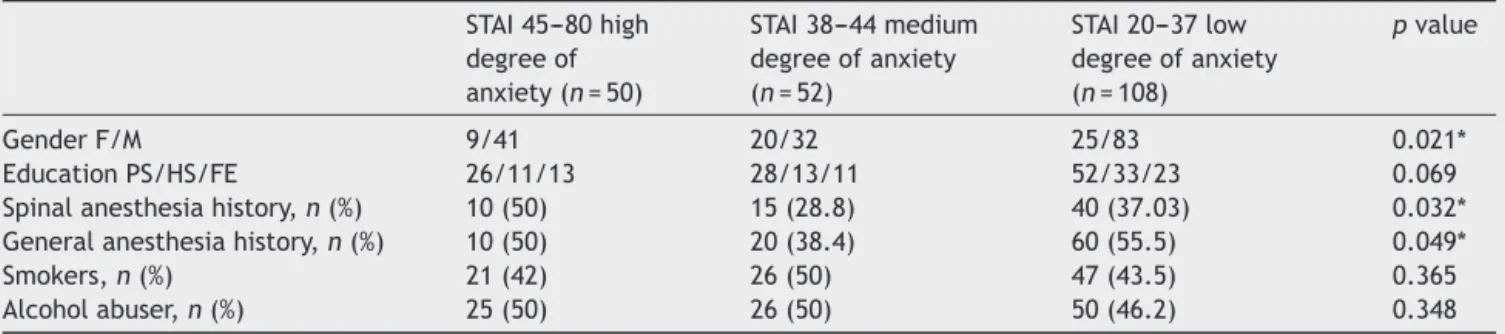
A statistically significant relationship was determined
betweenhighanxiety scoresandgender andnohistoryof
spinalorgeneral anesthesia(p<0.05).Nostatistically
sig-nificantrelationshipwasdeterminedbetweenhighanxiety
scoresandeducationallevel,smokingandalcohol
consump-tion(p>0.05)(Table5).
Table2 Vasovagalincidentsseeninpatients.
Typeofsymptom n(%)
Sudation 30(75%)
Hypotension/dizziness 16(40%)
Bradycardia 10(25%)
Table3 Comparisonofpatient’spreviousanesthesiaexperience,operationtype,numberofspinalpunctureattempts.
Vasovagalsymptom present(n=40)
Vasovagalsymptom absent(n=170)
pvalue
Spinalanesthesiahistory,n(%) 1(2.5) 64(37.6) <0.001
Generalanesthesiahistory,n(%) 6(15) 84(49.4) <0.001
Operationtype
Inguinalhernia 12 42 0.398
Pilonidalsinus 14 80
Analfissure 6 34
Hemorrhoid 8 16
1trial/>1trials 16/24 156/14 0.051
Pearsonchi-squaretest.
Table4 Degreeofanxietyinvasovagalsymptomoccurringandnonoccuringpatients.
Vasovagalsymptom present(n=40)
Vasovagalsymptom absent(n=170)
pvalue
STAI20---37(lowdegreeofanxiety) 2(5%) 106(62.3%) <0.001
STAI38---44(moderatedegreeofanxiety) 8(20%) 44(25.8%) STAI45---80(highdegreeofanxiety) 30(75%) 20(11.9%)
STAI,StateTraitAnxietyInventory. Pearsonchi-squaretest,n(%).
Discussion
In the current study, factors causing vasovagal incidents whichareoftenencounteredduringspinalanesthesiawere investigatedand the relationship withanxiety was evalu-ated.In literature, although thereare many case reports ofpreoperativevasovagalincidentsandvasovagalincidents observedduringregionalanesthesiainterventions,the cur-rentstudypresentsawidercaseseries.16,17
Anxiety is the first response when people confront a
problemandthemostfrequentreactionincasesofillness.
Anxietydevelopsinhospitalpatients,especiallythosewho
aretoundergoanysurgicalintervention.9Inadditionto
sur-gicalinterventions,allanesthesiaapplicationsareperceived
asdangerousbypatientsandbothpreoperativeand
postop-erativestressandtensiondevelopwiththisperception.18
While different tests have been used in the
evalua-tionof preoperativeanxietyinliterature,theuseof STAI,
whichincludesbothastateandtraitanxietyscaleiswidely accepted.19
Preoperative anxiety incidence has been reported
between 11%and92%in varioussurgicalpatientgroups.20
WhileSTAI-Sthreshold,whichisusedforthestateofanxiety withclinicallydistinctivesymptoms,isacceptedas39---40,
it has been determinedas 44---45for patientsin a
preop-erativeperiod.Thereasonfor thisisthatSTAI-Sindicates
howpeoplefeelindependentlyofthepresentsituationsand
circumstances.20
Inthecurrentstudy,patientswithSTAI-Sscores>45were
classifiedashighdegreeanxietyandthesepatients
consti-tuted23%(50)ofthetotalpatientgroup.
Anxietylevelshavebeenreportedtobehigherinfemales
in many studies.20---22 As the hospitalwhere thestudy was
conductedservesamilitarybase,therewasagreater
num-berofmalesinthecurrentstudypopulation.Contrarytothe
generalliteratureinformation,anxietyinfemaleswaslower
Table5 Relationshipsofeducationlevel,gender,smoking,useofalcoholandanesthesiaexperiencewithanxietyscores.
STAI45---80high degreeof anxiety(n=50)
STAI38---44medium degreeofanxiety (n=52)
STAI20---37low degreeofanxiety (n=108)
pvalue
GenderF/M 9/41 20/32 25/83 0.021*
EducationPS/HS/FE 26/11/13 28/13/11 52/33/23 0.069
Spinalanesthesiahistory,n(%) 10(50) 15(28.8) 40(37.03) 0.032*
Generalanesthesiahistory,n(%) 10(50) 20(38.4) 60(55.5) 0.049*
Smokers,n(%) 21(42) 26(50) 47(43.5) 0.365
Alcoholabuser,n(%) 25(50) 26(50) 50(46.2) 0.348
Pearsonchi-squaretest*p<0,05.
thanthatofmalesinthisstudy.Thesignificantlyhigher num-berofmalesinthestudypopulationmaybethereasonfor thisdifference.Whiletheanxietyconnectedwithbeing sep-aratedfromthefamilywasreportedtobehigherinfemales, someresearchershavealsostatedthatfemalesexpresstheir anxietiesmoreeasilythanmales.23
Itwasconsideredthatthisdifferencecouldbeconnected
withlevelsofexpressedemotion beingmorerestrictedin
malesinoursociety.Inthecurrentstudy,itwasdetermined thattheanxietylevelsofmaleswerestatisticallyhigherin
thepreoperativeperiodcomparedtothoseoffemales.
Somestudieshavereportedthatprevioussurgical
experi-encereducedpreoperativeanxietyandthisisexplainedwith
theconditional learningmodel, inwhich an unconditional
fearstimulusisencounteredatshortintervals.22
Whiletherearestudieswhichhavestatedthatthe
anes-thesiaexperiencedidnotchange thepreoperativeanxiety
level,therearealsostudieswhichhavesuggestedthatthe
anesthesiaexperiencereducedanxietyinmen,whileitdid
notaffectanxietyinwomen.23,24 Therearealsostudiesin
literature,whichhavereportedthatpatientswithan
anes-thesia experience of more than 10 years previously had
fewer anesthesia-dependent anxieties compared to those
whohadundergonesurgerywithinthelast10years.10Inthe
currentstudy,regionalandgeneralanesthesiaexperiences
were questioned separately, and a statistically significant
differencewasdeterminedinvasovagalincidencesbetween
thepatientswithandwithoutanesthesiaexperience.
Ithasbeenreportedinliteraturethataphysical status
ofASAIIandaboveandthesizeofoperationaffectedthe
levelofanxiety.Insomestudies,theASAstatuswasreported
to be a determinant of the preoperative anxiety level.22
ThecurrentstudywasappliedtopatientswithASAI---II
sta-tusundergoingoperationswithdischargeonpostoperative
day1attheverylatest, consideringtheexpectedamount
ofbleeding,operationtimeandpostoperative
hospitaliza-tionduration.Nosignificantdifferencewasdeterminedin
termsofASAstatusbetweenthegroupsparticipatinginthis
study.
Someresearchershavestatedthatagewasnotafactor
affecting the anxiety level,12,23,24 although Ramsay
deter-minedthattherateofanxietywashigherinamiddle-aged
patientgroupandconnectedthat withthe family
respon-sibilities of these patients. There is a greater sense of
pre-destinyin olderpatientsandyoungerpatientsmaybe
better informed about health-related negative incidents
throughmediatechnology.10Inthecurrentstudy,thepatient
population with observed vasovagal incidents was mostly
comprisedofyoungerpatients,whichconformswith
liter-ature, although no statistically significant difference was
determinedbetweentwogroups.
Whileithasbeenreportedinsomestudiesthatanxiety
increasedwithanincreasinglevelofeducation,other
stud-ieshaveshownthattheeducationleveldidnotaffectthe
degreeofanxiety.25,26Itwasstatedinonestudythat
preop-erativeanxietylevelswerehigherinthosewhohadreceived
educationformorethan12years.22Inthecurrentstudy,no
relationship wasdetermined between the level of
educa-tionandanxiety.Thelevelofanxietywashigherinpatients
withaprimaryschoollevelofeducationandlowerinthose
whohadattended highschool butthe differencewasnot
statisticallysignificant.
Preoperativenicotine replacementtreatment has been
shownnottohaveany effectonthepreoperative anxiety
levelsofsmokersandthesymptomsdevelopingconnected
todeprivationin smokers didnot clinically create a
seri-ousproblemintheperioperativeperiod.27,28Inthecurrent
study, no difference was observed in the anxiety levels
betweensmokersandnon-smokers.
This study had some limitations, including the
imple-mentationofspinalanesthesiaonly,thatmostofthestudy
populationwasmaleandthe limitednumberofoperation
types.Futurestudiescouldinvestigatevasovagalsymptoms
seenduringtheimplementationofregionalanesthesiaand
peripheralnerveblocks.
Conclusion
The determination of the factors causing vasovagal
inci-dents during spinal anesthesia application has a place in
bothdiagnosis andtreatment astheyshouldbeknownby
both patients and anesthetists. The prevalence of
vaso-vagal incidences increases with high anxiety scores and
absenceofanesthesiahistory.Evaluationoftheanxiety
lev-elsofpatients,reducingunwantedvasovagalproblemswith
preoperativeanxiolyticmedication andinformingpatients
abouttheapplicationofregionalanesthesiawillbehelpful
ineradicatingvasovagalincidents.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.BrignoleM,AlboniP,BendittD,etal.Guidelinesonmanagement (diagnosisandtreatment)ofsyncope-update2004.Executive summary.EurHeartJ.2004;25:2054---72.
2.Abboud F. Neurocardiogenic syncope. N Engl J Med. 1993;328:1117---20.
3.Badner NH, Nielson WR, Munk S, et al. Preoperative anx-iety detection and contributing factors. Can J Anaesth. 1990;37:444---7.
4.KinsellaSM,TuckeyJP.Perioperativebradycardiaandasystole: relationshiptovasovagalsyncopeandtheBezold-Jarischreflex. BrJAnaesth.2001;86:859---68.
5.DoyleDJ, MarkPW. Reflexbradycardiaduringsurgery.CanJ Anaesth.1990;37:219---22.
6.PrakashES,Madanmohan.Whentheheartisstoppedforgood: hypotensionbradycardia paradoxrevisited. Adv PhysiolEduc. 2005;29:15---20.
7.AptL,IsenbergSJ.Theoculo-cardiacreflexasasurgicalaidin identifyingaslippedor‘lost’extraocularmuscle.BrJ Ophthal-mol.1980;64:362---5.
8.Bekaro˘gluM, UluutkuN,Alp K, et al. Ameliyatöncesi kaygı vedepresyondurumununameliyatkomplikasyonlarınaveyatıs¸ süresine etkisi üzerine bir ¸alıs¸ma.c Türk Psikiyatri Dergisi. 1991;2:285---8[inTurkish].
9.Kindler CH, Harms C, Amsler F, et al. The visual analog scaleallows effective measurementofpre-operative anxiety anddetectionofpatient’sanestheticconcerns.AnesthAnalg. 2000;90:706---12.
11.KainZN,SevarinoF,PincusS,etal.Attenuationofthe preoper-ativestressresponsewithmidazolam:effectsonpostoperative outcomes.Anesthesiology.2000;93:141---7.
12.Savage DD, Corwin L, McGee DL, et al. Epidemiologic fea-tures of isolated syncope: the Framingham Study. Stroke. 1985;16:626---9.
13.LipsitzLA,WeiJY,RoweJW.Syncopeinanelderly, institution-alisedpopulation:prevalence,incidence,andassociatedrisk. QJMed.1985;55:45---54.
14.Kapoor W. Evaluation and management of syncope. JAMA. 1992;268:2553---60.
15.LeCompte WA,Ömer N.DevelopmentoftheTurkish edition ofstate-traitanxietyinventory.In:SpielbergCD,DiazGuerro R,editors.Cross-culturalanxiety.Washington,DC:Hemisphere PublishingCo.;1976.p.51---68.
16.JangYE,DoSH,SongI.Vasovagalcardiacarrestduringspinal anesthesiaforCesareansection---acasereport.KoreanJ Anes-thesiol.2013;64:77---81.
17.KimKO, OhJS.Vagallymediatedatrioventricular blockwith ventricularasystoleimmediatelyafterassumingproneposition underspinalanesthesia:acasereport.KoreanJAnesthesiol. 2016;69:63---5.
18.Kehlet H,WilmoreDW.Evidence-basedsurgical careandthe evolutionoffast-tracksurgery.AnnSurg.2008;248:189---98.
19.AykentR,Kocamano˘gluS,ÜstünE,etal.Preoperatifanksiyete nedenleri ve de˘gerlendirilmesi: APAIS ve STAI skorlarının
kars¸ılas¸tırılması.TurkiyeKlinikleriJAnestReanim.2007;5:7---13 [inTurkish].
20.WetschWA,PircherI,LedererW,etal.Preoperativestressand anxiety in day-carepatientsand inpatientsundergoing fast-tracksurgery.BrJAnaesth.2009;103:199---205.
21.MitchellM.Conscioussurgery:influenceoftheenvironmenton patientanxiety.JAdvNurs.2008;64:261---71.
22.Caumo W, Schmidt AP,Schneider CN, et al. Risk factors for postoperativeanxietyinadults.Anaesthesia.2001;56:720---8.
23.DomarAD,EverettLL,KellerMG.Preoperativeanxiety:isita predictableentity?AnesthAnalg.1989;69:763---7.
24.MoermanN,vanDamFS,MullerMJ,etal.TheAmsterdam Pre-operativeAnxietyandInformationScale(APAIS).AnesthAnalg. 1996;82:445---51.
25.DeyirmenjianM,KaramN,SalamehP.Preoperativepatient edu-cationforopen-heartpatients:asourceofanxiety?PatientEduc Couns.2006;62:111---7.
26.BayarA,Tuncay ˙I,AtasoyN,etal.Theeffectofwatchinglive arthroscopicviewsonpostoperativeanxietyofpatients.Knee SurgSportsTraumatolArthrosc.2008;16:982---7.
27.Warner DO, Patten CA, Ames SC, et al. Smoking behavior andperceivedstressincigarettesmokersundergoingelective surgery.Anesthesiology.2004;100:1125---37.