Artigo Original
Haydée Fiszbein Wertzner1
Luciana de Oliveira Pagan-Neves2
Renata Ramos Alves2
Tatiane Faria Barrozo2
Descritores
Patologia da fala e linguagem Fala Testes de articulação da fala Medida da produção da fala Criança Keywords
Speech-language pathology Speech Speech articulation tests Speech production measurement Child
Correspondence address:
Haydée Fiszbein Wertzner
R. Cipotânea, 51, Cidade Universitária, Butantã, São Paulo (SP), Brasil, CEP: 05360-160.
E-mail: [email protected]
Received: 8/3/2011
Accepted: 8/6/2012
Study conducted at the Department of Physical Therapy, Speech-Language Pathology and Audi ology, and Oc-cupational Therapy, School of Medicine, Universidade de São Paulo – USP – São Paulo (SP), Brazil. (1) Department of Physical Therapy, Speech-Language Pathology and Audi ology, and Occupational Therapy, School of Medicine, Universidade de São Paulo – USP – São Paulo (SP), Brazil.
(2) Investigation Laboratory in Phonology, Department of Physical Therapy, Speech-Language Pathology and Audi ology, and Occupational Therapy, School of Medicine, Universidade de São Paulo – USP – São Paulo (SP), Brazil.
Conflict of interests: None
sound disorder
Implicações da diadococinesia oral no transtorno fonológico
ABSTRACT
Purpose: To verify the performance of children with and without speech sound disorder in oral motor skills measured by oral diadochokinesia according to age and gender and to compare the results by two different methods of analysis. Methods: Participants were 72 subjects aged from 5 years to 7 years and 11 months divided into four subgroups according to the presence of speech sound disorder (Study Group and Control Group) and age (≤6 years and 5 months and >6 years and 5 months). Diadochokinesia skills were assessed by the repetition of the sequences ‘pa’, ‘ta’, ‘ka’ and ‘pataka’ measured both manually and by the software Motor Speech Profile®. Results: Gender was statistically different for both groups but it did not influence on the number of sequences per second produced. Correlation between the number of sequences per second and age was observed for all sequences (except for ‘ka’) only for the control group children. Comparison between groups did not indicate differences between the number of sequences per second and age. Results presented strong agreement between the values of oral diadochokinesia measured manually and by MSP. Conclusion:
This research demonstrated the importance of using different methods of analysis on the functional evaluation of oro-motor processing aspects of children with speech sound disorder and evidenced the oro-motor difficulties on children aged under than eight years old.
RESUMO
Objetivo: Verificar o desempenho de crianças com e sem transtorno fonológico nas habilidades motoras orais medidas pela diadococinesia oral, de acordo com as variáveis idade e gênero, além de comparar os métodos de análise manual e por meio de software específico. Métodos: Participaram do estudo 72 sujeitos, com idade entre 5 anos e 7 anos e 11 meses, que foram divididos em quatro subgrupos em função da presença do diag-nóstico de transtorno fonológico (grupo controle e grupo estudo) e da idade (≤6 anos e 5 meses e >6 anos e 5 meses). A diadococinesia oral foi avaliada na repetição das sequências ‘pa’, ‘ta’, ‘ka’ e ‘pataka’ utilizando o método de análise manual e pelo softwareMotor Speech Profile®. Resultados: Houve diferença somente
relacionada à variável gênero nos grupos, mas que não influenciou na produção do número de sequências por segundo. Houve correlação entre o número de sequências por segundo e a idade em todas as sequências, exceto para ‘ka’, somente no grupo controle. Os resultados da comparação entre grupos indicaram que não houve diferença entre as distribuições do número de sequências por segundo nas sequências estudadas nas duas faixas etárias analisadas. Observou-se concordância forte entre as medidas realizadas a partir dos dois métodos.
INTRODUCTION
Different underlying causes, heterogeneity and severity of speech sound disorders (SSD) in children especially address-ing possible diagnostic markers has been extensively studied in the field of Speech and Language Pathology.
Diagnostic evaluation for SSD is based on a speech sample obtained from different tasks (words imitation, picture nam-ing and spontaneous speech) that enable the verification of phonological and phonetic inventory of the child. Despite the importance of these tasks for SSD diagnosis there is still the need to complement the diagnostic in order to provide more detailed information on individual speech development and to help on choosing the most adequate therapeutic model.
Therefore, diagnosis of SSD involves the application of different tasks in an attempt to establish the speech severity (which can be measured by various indexes)(1) and the most
affected ability during phonological acquisition: auditory per-ception, cognitive-linguistic processing or oro-motor speech processing(2-4). Speech errors produced during language
development may be related to children’s ability to plan and execute complex sequences of fine oro-motor sequences required for the articulation of speech(3). The inter-relation
of these processing is responsible for the emergence of first words and also for the phonological knowledge.
Evaluation of oral diadochokinesia (DDK) provides evi-dence about the existence of a relation between speech and oral motor skills. DDK is a complementary procedure for the diagnosis of SSD once it measures the ability to perform rapid repetitions of relatively simple patterns of opposite muscu-lar contractions(3,5-7) evaluating the evolution of neuromotor
maturation and integration of an individual.
DDK measure can be done based on different stimuli and using diverse methods of analysis. In general, the most used stimuli are the repetition of isolated syllables or the repeti-tion of a syllabic sequence during a certain period of time(8).
The most cited in the literature both for English(5,6,8) and for
Brazilian Portuguese(9-13) are the repetition of one isolated
syllable (pa, ta, ka) and also the repetition of a trisyllable (pataka).
One of the major difficulties in comparing the results of different studies presenting results based on the number of repetitions in a certain period of time during DDK analysis is related to the variability described in data collection(14).
DDK analysis can be hand-measured or automatic. Literature describes some studies using hand measurement for counting the number of sequences produced by an individual during a predetermined period of time(9,14), to count the time
that the individual takes to perform a number of repetitions(15)
and some to do both measures(7). Hand-measure is easy to
be used by speech pathologists but the professional must be careful with both the data collection and the analysis of the sequences.
On the other hand DDK measured using an automatic diadochokinetic rate analyzer provides greater efficiency on the results since in addition to quantifying the number of sequences produced the software is also able to make many
different analyses. The Motor Speech Profile (MSP) model 5141 manufactured by KayPentax® which is an optional software to be coupled to the Computerized Speech Lab (CSL) gives the user the possibility of obtaining information such as average DDK period, rate and peak intensity, coef-ficient variation of DDK period and peak intensity and other different measures(14).
A recently published study analyzed oral DDK using the software MSP in typically developing Brazilian Portuguese-speaking children aged between eight and ten years-old. The study indicated that the mean number of sequences per second ranged from 4.8 to 5.2 for the syllable ‘pa’, between 4.9 and 5.4 for ‘ta’ and between 4.3 and 4.9 for ‘ka’(13).
Another study(15) analyzing hand-measured DDK of the
tryssilable ‘pataka’ in both typically developing and children with SSD aged between five and ten years-old indicated that the use of DDK for diagnostic purposes is an evaluation of high discriminatory power to confirm the diagnosis of SSD in children aged over eight years-old. The cutoff value of 1.4 sequences per second presented at the study was able to separate subjects with from subjects without SSD.
Based on the literature review the hypothesis that moti-vated this study are: (1) typically developing children produce more sequences per second than children with SSD at the DDK evaluation; (2) there is no difference between the hand-measure and automatic analysis of DDK; (3) older children produce more sequences per second than the younger.
The aim of this study was to verify the performance of the oro-motor abilities measured by DDK in children with and without SSD according to age and gender and to compare hand-measure versus automatic analysis.
METHODS
This study was approved by the Ethics Commission for the Analysis of Research Projects (CAPPesq) of the Clinical Board of the General Hospital and School of Medicine of the Universidade de São Paulo (0958/08). Written, informed consent was obtained from the parent of each participant.
Participants were 72 male and female children aged be-tween five and seven years and eleven months-old divided into two groups with 36 children each one according to the presence of SSD (experimental group-EG) or the absence of the disorder (control group-CG). Age matching was not possible because of sample loss especially related to absences during evaluation process.
Inclusion criteria for CG included parental and teacher report of no history of auditory, language and speech impair-ment, adequate performance at both the phonology test(16)
from the Child Language Test ABFW(17) and at spontaneous
speech analysis based on the retelling of a history of the book Esconde-Esconde(18).
Inclusion criteria for EG included the positive diagnostic of SSD based on the same phonology test(16) and on parental
report.
coupled to a high performance and fidelity microfone from Kay Pentax® model 3706. Phonology and spontaneous speech samples were recorded using the H2 Handy recorder from Zoom coupled to the microfone Vocal Evolution 817 from Sennheiser. Speech samples were recorded inside an acoustically treated room.
The number of sequences produced during the pre--established time was both hand-analyzed by visualizing the speech waveform at CSL as an auxiliary tool and also auto-matically analyzed by the software Motor Speech Profile® (MSP-model 5141).
Procedures for the application of experimental tests
To collect the speaking data of DDK participants were asked to repeat three CV syllables ‘pa’, ‘ta’, ‘ka’ and the trissylabic sequence ‘pataka’ for 10 seconds. Examiner´s instructions for the child were to “repeat the sequences as fast as you can while you see my arm raised; when I lower my arm you can stop the repetitions”. Examiner began to count up to 10 seconds when the first sequence was produced by the child. Respiratory or any other sort of pause was discounted from the 10 seconds. The initial training conducted before the definitive collection of DDK data was based on the repetition of the sequence ‘badaga’. Sequences were collected in diffe-rent orders to avoid possible bias during the study.
Hand-measurement was done for all the 72 subjects (36 from CG and 36 from EG). Speech samples analyzed using the MSP software was done for 15 children from CG and 12 from EG due to the occurrence of sample losses.
Sample losses on both groups occurred especially because of the difficulties of concentration and equipment´s stability required for the collection of good data to be analyzed by the acoustic analysis software. For the CG speech sample losses occurred because children were not able to come on the scheduled day to the university to record the data. For the EG speech sample losses occurred because of the interferences during speech collection which precluded data analysis such as problems with the variation of speech intensity during production and background noise.
Hand-measurement data analysis
Hand-made analysis was done by counting the number of sequences divided by the time of production (five seconds). The three initial seconds and the two final seconds were exclu-ded so only the five medial seconds were analyzed. Counting was done based on both audio (recorded signal) and visual images (spectrogram).
Data analysis using MSP
MSP analyzes and extract speech parameters that are important on the identification of motor difficulties. The analysis proposed measures the ability of a child in repeating a consonant-vowel combination in a quick, steady and rhyth-mic manner as described by MSP manual(19). The software
extracts 11 acoustic parameters but in this study only DDKavr (the parameter that shows the mean number of repetitions in seconds) was analyzed.
For the analysis by MSP the first and the last seconds from the recorded speech were discarded (eight seconds were analyzed), following the instructions for the necessary time for analysis by MSP(19).
Statistics
Age distribution was done by T-test and gender by chi--square test. The number of sequences per second was com-pared by Mann-Whitney test. Spearman correlation verified a possible correlation between age and the parameters from the study. T-test was applied when no correlation was observed.
Groups were subdivided according to the median of age (6 years and 5 months) when correlation between age and the parameters from the study was observed (≤6 years and 5 months and >6 years and 5 months).
After this subdivision, four new subgroups were com-bined: CG with ≤6 years and 5 months, CG with >6 years and 5 months children, EG with ≤6 years and 5 months chil-dren and finally EG with >6 years and 5 months chilchil-dren. Kruskal-Wallis test was done to compare the four subgroups. Bonferroni correction was used when necessary. Concordance between hand-measurement of DDK and the analysis by MSP was done by the coefficient of intraclass correlation.
RESULTS
Characteristics of children according to gender and age
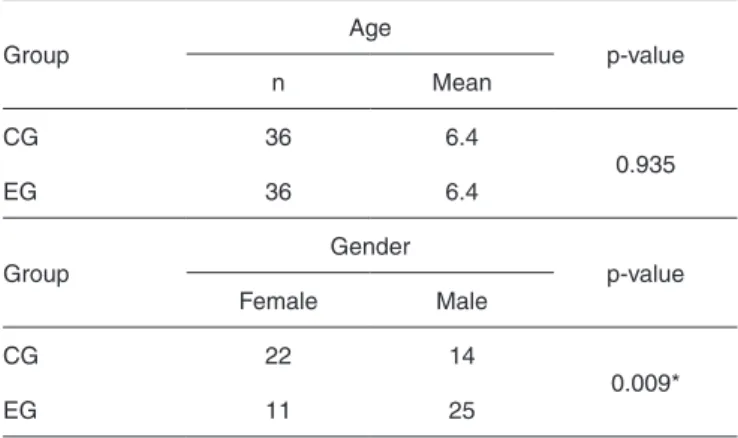
Comparative analysis between children from CG and EG according to age and gender is indicated in Table 1. Difference was observed only for gender.
DDK performance according to hand-measurement
All children (36 of each group) participated from the hand-made analysis of DDK. Intra-group gender comparison
Table 1. Comparative analysis between gender and age for both groups
Group
Age
p-value
n Mean
CG 36 6.4
0.935
EG 36 6.4
Group
Gender
p-value
Female Male
CG 22 14
0.009*
EG 11 25
* Significant values(p≤0.05) – T-student and Chi-square tests
was made for all the sequences from the task. P-values are indicated at Table 2. No difference between gender and the number of sequences per second was observed.
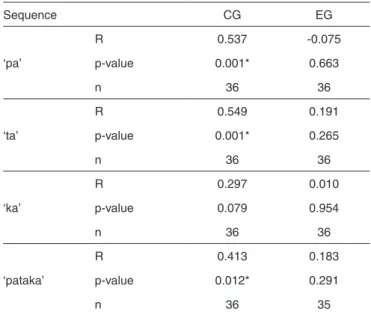
Analysis of the EG did not indicate correlation between the number of sequences per second and age. The sequence ‘ka’ was different only for the CG analysis (Table 3).
Comparison between groups from the number of repeti-tions of the sequence ‘ka’ per second (Mann-Whitney test) indicated no difference (p=0.478). Kruskal-Wallis test was used to compare the distribution of the number of sequences per second between CG and EG for the other sequences where age analysis indicated statistical differences for CG. Subjects were then grouped into two other different subgroups accor-ding to age (≤6 years and 5 months; >6 years and 5 months). Results for this comparison indicated no difference between the distribution of the number of sequences per second for children aged ≤6 years and 5 months for ‘pa’(p=0.078), ‘ta’ (p=0.396) and ‘pataka’ (p>0.999) and also for the subgroup aged >6 years and 5 months for ‘pa’ (p>0.999), ‘ta’ (p=0.408) and ‘pataka’ (p=0.078).
Comparison between hand-measurement and MSP analysis
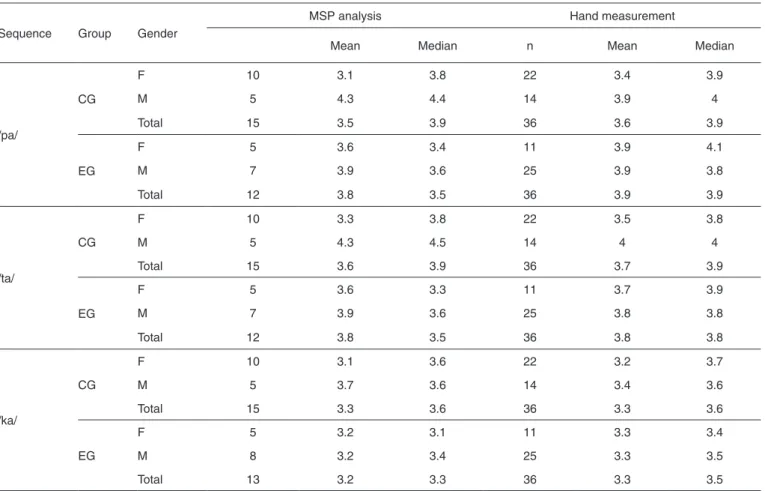
Concordance analysis between the number of sequences per second analyzed by hand-measure and MSP was applied only for the monosyllabic sequences ‘pa’, ‘ta’, ‘ka’ because the speech program analyzes only monosyllables. Descriptive data from both measures are presented in Table 4.
The coefficient of intraclass correlation was applied to verify the concordance between the two measurements (Table 5). Results for the three sequences demonstrated a coefficient higher than 0.9 which indicates a strong concordance between the two methods of analysis.
DISCUSSION
Heterogeneity of children with SSD related to the cause of the disorder, manifestation and severity still is a frequent theme of researches. The use of complementary and specific phonology tests contributes for a better understanding of SSD´s characteristics. Such complementary tests shall clarify the speech evaluation for a better characterization of the most
committed impaired processing or even for the interaction between them.
The complementary task of oral DDK used at the present research may provide evidences of a deficit at the speech motor programming(10,20). Both the application and analysis of
the oral DDK testing depend on: the age of the participants, the data collection (the command given to the subject), the duration of the sequences, the type of sequence analyzed and the acoustic treatment of the recorded data. These questions are addressed by many published studies(5,9,10,12,14,15, 21,22) what
turns difficult the comparison between them.
At the present study the analysis of oral DDK indicated that despite the difference of gender and age there was no difference between gender and the number of sequences per second for both CG and EG.
Another study with typically developing children(13)
de-monstrated differences between oral DDK and gender (only for the sequences ´pataka´ and ´ta´) but age of the children was superior to the participants from the present study. This study points to the fact that younger children behave similarly independently of their gender.
Literature(23-28) demonstratres that speech motor abilities
in children are refined after eight years old and are much more variable in articulatory patterns until 14–16 years of age. This is an indication that children younger than eight do not present sufficient neuromuscular control to produce all the sequences of sounds and need to adopt different motor strategies to approximate to the adult speech model(28). As
children from the present research were younger than eight years of age we believe that they do not have the proper motor maturation required to the correct production of sounds in terms of velocity and precision(15) what suggests that children
as old as seven years and eleven months of age present the same patterns of motor control independently of the gender.
Table 2. P-values from the equality test of distribution of the number of sequences per second for the groups
Sequence CG EG
‘pa’ 0.363 0.891
‘ta’ 0.372 0.642
‘ka’ 0.697 0.594
‘pataka’ 0.108 0.887
Mann-Whitney test (p≤0.05)
Note: EG = experimental group; CG = control group
Table 3. Correlation between hand-measurement and MSP analysis of the number of sequences per second
Sequence CG EG
‘pa’
R 0.537 -0.075
p-value 0.001* 0.663
n 36 36
‘ta’
R 0.549 0.191
p-value 0.001* 0.265
n 36 36
‘ka’
R 0.297 0.010
p-value 0.079 0.954
n 36 36
‘pataka’
R 0.413 0.183
p-value 0.012* 0.291
n 36 35
* Significant values (p≤0.05) – Spearman correlation test
The fact that we observed a positive correlation between age and the number of sequences per second using the hand--measurement only for the children from CG, but not for the EG ones reinforces this finding. The absence of a correla-tion with children from the EG may indicate an increased difficulty of this children on maturational and neuromotor integrational aspects since they do not present an increasing number of sequences per second with age growth(29) (even
though comparison between groups and age did not point to differences).
Comparison between groups from the children aged >6 years and 5 months for the repetition of the sequence ´pataka´ showed a tendency to significance. This is an indication that the repetition of this specific sequence may demonstrate important information relative to the fast speech movements required to the speech production and also that the higher is the children age, the more reliable the information is.
The mean number of sequences per second of the sequen-ce ´pataka´ was always higher for CG in comparison to EG. Even though this comparison was not different it suggests that children with SSD present difficult at the sequencing of motor patterns necessary for speech production.
This fact is related to the greater level of control deman-ded by the polysyllabic sequences when compared to the monosyllabic ones. A greater number of syllables implies into a larger number of articulatory gestures and motor program-ming(10,13) which may interfere at the difficulties observed in
children with SSD.
The question of age and type of sequence was also discus-sed in other study(10,15) in which it was demonstrated that DDK
test evaluated by the sequence ‘pataka’ was able to separate groups of children with from without SSD after the age of 8 years with high sensitivity and specificity.
Strong correlation was observed between hand-measure-ment and MSP analysis of DDK demonstrating that the two measures are quite reliable. This is an important result since it indicates that hand-measurement is a reliable option for the analysis of DDK. It is important to note that for hand--measure analysis some rules were established (described at the methods section) that may have influenced the results. We recommend professionals to follow such instructions so that biases do not occur.
The use of DDK measure in this study demonstrated a
Table 5. Concordance between hand-measurement and MSP analysis of the number of sequences per second
Sequece Coefficient Confidence interval (95%)
‘pa’ 0.94 [0.88; 0.97]
‘ta’ 0.91 [0.80; 0.96]
‘ka’ 0.95 [0.87; 0.98]
Intraclass correlation coefficient test
Table 4. Descriptive statistics of the number of sequences per second by hand-measured and MSP analysis
Sequence Group Gender
MSP analysis Hand measurement
Mean Median n Mean Median
/pa/
CG
F 10 3.1 3.8 22 3.4 3.9
M 5 4.3 4.4 14 3.9 4
Total 15 3.5 3.9 36 3.6 3.9
EG
F 5 3.6 3.4 11 3.9 4.1
M 7 3.9 3.6 25 3.9 3.8
Total 12 3.8 3.5 36 3.9 3.9
/ta/
CG
F 10 3.3 3.8 22 3.5 3.8
M 5 4.3 4.5 14 4 4
Total 15 3.6 3.9 36 3.7 3.9
EG
F 5 3.6 3.3 11 3.7 3.9
M 7 3.9 3.6 25 3.8 3.8
Total 12 3.8 3.5 36 3.8 3.8
/ka/
CG
F 10 3.1 3.6 22 3.2 3.7
M 5 3.7 3.6 14 3.4 3.6
Total 15 3.3 3.6 36 3.3 3.6
EG
F 5 3.2 3.1 11 3.3 3.4
M 8 3.2 3.4 25 3.3 3.5
Total 13 3.2 3.3 36 3.3 3.5
tendency of children with SSD to produce fewer sequences per second what is more evident at the sequence ‘pataka’. Furthermore we observed correlation between the number of sequences per second and age for the CG children indicating that as age increases maturational processes also increases as indicated by the velocity of the production of sequences.
Evidences from the analysis of DDK provided important information to complement the diagnosis of SSD highlighting that articulatory production of syllables in sequence seems to be better to differentiate groups than the repetition of isolated syllables(21) which highlights the influence of the extent of
word during speech motor control.
Results of this study encourage further research to verify the interference of both time of production and type of syllable sequence during the analysis of DDK in children with SSD.
CONCLUSION
Studies in children with SSD are still very focused on the description of its manifestation characteristics. This study demonstrated the importance of a functional evaluation of other aspects of oro-motor speech processing by using two different methods of analysis of DDK.
Although no correlation between DDK measurement and age have been observed, there was no difference between groups indicating that children aged between 5 and 7 years and 11 months are still improving their motor speech deve-lopment and therefore it was not possible to differentiate children with from children without a diagnosis SSD during the evaluation of DDK.
The fact that there was no difference between genders in both groups suggests that children aged between 5 and 7 years and 11 months exhibit similar abilities (regardless of gender) related to the rapid repetition of sequences of the oral DDK test.
Agreement between the two methods of analysis indica-ted that hand-measure is an option as reliable as the analysis performed by the MSP software.
ACKNOWLEDGEMENTS
This work was supported by Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP) grant 2008/57145- 2.
* HFW designed the study, participated in data collection and analysis, conclusion of findings and manuscript elaboration; LOPN contributed with data tabulation, conclusion of findings and manuscript elaboration; RAR participated in data collection and analysis, and manuscript elaboration; TFB contributed with data collection and tabulation, and manuscript elaboration.
REFERENCES
1. Shriberg LD, Austin D, Lewis BA, McSweeny JL, Wilson DL. The speech disorders classification system (SDCS): extensions and lifespan reference data. J Speech Lang Hear Res. 1997;40(4):723-40.
2. Dodd B, McIntosh B. The input processing, cognitive linguistic and oro-motor skills of children with speech difficulty. J Speech Lang Pathol. 2008;10(3):169-78.
3. Dodd B, McIntosh B. Two-year-old phonology: impact of intput, motor and cognitive abilities on development. J Child Lang. 2010 Nov;37(5):1027-46.
4. Castro MM, Wertzner, HF. Speech inconsistency index in brazilian portuguese-speaking children. Folia Phoniatr Logop. 2011;63(5):237-41. 5. Williams P, Stackhouse J. Diadochokinetic skills: normal and atypical
performance in children aged 3-5 years. Int J Lang Commun Disord. 1998;33:481-6.
6. Williams P, Stackhouse J. Rate, accuracy and consistency: diadochokinetic performance of young, normally developing children. Clin Linguist Phon. 2000;14(4):267-93.
7. Prathanee B, Thanaviratananich S, Pongjanyakul A. Oral diadochokinetic rates for normal Thai children. Int J Lang Commun Disord. 2003 Oct-Dec;38(4):417-28.
8. Gadesmann M, Miller N. Reliability of speech diadochokinetic test measurement. Int J Lang Commun Disord. 2008 Jan-Feb;43(1):41-54. 9. Modolo, D. J. Diadococinesia oral e laríngea em crianças. [dissertação].
São Paulo: Faculdade de Odontologia de Bauru da Universidade de São Paulo; 2007.
10. Wertzner HF, Alves RR, Ramos ACO. Análise do desenvolvimento das habilidades diadococinéticas orais em crianças normais e com transtorno fonológico. Rev Soc Bras Fonoaudiol. 2008 Abr-Jun;13(2):136-42. 11. Folha GA, Felício CM. Relações entre idade, porcentagem de consoantes
corretas e velocidades de fala. Pro Fono. 2009 Jan-Mar;21(1):39-44. 12. Andrade CRF, Queiróz DP, Sassi FC. Eletromiografia e diadococinesia:
estudo com crianças fluentes e com gagueira. Pro Fono. 2010 Abr-Jun;22(2):77-82.
13. Modolo DJ, Berretin-Felix G, Genaro KF, Brasolotto AG. Oral and vocal fold diadochokinesis in children. Folia Phoniatr Logop. 2011;63:1-8. 14. Wang YT, Kent RD, Duffy JR, Thomas JE. Analysis of diadochokinesis
in ataxic dysarthria using the motor speech profile program. Folia Phoniatr Logop. 2009;61(1):1-11.
15. Alves RR. Diadococinesia oral em crianças com e sem transtorno fonológico [tese]. São Paulo: Faculdade de Filosofia, Letras e Ciências Humanas da Universidade de São Paulo; 2011.
16. Wertzner HF. Fonologia. In: Andrade CRF, Befi-Lopes DM, Fernandes FDM, Wertzner HF. ABFW: teste de linguagem infantil nas áreas de fonologia, vocabulário, fluência e pragmática. 2a ed. Barueri - SP: Pró-Fono; 2004. p. 5-31.
17. Andrade CRF, Befi-Lopes DM, Fernandes FDM, Wertzner HF. ABFW: teste de linguagem infantil nas áreas de fonologia, vocabulário, fluência e pragmática. 2a ed. Barueri- SP: Pró-Fono; 2004.
18. Furnari, E. Esconde- Esconde. São Paulo: Ática; 1993.
19. KayPENTAX. Software Motor Speech Profile (MSP) Model 5141,
software instruction manual. Lincoln Park, NJ: KayPentax; 2008. 20. Castro MM, Wertzner HF. Influence of sensory cues on the stimulability
for liquid sounds in brazilian portuguese-speaking children. Folia Phoniatr Logop. 2009;61(5):283-7.
21. Kent RD, Kent JF, Rosenberk JC. Maximum performance tests of speech production. J Speech Lang Hear Disord. 1987 Nov;52:367-87. 22. Depret MMP. Análise da diadococinesia articulatória e laríngea em
indivíduos com e sem transtornos neurológicos. [dissertação]. São Paulo: Universidade Federal de São Paulo; 2005.
23. Kent RD. Motor control: neurophysiology and functional development. In: Caruso AJ, Strand EA. Clinical management of motor speech disorders in children. New York: Thieme Medical Publishers, 1999. p. 29-71.
24. Green JR, Moore CA, Higashikawa M, Steeve RW. The physiologic development of speech motor control: lip and jaw coordination. J Speech Lang Hear Res. 2000 Feb;43(1):239-55.
25. Green JR, Moore C, Reilly K. The sequencial development of jaw and lip control for speech. J. Seepch Lang Hear Res. 2002 Feb;45(1):66-79. 26. Nip IS, Green JR, Marx DB. Early speech motor development:
27. Smith A. Development of neural control of orofacial movements for speech. In: Hardcastle WJ, Laver J, Gibbon FE. The handbook of phonetic sciences. 2a. ed. Wiley-Blackwell, 2010. p. 251-96.
28. Smith A. Speech motor development: integrating muscles, movements, and linguistic units. J Commun Disord. 2006 Sep-Oct:39(5):331-49.