w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Intra-articular
injections
of
triamcinolone
hexacetonide
in
rheumatoid
arthritis:
short
and
long-term
improvement
predictors
Rita
Nely
Vilar
Furtado,
Flavia
Soares
Machado,
Karine
Rodrigues
da
Luz,
Marla
Francisca
dos
Santos,
Monique
Sayuri
Konai,
Roberta
Vilela
Lopes,
Jamil
Natour
∗UniversidadeFederaldeSãoPaulo,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received9January2014 Accepted8August2014 Availableonline5January2015
Keywords: Injection
Triamcinolonehexacetonide Arthritisrheumatoid Predictions
a
b
s
t
r
a
c
t
Objectives:Identifygoodresponsepredictorstointra-articularinjection(IAI)with triamci-nolonehexacetonide(TH).
Methods:Thisstudywascarriedoutinrheumatoidarthritis(RA)patients(AmericanCollege ofRheumatologycriteria)submittedtoIAI(mono,pauciorpolyarticularinjection). Assessment:a“blinded”observerprospectivelyevaluatedjointsatoneweek(T1),fourweeks (T4),twelveweeks(T12)and24weeks(T24)afterIAI.Outcomemeasurementsincluded VisualAnalogue Scale (0-10cm)at rest, inmovement and forswollen joints. Clinical, demographicandvariablesrelatedtoinjectionatbaselinewereanalyzedaccordingtoIAI response.
Results:Westudied289patientswithRA(635joints)withameanageof48.7years(±10.68), 48.5%ofthem Caucasians,VASforglobalpain=6.52(±1.73). Underunivariateanalysis, thevariablesrelatingthebestresponsesfollowingIAI(improvement>70%)were:“elbow andmetacarpophalangeal(MCP)IAI,andfunctionalclassII”.Undermultivariateanalysis, “males”and“non-whites”werethepredictorswiththebestresponsetoIAIatT4,while “elbowandMCPIAI”,“polyarticularinjection”,“useofmethotrexate”and“highertotaldose ofTH”obtainedthebestresponseatT24.
Conclusion:SeveralpredictorsofgoodresponsetoIAIinpatientswithRAwereidentified. Thebest-responsepredictorsforTHIAIoflongtermwere“injectelbowandMCPIAI”and “performpolyarticularinjection”.
©2014ElsevierEditoraLtda.Allrightsreserved.
∗ Correspondingauthor.
E-mail:[email protected](J.Natour).
http://dx.doi.org/10.1016/j.rbre.2014.08.016
Infiltrac¸ões
intra-articulares
de
triancinolona
hexacetonida
na
artrite
reumatóide:
preditores
de
melhora
a
curto
e
longo
prazo
Palavras-chave: Infiltrac¸ão
Triancinolonahexacetonida Artritereumatoide Prognósticos
r
e
s
u
m
o
Objetivos: Identificarfatorespreditoresderespostaàinfiltrac¸ãointra-articular(IIA)com hexacetonidedetriancinolona(HT).
Métodos: Esteestudofoirealizadoem pacientescomartritereumatoide(AR)(segundo critériosdoAmericanCollegeofRheumatology)submetidosàIIA(infiltrac¸ãomono,pauciou poliarticular).
Avaliac¸ão: Umobservador“cego”avaliouprospectivamenteasarticulac¸õesumasemana (T1),quatro semanas(T4), 12 semanas(T12)e 24 semanas(T24)apósIIA. Asmedidas dedesfechoforamEscalaVisualAnalógica(0-10cm)emrepouso,emmovimentoepara articulac¸õesedemaciadas.Asvariáveisclínicasedemográficaseaquelasrelacionadasà infiltrac¸ãonoiníciodoestudoforamanalisadasdeacordocomarespostaàIIA.
Resultados: Foramestudados289pacientescomAR(635articulac¸ões)commédiadeidade de48,7(±10,68)anos;48,5%eramcaucasianos,EVAparadorglobal=6,52(±1,73).Naanálise univariada,asvariáveisrelativasàsmelhoresrespostasseguidaàIIA(melhora>70%)foram: “IIAnocotoveloemetacarpofalangeanas(MCF)”e“classefuncionalII”.Naanálise multi-variada,“homens”e“nãobrancos”foramospreditorescommelhorrespostaàIIAemT4, enquanto“IIAnocotoveloeMCF”,“infiltrac¸ãopoliarticular”,“usodemetotrexato”e“dose totalmaiordeHT”obtiveramamelhorrespostaemT24.
Conclusão:ForamidentificadosdiversosfatorespreditoresdeboarespostaàIIAempacientes comAR.OspreditoresdemelhorrespostaparaIIAdeHTemlongoprazoforam“realizar IIAnocotoveloeMCF”e“realizarinfiltrac¸ãopoliarticular”.
©2014ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Althoughintra-articularinjectionofcorticosteroids(IAIC)has been a commonly used procedure amongrheumatologists foroverhalfacentury,1fewstudieshavebeenconductedto demonstrateitsbenefitsinaccordancetoscientific method-ology.
Rheumatoid arthritis (RA) is the rheumatic condition that most severely affects the joints. Pannus, the hyper-trophic and hyperplasic synovial membrane formed, is an aggressive tissue that damages articular and periarticular structures, whether through the release of metalopro-teinasesoritsmechanicalinvasionofthesurroundingjoint space.2–4
EventhoughRAtreatmenthasevolvedinrecentdecades with the advent of immunobiological therapy allied with disease-modifyingantirheumaticdrugs(DMARDs),5patients withmonoor oligoarticularsynovitismay persist.Inthese cases,IAICcanbeausefultherapeutictool.
It is known that triamcinolone hexacetonide (TH) is the drug of choice for intra-articular treatment of RA, givenitssynovialatrophyingpropertiesandslowabsorption from the injection site.6–13 On the other hand, if injected outside of the joint, it can cause serious adverse local effects.14
ThoughsomeconceptsconcerningIAIChavebeen estab-lished,fewstudieshavebeenconductedtoevaluateresponse predictorsinadultRApatients.15Inaddition,tothebestofour knowledge,noneofthemevaluatedTHIAICresponse predic-torsinpatientswithestablishedRA.
The aim of this study was to identify variables (clini-cal,demographicandrelatedtoinjection)thatserveasthe best predictors of response to TH IAIC over short term (4 weeks)andlongterm(24weeks)inpatientswithestablished RA.
Materials
and
methods
Aprospectivenon-controlledstudywasconductedonacohort of patientswith establishedRA receiving treatmentat the InterventionalRheumatologyUnitatUniversidadeFederalde SãoPaulo(UNIFESP),SãoPaulo,Brazil.
PatientswereclassifiedaccordingtoAmericanCollegeof Rheumatology–ACR16criteria,andhadbeenreferredforIAIC (mono,pauciorpolyarticular).
Inclusioncriteriawere:agebetween18and65;functional classIIorIII;17 stableDMARDforthelast3months;stable oralcorticosteroidforthelastmonth;indicationforIAIC injec-tion(persistentsynovitiswithswellingandarticularpain)and musthavesignedtheinformedconsentform.
Exclusioncriteriawere:IAICinanyjointwithinthelast6 months;anysymptomsofsystemicorarticularinfection;any formofclottingdisturbance;diagnosisofdiabetesmellitusor systemicarterialhypertension;knownallergytocontrastsor radioisotopes,andsuspicionofpregnancy.
Intervention
PatientsreceivedIAICinoneormoreofthefollowingjoints: shoulder(glenohumeral),elbow,wrist,metacarpophalangeal (MCP), knee and ankle. The procedure was carried onlyat thebaselinebythesamerheumatologist,withovertenyears ofexperienceininterventionalrheumatology(RNVFurtado). TheIAICwasmono,pauci(uptothreeinfiltrationsatonce) orpolyarticular(4to8simultaneousIAIC),dependingonthe numberofjointsindicatingpainandswelling.
Theonlycorticosteroid usedwastriamcinolone hexace-tonide(20mg/mL).Dependingonthesizeofthejointspace, doseofcorticosteroidwasconsideredlow(1),medium(2)and high (3). Thedose ofTH usedforeach joint studied were: shoulder,80mg(3);elbow,40mg(2)or60mg(3);wrist,30mg (2)or40mg(3);metacarpophalangeal,10mg(2)or20mg(3); knee,40mg(1),60mg(2)or80mg(3);andankle,40mg(2)or 60mg(3).
PatientsreceivedtheIAICprocedureindorsaldecumbency aftertheinjectionsitehadbeencleansedwithtopical povi-dine.Onlysterileneedlesandsyringeswereused.Xylocaine chloride2%withoutvasoconstrictorwasusedforanesthetic purpose.THwasonlyadministeredoncetheneedlehadbeen correctedpositionedinsidethejointspace.
InpatientssubmittedtokneeIAICwithradioisotopes,all thesafetynormsforradioactivematerialhandlingwere fol-lowed.Thedoseappliedwas5mCiYttrium-90plus40mgof TH,or15mCiSamarium-153hydroxyapatiteplus40mgofTH, dependingonavailability.Thesedrugswereusedonlyincases ofrefractorysynovitisonlyintheknee.
Allpatientswerewarnedtorestforaperiodof48hours afterinjection,onlyallowedto movearound tomeettheir physiologicalneeds.Anorthoticimmobilizerwasusedincase ofIAIwithradioisotopes.
Assessment
“Blinded”examinationatT0(baseline),T1,T4,T12,andT24 weeks post-injection were performed. Outcome measures included:visualanaloguescale(0-10cm)forjointpainatrest (VASr);visualanaloguescale(0-10cm)forjointpainin move-ment(VASmv)and visualanaloguescale forswollenjoints (VASs).
IAICresponsewasassessedinrelationtotheinjectedjoint (ratherthanthepatientasawhole)andwasmeasuredas per-centage(%) ofimprovementontheVASr,VASmv andVASs scalesforeachjointattimesT1,T4,T12andT24.Improvement between50%and70%wasconsideredmoderate,andover70% wasconsideredsignificant.Theassociationbetween improve-mentpercentagesforVASr,VASmv and VASswas madein isolation(50%-70%and>70%)and concomitantly (improve-ment>50% inall threeVASatonce)andmultiplebaseline variableswerefactoredin.
Baseline variables considered under this analysis were: demographic (gender, age and skin color – white or non-white);relatedtodisease(duration,functionalclassIIorIII, presenceofrheumatoidfactor, DMARDSinuse, useoforal corticosteroid and presence of extra-articular disease) and relatedto injection(joint injected, previousIAI, number of
joints injected, TH dose, total TH dose per patient, image guidedIAIanduseofradioisotopeorcontrastagent).
Statisticalanalysis
The continuous variables were described in mean and standarddeviation(SD),andthecategoricalvariablesin fre-quenciesandpercentages.
Comparisonbetweencontinuousandcategoricalbaseline variableswasmadeusingKruskal-Wallisunivariateanalysis, whilecomparisonbetweencategoricalbaselinevariableswas performedusingchi-squareorFisher’sexacttests.
Only those joints showing improvement percentages higherthan50%concomitantlyforallthreeVAS(VASr,VASmv andVASs)weresubjectedtomultivariatelogisticregression analysis,withthechanceofimprovementmeasuredinOdds Ratio(OR)(IC95%).
Significantpvaluewassetat5%.
Ethics
Writteninformedconsentwasobtainedfromallsubjects,and the EthicsCommitteeoftheuniversityapprovedthestudy.
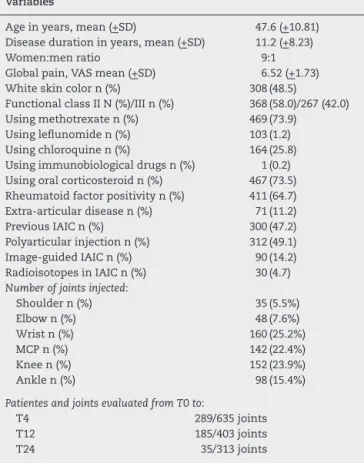
Table1–Demographic,relatedtodiseaseandrelatedto injectiondataofthebaselinesample.
Variables
Ageinyears,mean(+SD) 47.6(+10.81) Diseasedurationinyears,mean(+SD) 11.2(+8.23) Women:menratio 9:1 Globalpain,VASmean(+SD) 6.52(+1.73) Whiteskincolorn(%) 308(48.5)
FunctionalclassIIN(%)/IIIn(%) 368(58.0)/267(42.0) Usingmethotrexaten(%) 469(73.9)
Usingleflunomiden(%) 103(1.2) Usingchloroquinen(%) 164(25.8) Usingimmunobiologicaldrugsn(%) 1(0.2) Usingoralcorticosteroidn(%) 467(73.5) Rheumatoidfactorpositivityn(%) 411(64.7) Extra-articulardiseasen(%) 71(11.2) PreviousIAICn(%) 300(47.2) Polyarticularinjectionn(%) 312(49.1) Image-guidedIAICn(%) 90(14.2) RadioisotopesinIAICn(%) 30(4.7) Numberofjointsinjected:
Shouldern(%) 35(5.5%) Elbown(%) 48(7.6%) Wristn(%) 160(25.2%) MCPn(%) 142(22.4%) Kneen(%) 152(23.9%) Anklen(%) 98(15.4%)
PatientesandjointsevaluatedfromT0to:
T4 289/635joints
T12 185/403joints
T24 35/313joints
153SmPHYPwasprovidedbyInstitutodePesquisas
Energéti-caseNuclearesdoBrasil(IPEN).90YwasimportedbyIPEN fromCisBioScheringInternational(France).Allprocedures thatusedradioisotopeswereperformedunderbiosafetyrules attheNuclearMedicineSector.
Results
Westudied 289patients withRA witha mean age of47.6 years (SD±10.81)and mean disease duration of11.2 years (SD±8.23),48.5%whiteandwomen-to-menratioof9:1,VAS forglobalpain6.52(±1.73).Monoarticularinjectionoccurred in175patients(60.55%);pauciarticularinjectionin68patients (23.53%),andpolyarticularinjectionin46patients(15.92%).Six hundredandthirty-five(635)jointswereinjectedand prospec-tivelystudiedthroughT4;403throughT12,and313through
T24.Table1presentsthedemographicdataanddatarelated
todiseaseandrelatedtoinjectionforthesamplepatients. Baselinevariablesthatdidnotcorrelatestatisticallywith VAS improvement at any of the assessment times were: image-guidedIAIC,useofradioisotopesanduseofcontrast inIAIC.
Univariateanalysis(Kruskal-Wallis)betweenVAS improve-mentsandbaselinevariablesrevealedvariousIAICresponse predictors.
Intermsofmoderateimprovement(50-70%)onpost-IAIC, thestatisticallyassociatedbaselinevariableswere(p<0.05): VASmv,atT4–loweruseofNSAIDsatbaseline;atT24–knee IAIC; VASr,atT4–higherdoseofMTX;atT12–knee IAIC, highertotalTHdoseperpatient;atT24–wristIAIC,longer dis-easeduration,higheruseofNSAIDsatbaseline;VASs,at T12-kneeIAIC,mediumdoseofTHperIAIC,malegender(Table2). Thebestoutcomepredictorsforsignificantimprovement post-IAIC (>70%)were (p<0.05):VASmv, atT4–elbow and kneeIAIC,longerdiseaseduration;atT12–MCPIAIC,higher doseofTHperIAIC,polyarticularinjection,highertotaldose ofTHperpatient,lowermeanage,functionalclassII,useof chloroquine,nouseofleflunomide;nopreviousIAIC;atT24– MCPIAIC,higherTHdoseperIAIC,highertotalTHdoseper patient, polyarticularinjection, lower mean age, non-white skincolor,functionalclassII,moreextra-articulardisease,no useofleflunomide;VASr,atT4–wristandkneeIAIC,higherTH doseperIAIC,useofmethotrexate;atT12–MCPIAIC,higher THdoseperIAIC,higherTHdoseperpatient,non-whiteskin color,functionalclassII,nouseofleflunomide;atT24–MCP
Table2–Associationbetweenimprovementof50%-70%and>70%onVASmv,VASrandVASsassessmentsafterIAIC andthepresenceofbaselinepredictors.
VASmv Improvement(%)
VASr Improvement(%)
VASs
Improvement(%)
T4 T24 T4 T24 T4 T24
Baselinepredictors 50-70 >70 50-70 >70 50-70 >70 50-70 >70 50-70 >70 50-70 >70
IAICinelbow - + - - - + - +
IAICinwrist - - - + + - - - -
-IAICinMCP - - - + - - - + - + - +
IAICinknee - + + - - + - - - +
SizeofTHdoseper IAIC(1/2/3)
- - - +(3) - +(3) - +(3) - +(3) - +(3)
Polyarticularinjection - - - + - - - + - + - +
TotalTHdoseper patient(H/L)
- - - +(H) - - - +(H) - +(H) - +(H)
Age(H/L) - - - +(L) - - -
-Gender(fem/male) - - -
-Skincolor(W/NW) - - - +(NW) - - - +(NW) - - - -Functionalclass(2/3) - - - +(2) - - - +(2) - - - +(2) Extra-articulardisease
(Y/N)
- - - +(Y) - - -
-Diseaseduration(H/L) - +(H) - - - - +(L) - - - - -Useofchloroquine
(Y/N)
- - -
-MTX(H/Ldosage) - - - - +(H) +(H) - - -
-UseofLFU(Y/N) - - - +(Y) - - - +(S) - +(N) - +(N) Totalnumberof
DMARDS(H/L)
- - - +(H) -
-PreviousIAIC(Y/N) - - -
-UseofNSAIDS(Y/N) +(N) - - - +(Y) -
-DoseofOC(H/L) - - - +(H) +(L) - - -
Table3–Associationbetween>50%concomitant improvementonVASmv,VASrandVASspost-IAICand thepresenceofvariablesatbaseline.
Variables T4 T24
OR P OR p
Jointtype(comparedtothe knee)
1.Elbow NS NS 4.4 0.008 2.Wrist 0.59 0.03 NS NS 3.MCP 0.46 0.002 2.75 <0.001 4.Shoulder NS NS NS NS 5.Ankle 0.55 0.03 NS NS Poly-injection(yes/no) 0.26 <0.001 2.37 0.02 Sex(male/female) 2.19 0.008 NS NS Skincolor(non-white/white) 2.47 <0.001 0.55 0.04 Rheumatoidfactor(yes/no) NS NS 0.34 <0.001 Functionalclass(3/2) NS NS 0.42 0.003 Chloroquine(yes/no) 0.61 0.03 0.52 0.03 MTX(yes/no) NS NS 1.90 0.013 Useoforalcorticosteroid NS NS 0.95 0.02 TotalDoseofTH 0.99 <0.001 1.00 0.02
IAIC,Intra-articularinjection withcorticosteroid;VASmv,Visual AnalogueScaleforpaininmovement;VASr,VisualAnalogueScale forpainatrest;VASs,VisualAnalogueScaleforswollen joints; OR,oddsratio;TH,triamcinolonehexacetonide;MTX, methotrex-ate;MCP,metacarpophalangealjoint;NS,nostatisticalsignificancy (p>0.05);Statisticaltest,multivariatelogisticregression.
IAIC,higherTHdoseperIAIC,polyarticularinjection,higher totaldoseofTHperpatient,non-whiteskincolor,functional class2,nouseofleflunomide,lessuseoforalcorticosteroid;
VASs,atT4–elbowandMCPIAIC,higherTHdoseperIAIC, polyarticularinjection,highertotalTHdoseperpatient,no useofleflunomide,lowernumberofDMARDS,NSAIDuse;at T12–MCPIAIC,polyarticularinjection,highertotalTHdose perpatient,nopreviousinjection,lowerdoseoforal cortico-steroids;atT24–elbow,MCPandkneeIAIC,higherTHdose perIAIC,polyarticularinjection,highertotaldoseofTHper patient,functionalclassII,nouseofleflunomide(Table2).
Multivariate logistic regression also showed that some ofthevariables presentedatbaselinewereconsideredIAIC responsepredictors(Table3).
Intheshortterm(T4),theonlyvariablesthatwere predic-torsofbestIAICresponsewere:“malegender”and“non-white skin color”. On the other hand, “wrist, MCP and ankle IAIC”,“dopolyarticularinjection”,“beusingchloroquine”and “highertotaldoseofTHperpatient”werethepredictorsfor theworstIAICresponseintheshortterm.
In the long term (T24), various baseline variables were predictorsofthebestIAICresponse,themostimportantof whichwas“doelbowIAIC”(witha4.4timeshigherchance of success), followed by “do MCP IAIC”, “do polyarticular injection”, “be using MTX” and “higher total dose of TH” perpatient(Table3).Thebaselinevariables associatedwith the worst long-term IAIC response were: “non-white skin color”,“rheumatoidfactor positivity”, “functional classIII”, and“beusingchloroquineandoralcorticosteroid”. Multivari-atelogisticregressiondidnotshowanymedium-term(T12) improvementpredictor.
Only mild and transitory local adverse effects were observed. Post-IAIC inflammatory flare was observed in 37.82%ofthepatients(relatedbythepatientsbutnotobserved bytheblindedobserveratT1).Skinatrophy,skinhypochromic andarticularinstabilitywereobservedin1.9%,15.3%and2.0% ofthepatients,respectively.
Discussion
Thiswasaprospective,non-controlledstudyconductedona cohortofpatientswithestablishedRAreceivingTHIAIC injec-tion,adescriptionofagreatexperienceofourgroup.Though knownasthemosteffectivecorticosteroidforintra-articular use,6–8,10–12weareunawareofothersimilarstudiesinwhich THwasusedasanIAICdrug.
Our group has already published few studies in which RA patients were submitted to TH IAIC injection. Monoar-ticular and polyarticular IAIC effectivenesswas considered superiortosystemicuseofcorticosteroids;10,11anklewas con-sideredthejointwithlowestaccuracyforblindedIAIC;6the useofultrasoundtoguideTHinjectiondidnotincreaseits effectivenessinwristsjoint,12 and theuse ofradioisotopes (Yttrium-90 and Samarium-153-particulate hydroxyapatite) didnotimprovedTH IAICeffectivenesswhencomparedto injectionofTHIAICalone.7,8
UncommonTHdoses,as20mgforMCPjointor80mgfor kneejoint,wereusedinourstudy.TheidealTHdosesforIAIC havenotbeenalreadyestablished,but themostcommonly useddosagesare40mgofTHforlargejointsand10-20mgfor smalltomedium-sizedjoints.6,11,14,18,19Someauthors, how-ever,haveusedoptimizeddosesofTHsomewhatsimilarto ours,6,11,14withouttheoccurrenceofanysignificantadverse effects.
Inourstudy,theuseofradioisotopeswasnotrelatedtoany articularimprovementatanyoftheevaluationtime’s post-IAIC.IncreasedIAICeffectivenesswhenassociatedwiththe useoftheYttrium-90andSamarium-153Hydroxyapatitehas beenquestionedbypreviousstudies.7,8,20,21
Univariateanalysisfoundthatbaselinevariablesas“higher TH doses applied via IAIC and per patient”, “polyarticular injection”and “beusingleflunomide”were associatedwith theworstIAICresponses.PerhapsamoreaggressiveTHdose administeredviaIAICandagreaternumberofjointsinjected areassociatedwithhigherpost-IAICarticularflareand, there-fore,withaclearerperceptionofshort-termaggravation.
OtherstudiesthatevaluateIAICresponsepredictors15,22–25 havebeenalreadypublished,butfewofthemusedTHasthe chosencorticosteroid.22,24
InthestudyconductedbyGreenetal.,15fifty-onepatients, with less than or equalto five joints with synovitis, were treatedwithmethylprednisoloneIAIC.Predictorsofresponse werestudiedbeingtheprimaryendpointacompleteresponse at 12 weeks. Twenty-nine patients (57%) had a complete responseat2weeks.Thebestpredictorofresponseat12and 26weekswasthecompleteresponseat2weeks.15Thepresent studyusedTHratherthanmethylprednisolone;itevaluateda highernumberofpatientsanddidnotstudytherelationship betweenIAICresponsesobtainedatthefirstassessmenttime andthoseobtainedduringsubsequentevaluationtimes.
Ederetal.25evaluatedIAICresponsesintwohundredand twentypatientswithpsoriaticarthritissubmittedto245IAIC. Clinicalfactorsassociatedwithgoodresponseincluded dura-tionofpsoriasis[OddsRatio(OR)1.03]and theuseofMTX oranti-TNFagentsatthe timeofinjection(OR2.68). Injec-tionintolargejoints(OR4.58),elevatedsedimentationrate(OR 15.0)andMIFpolymorphism(OR3.2)werefactorsassociated withrelapse,whereasabsenceofclinicaland/orradiographic damage(OR0.23)anddurationofdisease(OR0.92)reduced riskofrelapse.25Similarlytoourstudy,Ederetal.25also stud-iedagreaternumberofpatientsandfoundthattheuseofMTX wasapredictivefactorofIAICresponse.However,thediseases studiedweredifferent,whichmakeitdifficulttocompareboth setsofresults.
Hetlandet al.23 evaluated betamethasone IAIC response in 160 patients with early RA. One thousand three hun-dredand seventy-three joints (ankles, elbows, knees,MCP, metatarsophalangeal,proximalinterphalangeal(PIP), shoul-ders,wrists)wereinjected(onceorrepeatedinjections)during 2years.Alljoint areashad good 2-yearjointinjection sur-vival,longestforPIPjoints:73.7%.AhigherMRIsynovitisscore ofMCPjointsandanti-CCP-negativitywereassociatedwith poorerjointinjectionsurvival,whereasIgM-RFandC-reactive proteinwerenot.Likeourstudy,IAICinjectionofsmallhand jointwasagoodIAIC-responsepredictor.However,the pres-enceofpositiverheumatoidfactorwasassociatedwithworse IAICresponsesatT24 andrepeated injectionsinthe same jointspacewerenotperformed.ThetimeofonsetofRAand the drug injected were important differences between the studies.
According to our multivariate logistic regression analy-sis,anassociationwithbestIAICresponsewasobservedin onlysevenbaselinevariables.“Beingmale”and“non-white skincolor”wasassociatedwithbestIAICresponsesoverthe shortterm.However,thestrongerassociationswithbestIAIC responseoverthelongterm(24weeks)wereobservedforthe variables“doelbowand MCPIAIC”,“dopolyarticular injec-tion”,“beusingmethotrexate”and“highertotaldoseofTHper patient”.Asinitiallyshownbyunivariateanalysis,“doelbow” and“doMCP”IAICremainedthebaselinevariablespredictive ofbestIAICresponse.Thebenefitofpolyarticularinjection, which implies the use of a higher total dose of corticos-teroidperpatient,wasprovenbypreviouscontrolledstudies usingmethylprednisoloneandTH.11,26Asalreadysuggested byEderetal.,25 “betakingmethotrexate”,givenits disease-modifyingactiononsynovitis,favorapositiveIAICresponsein
comparisontowhenthisdrugisnotinuseinpsoriaticarthritis patients.
Inthepresentstudy“doMCPIAIC”,“dopolyarticular injec-tion”and“highertotaldoseofTHperpatient”werebothworst and best-responsepredictorsoverthe shortand longterm, respectively.Thissuggeststhatpost-IAICarticularflaremay becauseoftheworstresponsesintheshortterm.
Theworstlong-termresponsepredictors–“havinga posi-tiverheumatoidfactorandfunctionalclassIII”and“beusing oralcorticosteroidatthetimeofIAIC”–suggestaworseIAIC response in patients sufferingfrom a moreserious condi-tion.However,“beusingchloroquine”isassociatedwithworse IAIC response over both the shortand long term.Perhaps themechanismofactionofchloroquineinterfereswith intra-articular-administered TH,amicrocrystallinecorticosteroid. But thisassociation hasneverbeen studied,and aspecific prospectivestudyisneededtoclarifythisdoubt.
Oneofthelimitationsofthisstudyisthatanticitruline anti-bodieswerenotmeasuredinoursamplepatients.Asonly0.2% ofthepatientsstudiedwerereceivingimmunobiological ther-apy,predictivevariablesforbestIAICresponseidentifiedin thisstudycannotbeextrapolatedforthosepatientsreceiving thistherapy.
Finally, this isthefirst study toidentify,inRApatients, baselinepredictorsforworstandbestresponsestoIAICwith TH,themostatrophyingcorticosteroidforintra-articularuse. DefiningpredictivefactorsforIAICresponsemayprovetobe extremelyhelpfulinobtainingmoreadequate recommenda-tionsforIAIC,and,therefore,bettertherapeuticmanagement forRApatients.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.HollanderJL,BrownEMJr,JessarRA,BrownCY.Comparative
effectsofCompoundF(17-hydroxycorticosterone)and
cortisoneinjectedlocallyintotherheumatoidarthriticjoint.
AnnRheumDis.1951;10:473–6.
2.LeeDM,WeinblattME.Rheumatoidarthritis.Lancet.
2001;358:903–11.
3.FiresteinGS.Evolvingconceptsofrheumatoidarthritis.
Nature.2003;423:356–61.
4.BartokB,FiresteinGS.Fibroblast-likesynoviocytes:key
effectorcellsinrheumatoidarthritis.ImmunolRev[Review].
2010;233:233–55.
5.NamJL,WinthropKL,vanVollenhovenRF,PavelkaK,Valesini
G,HensorEM,etal.Currentevidenceforthemanagementof
rheumatoidarthritiswithbiologicaldisease-modifying
antirheumaticdrugs:asystematicliteraturereviewinforming
theEULARrecommendationsforthemanagementofRA.Ann
RheumDis.2010;69:976–86.
6.LopesRV,FurtadoRN,ParmigianiL,RosenfeldA,Fernandes
AR,NatourJ.Accuracyofintra-articularinjectionsin
peripheraljointsperformedblindlyinpatientswith
rheumatoidarthritis.Rheumatology(Oxford).2008;47:1792–4.
7.SantosMF,FurtadoRN,KonaiMS,CastiglioniML,Marchetti
RR,NatourJ.Effectivenessofradiationsynovectomywith
arthritispatientswithkneesynovitis:acontrolled
randomizeddouble-blindtrial.Clinics(SãoPaulo).
2009;64:1187–93.
8. DosSantosMF,FurtadoRN,KonaiMS,CastiglioniML,
MarchettiRR,SilvaCP,etal.Effectivenessofradiation
synovectomywithYttrium-90andSamarium-153particulate
hydroxyapatiteinrheumatoidarthritispatientswithknee
synovitis:acontrolled,randomized,double-blindedtrial.
ClinicalRheumatol.2011;30:77–85.
9. ParmigianiL,FurtadoRN,LopesRV,RibeiroLH,NatourJ.Joint
lavageassociatedwithtriamcinolonehexacetonideinjection
inkneeosteoarthritis:arandomizeddouble-blindcontrolled
study.ClinicalRheumatol.2010;29:1311–5.
10.KonaiMS,VilarFurtadoRN,DosSantosMF,NatourJ.
Monoarticularcorticosteroidinjectionversussystemic
administrationinthetreatmentofrheumatoidarthritis
patients:arandomizeddouble-blindcontrolledstudy.Clin
ExpRheumatol.2009;27:214–21.
11.FurtadoRN,OliveiraLM,NatourJ.Polyarticularcorticosteroid
injectionversussystemicadministrationintreatmentof
rheumatoidarthritispatients:arandomizedcontrolledstudy.
JRheumatol.2005;32:1691–8.
12.LuzKR,FurtadoRN,NunesCC,RosenfeldA,FernandesAR,
NatourJ.Ultrasound-guidedintra-articularinjectionsinthe
wristinpatientswithrheumatoidarthritis:adouble-blind,
randomisedcontrolledstudy.AnnRheumDis.
2008;67:1198–200.
13.DerendorfH,MollmannH,GrunerA,HaackD,GyselbyG.
Pharmacokineticsandpharmacodynamicsofglucocorticoid
suspensionsafterintra-articularadministration.Clin
PharmacolTher.1986;39:313–7.
14.GrayRG,GottliebNL.Intra-articularcorticosteroids.An
updatedassessment.ClinOrthopRelatRes.1983:235–63.
15.GreenM,Marzo-OrtegaH,WakefieldRJ,AstinP,ProudmanS,
ConaghanPG,etal.Predictorsofoutcomeinpatientswith
oligoarthritis:resultsofaprotocolofintraarticular
corticosteroidstoallclinicallyactivejoints.ArthritisRheum.
2001;44:1177–83.
16.ArnettFC,EdworthySM,BlochDA,McShaneDJ,FriesJF,
CooperNS,etal.TheAmericanRheumatismAssociation
1987revisedcriteriafortheclassificationofrheumatoid
arthritis.ArthritisRheum.1988;31:315–24.
17.HochbergMC,ChangRW,DwoshI,LindseyS,PincusT,Wolfe
F.TheAmericanCollegeofRheumatology1991revised
criteriafortheclassificationofglobalfunctionalstatusin
rheumatoidarthritis.ArthritisRheum.1992;35:498–502.
18.CanosoJJ.Aspirationandinjectionofjointsandperiarticular tissues(includingintra-articularandintralesionaltherapy). 4thed.In:HochbergMCSA,SmolenJS,WeinblattME, WeismanMH,editors,editor:Mosby:Elsevier;2007. 19.CanosoJJ.TherapeuticInjectionsofJointsandSoftTissues.
13thed.In:KlippelJHSH,CroffordLJ,WhitePH,editor: Springer;2008.
20.Intra-articularradioactiveyttriumandtriamcinolone
hexacetonide:aninconclusive,trial,Arthritisand
RheumatismCouncilMulticentreRadiosynoviorthesisTrial,
Group,AnnRheum,Dis.1984;43:620–3.
21.JahangierZN,JacobsJW,LafeberFP,MoolenburghJD,Swen
WA,BruynGA,etal.Isradiationsynovectomyforarthritisof
thekneemoreeffectivethanintraarticulartreatmentwith
glucocorticoids?Resultsofaneighteen-month,randomized,
double-blind,placebo-controlled,crossovertrial.Arthritis
Rheum.2005;52:3391–402.
22.LanniS,BertaminoM,ConsolaroA,PistorioA,
Magni-ManzoniS,GalassoR,etal.Outcomeandpredicting
factorsofsingleandmultipleintra-articularcorticosteroid
injectionsinchildrenwithjuvenileidiopathicarthritis.
Rheumatology(Oxford).2011;50:1627–34.
23.HetlandML,OstergaardM,EjbjergB,JacobsenS,
Stengaard-PedersenK,JunkerP,etal.Short-andlong-term
efficacyofintra-articularinjectionswithbetamethasoneas
partofatreat-to-targetstrategyinearlyrheumatoidarthritis:
impactofjointarea,repeatedinjections,MRIfindings,
anti-CCP,IgM-RFandCRP.AnnRheumDis.2012;71:851–6.
24.RavelliA,ManzoniSM,ViolaS,PistorioA,RupertoN,Martini
A.Factorsaffectingtheefficacyofintraarticular
corticosteroidinjectionofkneesinjuvenileidiopathic
arthritis.TheJRheumatol.2001;28:2100–2.
25.EderL,ChandranV,UengJ,BhellaS,LeeKA,RahmanP,etal.
Predictorsofresponsetointra-articularsteroidinjectionin
psoriaticarthritis.Rheumatology(Oxford).2010;49:
1367–73.
26.ProudmanSM,ConaghanPG,RichardsonC,GriffithsB,Green
MJ,McGonagleD,etal.Treatmentofpoor-prognosisearly
rheumatoidarthritis.Arandomizedstudyoftreatmentwith
methotrexate,cyclosporinA,andintraarticular
corticosteroidscomparedwithsulfasalazinealone.Arthritis