www.jped.com.br
ORIGINAL
ARTICLE
Factors
influencing
excessive
daytime
sleepiness
in
adolescents
夽
Thiago
de
Souza
Vilela,
Lia
Rita
Azeredo
Bittencourt,
Sergio
Tufik,
Gustavo
Antonio
Moreira
∗UniversidadeFederaldeSãoPaulo(UNIFESP),SãoPaulo,SP,Brazil
Received9December2014;accepted27May2015 Availableonline10December2015
KEYWORDS
Adolescents; Sleep;
Sleepdeprivation; Sleepiness
Abstract
Objective: Sleep deprivationinadolescentshas latelybecomea healthissue thattends to increase withhigherstressprevalence, extenuatingroutines,andnewtechnologicaldevices thatimpairadolescents’bedtime.Therefore,thisstudyaimedtoassesstheexcessivesleepiness frequencyandthefactorsthatmightbeassociatedtoitinthispopulation.
Methods: Thecross-sectionalstudyanalyzed531adolescentsaged10---18yearsoldfromtwo privateschoolsandonepublicschool.Fivequestionnaireswereapplied:theCleveland Adoles-centSleepinessQuestionnaire;theSleepDisturbanceScaleforChildren;theBrazilianEconomic ClassificationCriteria;theGeneralHealthandSexualMaturationQuestionnaire;andthe Physi-calActivityQuestionnaire.Thestatisticalanalyseswerebasedoncomparisonsbetweenschools andsleepinessandnon-sleepinessgroups,usinglinearcorrelationandlogisticregression. Results: Sleepdeprivationwaspresentin39%oftheadolescents;sleepdeficitwashigherin privateschooladolescents(p<0.001),andtherewasapositivecorrelationbetweenageand sleepdeficit(p<0.001;r=0.337).Logisticregressionshowedthatolderage(p=0.002;PR:1.21 [CI:1.07---1.36])andhigherscorelevelforsleephyperhidrosisinthesleepdisturbancescale (p=0.02;PR:1.16[CI:1.02---1.32])wereriskfactorsforworsedegreeofsleepiness.
Conclusions: Sleep deficitappears to beareality among adolescents; theresultssuggest a higherprevalenceinstudentsfromprivateschools.Sleepdeprivationisassociatedwitholder ageinadolescentsandpossiblepresenceofsleepdisorders,suchassleephyperhidrosis. ©2015SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Allrightsreserved.
夽 Pleasecitethisarticleas:VilelaTS,BittencourtLR,TufikS,MoreiraGA.Factorsinfluencingexcessivedaytimesleepinessinadolescents. JPediatr(RioJ).2016;92:149---55.
∗Correspondingauthor.
E-mail:[email protected](G.A.Moreira).
http://dx.doi.org/10.1016/j.jped.2015.05.006
PALAVRAS-CHAVE
Adolescentes; Sono;
Privac¸ãodesono; Sonolência
Fatoresqueinfluenciamnasonolênciaexcessivadiurnaemadolescentes
Resumo
Objetivo: Aprivac¸ãodesononaadolescênciaéumimportanteproblemadesaúdenaatualidade esótendeaseagravarcomoaumentodoestresse,darotinaextenuanteedoadventodenovos aparelhostecnológicosqueparecemrefletirnegativamentenoiníciodosonoemadolescentes. Oestudoobjetivaavaliarafrequênciadasonolênciaexcessivae quaisfatores podemestar associadosàelanestapopulac¸ão.
Métodos: Oestudotransversalavaliou531adolescentesde10a18anosemduasescolasde ensinoprivadoeumadeensinopúblico,aplicandoparacadaadolescentecincoquestionários: ClevelandAdolescentSleepinessQuestionnaire;SleepDisturbanceScaleforChildren;Critério de Classificac¸ão Econômica Brasil; Questionário geralde saúde e maturac¸ão sexual; Ques-tionáriodeatividadefísica.Realizou-secomparac¸õesentreasescolaseentregruposcome semsonolênciapormeiodecorrelac¸ãolineareregressãologística.
Resultados: Observou-se privac¸ãode sono em 39% dos adolescentes, débitode sonomaior paraescolaresdoensinoprivado(p<0,001)ecorrelac¸ãopositivaentreidadeedébitodosono (p<0,001;r=0,337).Naregressãologística,apontou-secomofatoresparapiorgraude sonolên-ciamaiorfaixaetáriadosescolares(p=0,002;RP:1,21[IC:1,07-1,36])emaiorescorenavariável hiperidrosedosonodoquestionáriodedistúrbiosdosono(p=0,02;RP:1,16[IC:1,02-1,32]). Conclusões: Conclui-se que o déficit de sono é uma realidade na populac¸ão estudada, apresentando-se pior em escolaresdo ensino privado. A privac¸ão de sonoestá relacionada comamaiorfaixaetáriadosadolescentesepossívelpresenc¸adedistúrbiosdosono,comoa hiperidrosedosono.
©2015SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Todososdireitos reservados.
Introduction
Sleep is extremely important for appropriate physical growth,emotional stability,behavior, andmaintenanceof cognitive function in adolescents.1,2 Physiological studies
haveshownthatadequatesleepisalsoimportantfor mem-oryconsolidation,whichhasseriousimplicationsonschool successinthisagegroup.2,3Agoodqualitynightsleepwill
reflectinbetterschoolperformanceandincreased motiva-tiontostudy.3 Severalstudiessuggestthatthispopulation
requiresanaverageofeighttoninehoursofsleeppernight toadequatelyperform everydayactivities and absorbthe physicalandmentalbenefitsofsleep.4,5
Although this is the goal for a good-quality sleep, it is knownthat adolescents have been sleeping for shorter periods than necessary.6 The upgrading and launching of
increasingly more attractive videogames and virtual real-itysimulatorsandthe broadpresence ofInternet through chatgroups,andsocialnetworksareaggravatingfactorsfor inadequatesleep.7 The presenceof TVs, videogame
con-soles,andcomputersinbedrooms7---9arerelatedtogreater
sleepdeprivation. With the advent and popularization of handhelddevices,morestudiesshouldbeperformedto eval-uatetheireffectsonsleep,asadolescentshave thehabit of takingthem to bed at bedtime, consequently delaying sleeponset. Moreover, the current hectic lifestyle, espe-ciallyinlargecities,negativelyaffectsadolescents,making themvictimsofanxiety,aggression,stress,socialandschool burdens,withpossibledamagetoanadequatesleep.2,10
Sleepdeprivation,morethanpreviouslythought,isnot restrictedtopsychosocialalterations.Recently,associations
were observed between sleepiness and obesity.11
Over-weight adolescents appear to have a shorter and more disturbedsleep,11,12andoverweightisalsoariskfactorfor
sleep-disorderedbreathing,suchasobstructivesleepapnea syndrome(OSAS).13
Whatisknownsofaristhatbothinternalfactors,suchas sexualmaturity,age,gender,andobesity,aswellasexternal factors,suchasschoolshift,useoftechnologyanddruguse, caninfluencethesleep.5,7However,Brazilstilllackslarge
studiesthatdemonstratethisscenariointhecountry. Thus,toevaluatesleepinessinthispopulation,an alter-native istheuseofquestionnaires.Oneof themost often used,thePediatricDaytimeSleepinessScale(PDSS),14shows
as limitation a restrict age group for adolescents. The Modified Epworth Sleepiness Scale (ESS),15 in turn, is an
adaptationoftheEpworthSleepinessScale,containingfew questions in its evaluation and alsorestricted age group. Thus,asitaddressesquestionsfromfourareas(sleepinessat school,alertinschool,sleepinessintheevening,and sleepi-nessduringtransport),theClevelandAdolescentSleepiness Questionnaire(CASQ)16 isone ofthemost complete
ques-tionnairestoassessexcessivesleepinessinthatpopulation, even though it does not have acutoff point for the clas-sificationofpresenceornotofsleepiness.Although itisa newquestionnairetoassesssleepiness,otherquestionnaires commonly appliedtochildrenandadolescentsareusedin smallerpopulationsandhavelimitednationalapplication.
Methods
Thiswasaprospectivestudy andtheassessmentwas per-formedusingspecificquestionnairesappliedtoapopulation of 545 adolescents aged 10---18 years from three schools (two private andone public)in thecity of São Paulo and adjacenttowns, chosenbyconvenienceduringthesecond half of 2013. For inclusion, the adolescents were invited toparticipateinthestudythroughanexplanatorylecture. Adolescentsagedbetween10and18yearsoldfromschools whoagreedtoparticipatewererecruited.Participantshad to have the informed consent form and the adolescent termofagreementdulysigned.Adolescentswhohadsome degreeofmentaldeficitorother disabilitythatprevented themfromappropriatelyansweringthequestionnaireswere excluded.Thosewhowerechronicusersofdrugsthatcould influence the sleep---wake cycle were also excluded. The study wasapproved bythe Research EthicsCommitteeof UniversidadeFederaldeSãoPauloin2013,under registra-tionnumber15925613.4.0000.5505.
Thestudiedvariableswereage,gender,degreeofsexual maturation,ethnicity,bodymassindex(BMI),schoolshift, economic status, physical inactivity, presence of chronic diseasesandcontinuoususeofdrugs,economicstatus, pres-enceofexcessivesleepiness,sleepdisorders,andhoursof sleep.
The assessment of these variables was carried out through five questionnaires, distributed by a single researcher and filled out at home. One of them was the Portuguese (Brazil) version of the Cleveland Adolescent SleepinessQuestionnaire(CASQ)16 containing16questions,
whichassessesthesleepinessdegreeofadolescentsandits limit values are 16---80 points, without a cutoff point for theclassificationofthepresenceorabsenceofsleepiness. The adaptation of the CASQ to the Portuguese language was performed after the authorization from the original authorof the study and twoindividuals, fluent in English and Portuguese, translated it independently. As the first versions were obtained, the next step was to translate thembackintoEnglish,whichwasperformedbytwonative Englishspeakers,bothbilingual.Thetwotranslationswere assessedtogetherandchangesweremadeuntilaconsensus wasreached, withonly oneversion remaining.Then, this translatedversionwasanalyzedbyexpertsinthefieldand changesweremadeagaintoachieveasingledecision.This second versionwastested with15 adolescentswho,after readingthequestions,explainedtheirunderstandingofthe questionsandwhethertheyhadinterpretationdoubts.The 16questionswereunderstoodbyatleast80%ofthe adoles-cents.The questionsthat ledtocomprehensiondoubtsby over10%oftheadolescentswererewritten,resultinginthe thirdversionofthetranslation,definedasthefinalversion. Anotherquestionnairewasthevalidatedversionintothe Brazilian Portuguese (Ferreira et al.)17 of the Sleep
Dis-turbanceScalefortheChildren(SDSC),developedbyBruni et al.18 This questionnaire evaluates, in 26 questions, six
groupsoffrequentsleepdisordersinchildren(disordersof initiating and maintaining sleep,sleep-disordered breath-ing,disordersof arousal,sleep---wake transitiondisorders, disorders of excessive somnolence, sleep hyperhidrosis). There are no cutoff points for the classification, and
valuescan vary from26 to 130 in total. One more ques-tionwasaddedtothequestionnaireabouthoursofsleepon theweekendforthecalculationofsleepdeficit.
The socioeconomic status questionnaire Brazilian Eco-nomic Classification Criteria, formulated by the Brazilian AssociationofResearchCompanies(Associac¸ãoBrasileirade Empresas de Pesquisa), which classifies the population in socialclassesfromAtoEaccordingtotheexistingitemsat homeandeducationalleveloftheheadoffamily,wasalso appliedtotheadolescents.
Ageneralquestionnaire evaluatedtheremaining varia-bles: the degree of sexual maturation was assessed by self-report,accordingtothedrawingsofTanner’s matura-tionstagesforgenital,breast,andhairdevelopment.19Two
versionswereused,accordingtogender.Nutritional assess-mentwasaccomplishedusingthemorerecentself-reported measuresofweightandheighttocalculatebodymassindex, andthediagnosisofthenutritionalstatuswasbasedonBMI Z-scoreaccordingtothegrowthcurvesoftheWorldHealth Organization.20ObesitywasdefinedastheBMIZ-score>two
standarddeviations(>+2SD).
Thephysicalactivityquestionnaireincludedthree ques-tionsaboutthefrequencyofphysicalactivityandsedentary activities developed by the adolescents, adapted to the Brazilianrealityfromtheoriginalquestionnairedeveloped bythePediatricSleepCenterforSleepDisordersofthe Uni-versityof Chicago.21 The questionnaireclassifies asactive
studentswhoperform morethan 30min of exercisemore frequentlythanthreetimesaweek.Attheend,theyalso answeredtwoquestionsinthisquestionnaireregardingthe presenceofchronicdiseasesanduseofcontinuous medica-tion.
Results
Thestudyincludedatotalof545questionnaires,ofwhich 14 were delivered unfilled, resulting in 531 valid ques-tionnaires.Ofthese,368students(69%)fullyansweredall questionnaires.An activesearchwascarriedoutwith163 adolescentswithincomplete questionnairestohave them completed, but it was unsuccessful. However,the usable data were accepted, as long as they did not impair the study.
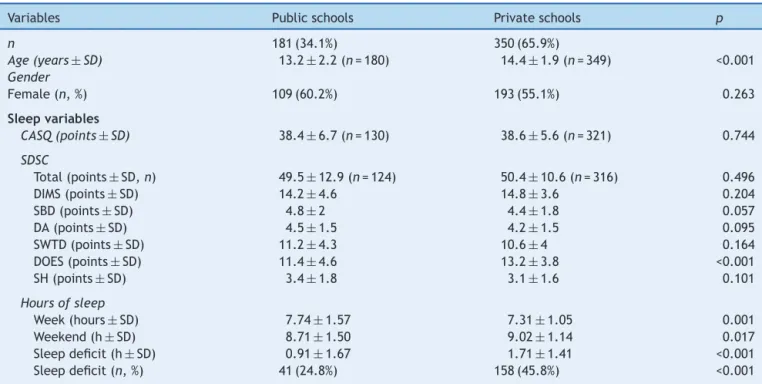
Table1showsthemostimportantdemographicandsleep characteristicsoftheassessedsampleofadolescents, com-paringstudentsfromprivateandpublicschools.Thethree schoolsweredividedintotwogroups,withregardtoprivate educationand public education.Among the assessed stu-dents,themajority(65.9%)camefromprivateschools.The meanageofthepopulation was13.9±2.1years(n=529), andstudentsofprivateschoolshadahighermeanagethan thosefrompublicschool(p<0.001).The sampleconsisted mostlyoffemales(302;56.9%),withnodifferencein gen-derdistribution betweenprivate andpublic schools.With regardtosocio-economicalclass,thedifferencewas signif-icant(p<0.001),withapredominanceofclassAinprivate schoolsandclassesBandCinpublicschools.Sexual matu-rityshowedsignificant differences(p<0.001),whichwere compatiblewiththeagedifferenceofthegroups,andthe dailyuseofmedication wassignificantlymore frequentin theprivateschoolstudents(p=0.003).
FortheCASQsleepiness questionnaire,themeanvalue obtained (n=451) was 38.6±6. There was no difference betweenstudentsfrompublicandprivateschools:themean inthepublicschoolwas38.4±6.7andintheprivateschool, 38.6±5.6(Table1).
As for the SDSC score, the mean of the total popula-tion(n=440)was50.1±11.3.Consideringonlythestudents frompublicschools,themeanwas49.5±13,andofprivate schools,50.4±10.6andthedifferencewasnotstatistically significant. However, a higher prevalence of disorders of excessivesomnolence(SDSCscore)wasobservedinstudents fromprivateschools(p<0.001).
Students frompublic schools had longer time of sleep duringtheweekthantheirprivateschoolpeers(p=0.001), and the latter had a longer time of sleep on weekends (p=0.017).Asforthesleeppattern,sleepdeprivationwas consideredwhensleepdeficitwas≥2h.Thus,199 adoles-cents(39%)reportedameanoftwoormorehoursofsleepon weekendswhencomparedwiththemeannumberofhours of sleeponweekdays. The sleepdeficit for studentsfrom thepublicschoolswas0.91hversus1.71hforprivateschool students(p<0.001),andthepercentageof sleep-deprived privateschoolstudentswashigherthatobservedinpublic schoolstudents(45.8%vs.24.8%;p<0.001).
Therewasa statisticallysignificantpositivecorrelation between sleep deficit and age (p<0.001), of moderate degree(r=0.337),showingagradualincreaseinsleepdeficit asageincreased(Fig.1).Whenconsideringage,thevalue ofCASQincreasedgraduallywithage:36±5.7for 10-year-oldsand41.3±6.2for17-year-olds, showingacorrelation betweenthevariablesageandtheCASQvalue(p<0.001)of milddegree(r=0.244).Thesampleofadolescentsaged18 yearswasnotshownasitwasnotrepresentative(n=8).
Toassesssleepiness,theauthorschosetousetheCASQ asthedependentvariable.Themeanscoreachievedbythe studentsin CASQ, 38points,wasusedasthe cutoffvalue for thedivisionbetweengroups withpresenceor absence ofsleepiness.Numericalvariableswerecomparedwiththe
Table1 Characteristicsofthesampleofadolescentsaccordingtotheschooltype.
Variables Publicschools Privateschools p
n 181(34.1%) 350(65.9%)
Age(years±SD) 13.2±2.2(n=180) 14.4±1.9(n=349) <0.001 Gender
Female(n,%) 109(60.2%) 193(55.1%) 0.263
Sleepvariables
CASQ(points±SD) 38.4±6.7(n=130) 38.6±5.6(n=321) 0.744
SDSC
Total(points±SD,n) 49.5±12.9(n=124) 50.4±10.6(n=316) 0.496
DIMS(points±SD) 14.2±4.6 14.8±3.6 0.204
SBD(points±SD) 4.8±2 4.4±1.8 0.057
DA(points±SD) 4.5±1.5 4.2±1.5 0.095
SWTD(points±SD) 11.2±4.3 10.6±4 0.164
DOES(points±SD) 11.4±4.6 13.2±3.8 <0.001
SH(points±SD) 3.4±1.8 3.1±1.6 0.101
Hoursofsleep
Week(hours±SD) 7.74±1.57 7.31±1.05 0.001
Weekend(h±SD) 8.71±1.50 9.02±1.14 0.017
Sleepdeficit(h±SD) 0.91±1.67 1.71±1.41 <0.001
Sleepdeficit(n,%) 41(24.8%) 158(45.8%) <0.001
17 16 15 14 13 12 11 10
Age (years)
CASQ 36 37.6 37 36.8 37.7 40.2 40.6 41.3
SLEEP DEFICIT 0.25 0.66 0.84 1.08 1.86 2.02 1.96 1.96
0 0.5 1 1.5 2 2.5
32 34 36 38 40 42
Sleep deficit (h)
C
ASQ*
*CASQ (Cleveland adolescent sleepiness questionnaire)
Figure1 Sleepinessvs.age.
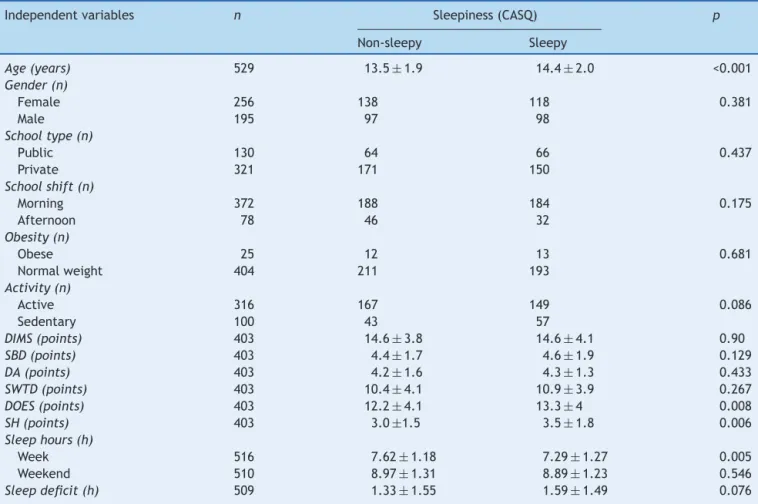
sixvariablesthatcomposetheSDSCquestionnaire,in addi-tiontothehoursofsleepduringtheweek,hoursofsleepon weekends, sleepdeficit, and age.There wasa significant association between higher values of the SDSC question-nairescorefordisordersofexcessivesomnolence(p=0.008) andsleephyperhidrosis(p=0.006),increasedsleep restric-tionduringthe week(p=0.005),and olderage (p<0.001) in the group with excessive sleepiness. The assessed
categoricalvariableswereschool(publicvs.private),school shift, gender, obesity and physical activity. None of the variables showed significant difference between the two groups(Table2).Thepresenceofchronicdiseases(p=0.34) wasnotsignificant.
When the correlation between the different variables and sleepiness (CASQ) was assessed, there was a posi-tive correlation with disorders of excessive somnolence
Table2 Comparisonofthesampleaccordingtosleepiness(CASQ).
Independentvariables n Sleepiness(CASQ) p
Non-sleepy Sleepy
Age(years) 529 13.5±1.9 14.4±2.0 <0.001 Gender(n)
Female 256 138 118 0.381
Male 195 97 98
Schooltype(n)
Public 130 64 66 0.437
Private 321 171 150
Schoolshift(n)
Morning 372 188 184 0.175
Afternoon 78 46 32
Obesity(n)
Obese 25 12 13 0.681
Normalweight 404 211 193
Activity(n)
Active 316 167 149 0.086
Sedentary 100 43 57
DIMS(points) 403 14.6±3.8 14.6±4.1 0.90
SBD(points) 403 4.4±1.7 4.6±1.9 0.129
DA(points) 403 4.2±1.6 4.3±1.3 0.433
SWTD(points) 403 10.4±4.1 10.9±3.9 0.267
DOES(points) 403 12.2±4.1 13.3±4 0.008
SH(points) 403 3.0±1.5 3.5±1.8 0.006
Sleephours(h)
Week 516 7.62±1.18 7.29±1.27 0.005
Weekend 510 8.97±1.31 8.89±1.23 0.546
Sleepdeficit(h) 509 1.33±1.55 1.59±1.49 0.076
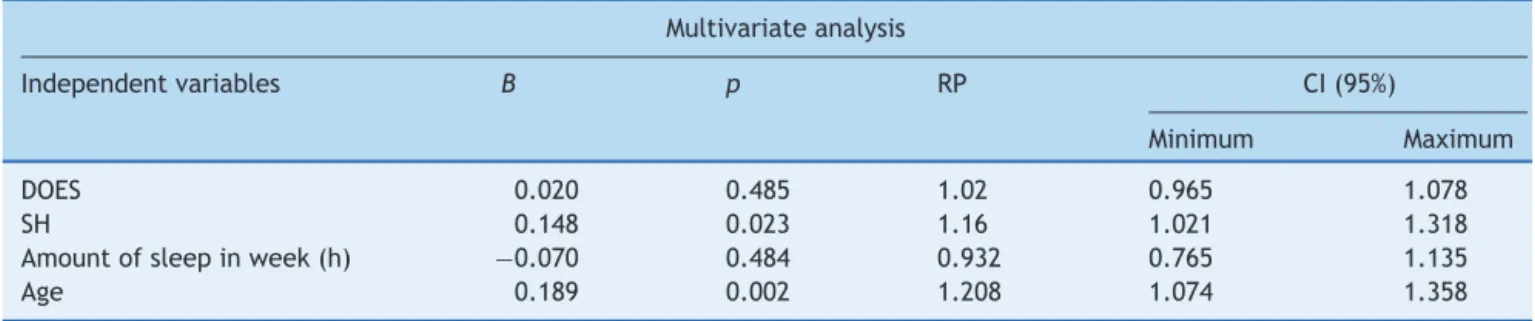
Table3 FactorsassociatedwithsleepinessinadolescentsinthecityofSãoPaulo,Brazil. Multivariateanalysis
Independentvariables B p RP CI(95%)
Minimum Maximum
DOES 0.020 0.485 1.02 0.965 1.078
SH 0.148 0.023 1.16 1.021 1.318
Amountofsleepinweek(h) −0.070 0.484 0.932 0.765 1.135
Age 0.189 0.002 1.208 1.074 1.358
DOES,disordersofexcessivesomnolence;SH,sleephyperhidrosis.
(r=0.25,p<0.001),sleephyperhidrosis(r=0.23,p<0.001), age(r=0.24,p<0.001)andsleepdeficit(r=0.11,p=0.02). There wasa negativecorrelation between sleepinessand theamount of sleepin hours during theweek (r=−0.21,
p<0.001)andtherewasnocorrelationbetweensleepiness andamountofsleeponweekends(r=−0,08,p=0.10).
Multivariatelogisticregressionwasperformedto investi-gatethefactorsassociatedwithsleepinessinadolescents. Statisticallysignificantvaluesindicatetheolderageof stu-dents and higher scores on the SDSC sleep hyperhidrosis variableasfactorsforworsedegreeofexcessivesleepiness (Table3).
Discussion
Basedonthe present results,age andsleephyperhidrosis hadastatisticallysignificanteffectondaytimesleepinessin thestudiedadolescentpopulation.The valuesfoundwhen applyingtheCASQinBrazilianadolescents(38.6±6)showed tobeslightlyhigherthanthosefoundbySpilsburyetal.16in
theUnitedStatesatthequestionnairevalidation(35.2±11) and in 314 Indian adolescents, in whom the mean value obtainedwas36±9.22
Analarmingfindingwasthat39%oftheseadolescentshad asleepdeficitgreaterthan2hand,therefore,weresubject to numerous complications of sleep deprivation.23 These
sleepdeprivation valuesfollowedthetrend ofPortuguese data,24 in which74% of theassessedindividuals sleptless
than8honweekdaysand33%didsoonweekends.Thereis alsoadirectassociationbetweenageanddaytimesleepiness (Fig.1).Theauthorsspeculatethat,withincreasingage,the adolescents,despite the littlesleep, prioritizesocial and leisureactivities,inadditiontolosingprecioustimeduring displacementintheurbanenvironment.7,25Also,thefinding
ofincreasedsleepdeficitinprivateschoolstudentsappears tobeassociatedwiththefactthattheprivateschool sam-plehave studentsmostlyattendingthemorningshift.The importanceofsleepdeprivationhasbeendemonstratednot only in the West,26 but also in recent data from China,27
whereaninterventiontookplaceinaprimaryschoolwith adelay in the start of school activitiesof 30 and 60min, resultinginbetterperformanceofstudents.
Another associated factor, sleep hyperhidrosis, is a complaint that interferes with the quality of sleep, thus contributingto sleepiness. It can be described in a large numberofdifferentialdiagnoses,frominfectious diseases toneuroendocrinedisorders,28butitisalsoaverycommon
complaint inpatients withOSAS28,29 and other respiratory
diseasesinchildhood.30
Thestudyhaslimitationsduetotheabsenceofsample size calculation, but thelinearcorrelations between age, excessivesleepiness,andsleepdeficit(CASQ)withasample of450,two-tailedpof5%,andr=0.37,evidencedapower of99%.Theunbalancedsamplebetweenthepublicand pri-vateschoolsalsocreatesparadoxesinthefindings,andmay notrepresentthegeneralBrazilian adolescentpopulation. Thesamplesizewithoutsufficientstatisticalpowertofind differencescanjustifythefactthatsomeassociationswere notstatisticallysignificant.Thehorizontalstudydesignalso doesnotallowforthedeterminationofthecause-and-effect association, but wasenough toshow some factors associ-ated with sleepiness in adolescents.Another point is the useofquestionnaires,whichinadditiontonotbeingas sen-sitiveasinterviews,hasthedisadvantageoflossesanddoes not consider the individuality of the population to which they areapplied.The CASQ, for instance, was developed forEnglish-speakingadolescentswhostudyfull-time. How-ever, this information is notas relevant,considering that over80%ofthepresentstudysamplestudiedinthemorning andwakeupearly.Thechoiceoftranslatingaquestionnaire andusingitforthefirsttimeinthecountrycanalsobea limitation;however,theCASQisoneofthebest question-nairestoassesssleepinessandtheonlyonethatcanaddress theentireagegroupofthisstudy.
The study conclusion is that excessive sleepiness is related to increasing age; an association with the pres-enceofsleephyperhidrosiswasalsoobserved.Sleepdeficit wasveryfrequentintheassessedpopulationofadolescents and, therefore, the effort to develop a better quality of sleepshouldbeprimarilyfocusedonbettersleephygiene, thuspreventingthispopulationfromsufferingthedamages causedbysleepdeprivationfromanearlyage.Future stud-iesshouldfocusoninterventionstrategiestoreducesleep deprivation.
Funding
Fundac¸ão de Amparo à Pesquisa do Estado de São Paulo (FAPESP) --- Thiago S. Vilela (Process 2012/20503-4).Associac¸ão Fundo de Incentivo à Pesquisa (AFIP) --- no processnumber.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
The authors would like toexpress their sincere apprecia-tion to the funders of the study, which allowed it to be performed.Additionally,theywouldliketothankthethree schoolsinvolvedinthisstudy,whoseparticipationwas fun-damental from the sample selection to the inclusion of thestudyintheirextracurricularactivities,encouragingin theirstudents, froman early age,an interestinscientific research. The authors would also like to thank the tea-chers,coordinatorsandprincipals,whogavetheaccessto thetargetpopulation,andespeciallytoalladolescentswho spontaneously answered thequestionnaires,thus allowing thestudytobecarriedout.
References
1.BeebeDW.Cognitive,behavioral,andfunctionalconsequences ofinadequatesleepinchildrenandadolescents.PediatrClinN Am.2011;58:649---65.
2.MeldrumRC,RestivoE.Thebehavioralandhealthconsequences ofsleep deprivationamongUS highschoolstudents:relative deprivationmatters.PrevMed.2014;63:24---8.
3.Allen-GomesA,TavaresJ,AzevedoMH.Sleepandacademic per-formanceinundergraduates:a multimeasure,multipredictor approach.ChronobiolInt.2011;28:786---801.
4.DewaldJF,MeijerAM,OortFJ,KerkhofGA,BögelsSM.The influ-enceofsleepquality,sleepdurationandsleepinessonschool performance in children and adolescents: a meta-analytic review.SleepMedRev.2010;14:179---89.
5.Owens J, Adolescent Sleep Working Group Committee on Adolescence. Insufficient sleep in adolescents and young adults: an update on causes and consequences. Pediatrics. 2014;134:e921---32.
6.MatriccianiL,OldsT,PetkovJ.Insearchoflostsleep:secular trendsinthesleeptimeofschool-agedchildrenand adoles-cents.SleepMedRev.2012;16:203---11.
7.CalamaroCJ,MasonTB,RatcliffeSJ.Adolescentslivingthe24/7 lifestyle:effectsofcaffeineandtechnologyonsleepduration anddaytimefunctioning.Pediatrics.2009;123:1005---10. 8.Cain N, Gradisar M. Electronic media use and sleep in
school-aged children and adolescents: a review. Sleep Med. 2010;11:735---42.
9.VandenBulckJ.Televisionviewing,computergameplaying, andinternetuseandself-reportedtimetobedandtimeoutof bedinsecondary-schoolchildren.Sleep.2004;27:101---4. 10.Shochat T, Cohen-Zion M, Tzischinsky O. Functional
conse-quences of inadequate sleep in adolescents: a systematic review.SleepMedRev.2014;18:75---87.
11.HartCN,CairnsA,JelalianE.Sleepandobesityinchildrenand adolescents.PediatrClinNorthAm.2011;58:715---33.
12.Mitchell JA, Rodriguez D, Schmitz KH, Audrain-McGovern J. Sleep duration and adolescent obesity. Pediatrics. 2013;131:e1428---34.
13.Bhattacharjee R, Kim J, Jheirandish-Gozal L, Gozal D. Obe-sity and obstructive sleep apnea syndrome in children: a tale of inflammatory cascades. Pediatr Pulmonol. 2011;46: 313---23.
14.Drake C, Nickel C, Burduvali E, Roth T, Jefferson C,Pietro B. The pediatric daytime sleepiness scale (PDSS): sleep habitsand schooloutcomesinmiddle-schoolchildren.Sleep. 2003;26:455---8.
15.JohnsMW.Anewmethodformeasuringdaytimesleepiness:the EpworthSleepinessScale.Sleep.1991;14:540---5.
16.Spilsbury JC, Drotar D, Rosen CL,Redline S. The Cleveland AdolescentSleepinessQuestionnaire:anewmeasuretoassess excessivedaytimesleepinessinadolescents.JClinSleepMed. 2007;3:603---12.
17.FerreiraVR,CarvalhoLB,RuotoloF,MoraisJF,PradoLB,Prado GF.Sleepdisturbancescaleforchildren:translation,cultural adaptation,andvalidation.SleepMed.2009;10:457---63. 18.Bruni O, Ottaviano S, Guidetti V, Romoli M, Innocenzi M,
Cortesi F, et al. The Sleep Disturbance Scale for Children (SDSC).Constructionandvalidationofaninstrumentto eval-uatesleepdisturbancesinchildhoodandadolescence.JSleep Res.1996;5:251---61.
19.TannerJM.Growthatadolescence.Oxford:BlackwellScientific; 1962.
20.BMI-for-age (5---19 years). Growth reference data for 5---19 years.TheWHOReference2007. WorldHealth Organization; 2007[cited2007July].Available from:http://www.who.int/ growthref/who2007bmiforage/en/index.html.
21.SpruytK,SansCapdevilaO,SerperoLD,Kheirandish-GozalL, GozalD.Dietaryandphysicalactivitypatternsinchildrenwith obstructivesleepapnea.JPediatr.2010;156:724---30.
22.DevnaniP,BhaleraoN.Assessmentofsleepinessandsleepdebt inadolescentpopulationinUrbanWesternIndia.IndianJSleep Med.2011;5:143---53.
23.FalloneG,OwensJA,DeaneJ.Sleepinessinchildrenand ado-lescents:clinicalimplications.SleepMedRev.2002;6:287---306. 24.MatosMG,SimõesC,Tomé G,CamachoI,FerreiraM,Equipa AventuraSocial,etal.Asaúdedosadolescentesportugueses: relatóriodoestudoHBSC2010.Lisboa:CentrodeMaláriae Out-rasDoenc¸asTropicais/IHMT/UNL,FMH/UniversidadeTécnicade Lisboa;2012.p.11---60.
25.BernardoMP,PereiraEF,LouzadaFM,D’AlmeidaV.Durac¸ãodo sonoemadolescentesdediferentesníveissocioeconômicos.J BrasPsiquiatr.2009;58:231---7.
26.WahlstromK.Schoolstarttimeandsleepyteens.ArchPediatr AdolescMed.2010;164:676---7.
27.LiS,ArguellesL,JiangF,ChenW,JinX,YanC,etal.Sleep, school performance,and a school-basedintervention among school-agedchildren:asleepseriesstudyinChina.PLoSONE. 2013;8:e67928.
28.MoldJW, HoltzclawBJ,McCarthyL.Night sweats: a system-aticreviewoftheliterature.JAmBoardFamMed.2012;25: 878---93.
29.Arnardottir ES, Janson C,Bjornsdottir E, Benediktsdottir B, Juliusson S, Kuna ST, et al. Nocturnal sweating --- a com-monsymptomofobstructivesleepapnoea:theIcelandicsleep apnoeacohort.BMJOpen.2013;3:e002725.