SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Case
report
Reconstruction
of
chronic
patellar
tendon
rupture
using
graft
from
contralateral
patella
graft
together
with
reinforcement
from
flexor
tendons.
Case
report
夽
Eduardo
Frois
Temponi
a,∗,
Lúcio
Honório
de
Carvalho
Júnior
a,b,
Cláudio
Otávio
da
Silva
Bernardes
a,
Bruno
Presses
Teixeira
aaHospitalMadreTeresa,BeloHorizonte,MG,Brazil
bDepartmentofMusculoskeletalSystem,SchoolofMedicine,UniversidadeFederaldeMinasGerais,BeloHorizonte,MG,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received27May2015 Accepted2July2015 Availableonline2April2016
Keywords:
Patellarligament Rupture Reconstruction
a
b
s
t
r
a
c
t
Chronicpatellartendonruptureisararedisablinginjurythatistechnicallydifficulttorepair. Thetrueprevalenceofthisinjuryisunknown.Delayedreconstructionofchronicpatellar tendonrupturehasyieldedsuboptimalclinicalandfunctionalresults.Manydifferent sur-gicalmethodsforreconstructionofchronicpatellartendoninjuryhavebeenreported.In thisreport,wepresentacasewithchronicpatellartendoninjurythatwasaddressedusing atechniquethathadnotpreviouslybeendescribedintheliterature,throughcombining proceduresthathadbeendescribedseparately.Thereconstructionmethodpresentedin thisarticlehastheadvantagesofbeingeasyandreproducible,withoutarequirementof allografts.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Reconstruc¸ão
de
ruptura
crônica
do
tendão
patelar
com
enxerto
patelar
contralateral
associado
a
reforc¸o
com
tendões
flexores.
Relato
de
caso
Palavras-chave:
Ligamentopatelar Ruptura
Reconstruc¸ão
r
e
s
u
m
o
Arupturacrônicadotendãopatelarélesãoraraeincapacitanteeaindatecnicamentedifícil deabordar.Averdadeiraprevalênciadessalesãoédesconhecida.Areconstruc¸ãotardiadas rupturascrônicasdotendãopatelarapresentaresultadosclínicosefuncionaisabaixodo ideal.Muitosmétodoscirúrgicosdiferentesforamrelatadosparaareconstruc¸ãodotendão
夽
StudycarriedoutatKneeGroup,ServiceofOrthopedicsandTraumatology,HospitalMadreTeresa,BeloHorizonte,MG,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](E.FroisTemponi).
http://dx.doi.org/10.1016/j.rboe.2016.03.003
patelaremlesõescrônicas.Nesterelatoapresentamosumcasocomlesãocrônicadotendão patelarabordadocomtécnicaatéentãonãodescritanaliteratura,quecombina,todavia, técnicaspreviamente relatadas.Ométododereconstruc¸ãopresentenesteartigotema vantagemdeserfácilereprodutível,semanecessidadedealoenxertos.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.EsteéumartigoOpenAccesssobalicençadeCCBY-NC-ND (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Chronicruptureofthepatellartendonisanuncommon,but disablinginjury,ofunknownprevalence.1,2 Theimpairment
oftheextensormechanismresultsingreatfunctional disabil-ity,makingsurgicaltreatmentthegoldstandardtherapy.1–5
Diagnosticdelaymakesthetreatmenttechnicallydifficultand demanding,consideringtheproximalpatellarmigrationdue toquadricepsretraction,poorqualityoftheremaining ten-donandkneestiffness.5Complicationssuchaskneeflexion
deficit,quadricepsatony,surgicalwoundproblemsand surgi-calfailureassociatedwiththepreviouslydescribedmethods aredescribedintheliterature.Littleisknownaboutthe func-tionaloutcomesofthesepatients.1–9
Asitisararecondition withmany describedtreatment techniques,thereisnoconsensusonthe optimal manage-ment.Wepresentacasereportwiththeuseofautologous patellargraftreconstructionwithcontralateralbone-patellar tendon-bone (BPTB) associated with ipsilateral semitendi-nosusandgracilistendonsaugmentationforapatientwith chronicrupture ofthepatellartendon.Wedidnotfindany similarproceduresdescribedintheliteraturetodate.
Case
report
A36-year-oldmalepatient,previouslyhealthy,withahistory ofspontaneoustraumatic rupture ofthe left knee patellar
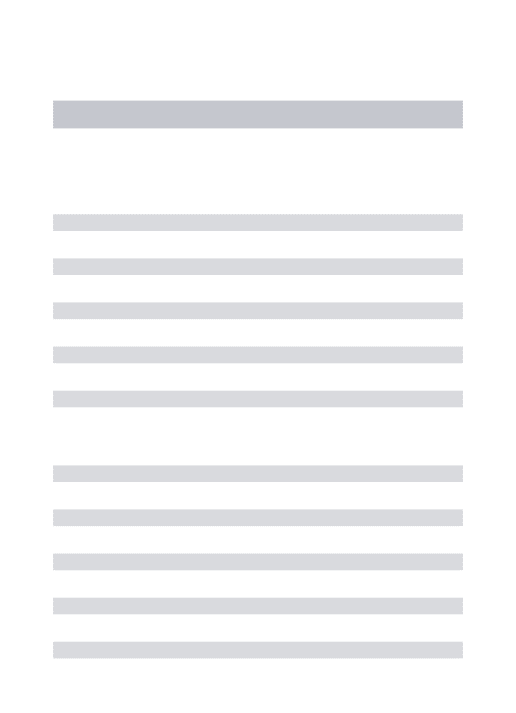
Fig.1–Schematicdrawingshowingcontralateralpatellargraftremovaltechnique(aandb)withsubsequentcontralateral
grafting,withhamstringsaugmentationpreservingtibialinsertions(c).
tendon during asoccer match in2009, underwent surgery 10daysaftertheincident atanotherinstitutionwithdirect repairwithtransosseousfixation. Accordingtothe patient, duringthepostoperativeperiodheusedakneebracethatkept thekneeextendedbyfourweeks,followedbygradual mobi-lizationafterthisperiod.Hereportedthatmonthsafterthe procedureheobservedproximalmigrationofthepatellawith subsequentonsetoflimping,lossofquadricepsstrengthand instability.
HesoughttreatmentattheKneeGroupofthe Orthope-dicsandTraumatologyServiceinAugust2014,complaining offunctionallimitationandextensionstrength impairment oftheaffectedknee.Onphysicalexaminationhehad: quadri-cepshypotrophy(thighcircumferentialmeasurement,10cm abovetheproximalpoleofthepatella–Right:43.5cm/Left: 40cm),symmetricalrangeofmotion(ROM)(0–130),decreased quadricepsstrength (10degreesdeficit ofactiveextension). Radiographs showed patella alta (Catton and Deschamps index: 2.2).By then,surgicaltreatmentwas offeredforthe chroniclesion.HehadTegnerlevelofactivityscoreof1and IKDCscoreof33.3.
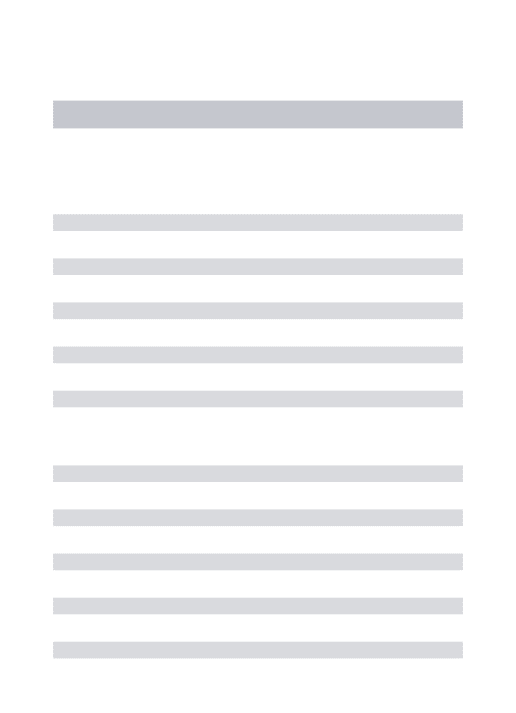
Fig.2–Preandpost-operativeradiographcomparison:(a,b)APandlateralviews,demonstratingpatellaaltaaccordingto
Catton–Deschampsindex(2.2).(c,d)APandlateralviewsdemonstratingpatellarandtibialfixationwithtwoscrews,with
patellardistalization.AP,anteroposterior.
andafterdebridementofscartissue,bonegrooveswere cre-atedonthepatellaandATT,ofsizessimilartotheBPTBgraft boneplugs(25mm-long×10mm-wide).Theboneblockswere thenadaptedtothepatellaandATTandfixedwith intrafrag-mentarycompressionusingtwopartiallythreadedcancellous screwsandtwosmall-fragmentcorticalscrewsinthepatella andthetibia,respectively.Thejointsurfaceofthepatellawas visualizedandpalpatedunderdirectview throughalateral mini-arthrotomytoavoidpossibleintra-articularpositioning ofsynthesismaterial.Thethirdstepwasharvesting ipsilat-eralsemitendinosusandgracilistendonsautograftswithan
open stripper, preservingthe tibialinsertion. Thetwo ten-dongraftswerethenpassedthroughthequadricepstendon attheproximalpoleofthepatellaandalongthepatella bor-dersinacircularform,tensionedandsuturedmatchingthe reconstructedpatellartendonlength(Fig.1).Aftertherepair, adequate patellarheightwasclinicallyconfirmedusingthe intercondylarroofandwithfluoroscopy,usingthenormalside asreference.
everytwoweeks,untilcompleteflexionwasrecovered.Partial weightbearingwasinitiatedimmediatelywithfull progres-sionattheendofsixweeks.Thepatientresumedworkafter fourmonthsandatthemoment(sixthmonthpostoperatively) is recovering muscle mass (gym) as preparation for retur-ningtohighdemandactivities.Currently,radiographsdisclose adequatepatellarheight(CattonandDeschampsIndex:1.1) (Fig. 2). His Tegner level of activity score is 5 and IKDC score73.6.
Discussion
Ruptureofthepatellartendonistheleastcommoncauseof kneeextensormechanisminjury,withestimatedforce17.5 times greater than the body weight being required for its rupture.1–3,5Therupturemechanismisusuallyaneccentric
overloadoftheextensormechanismwiththefoot fixedon theground andknee flexion.Repetitivemicrotraumas lead totendonweaknessandusuallyprecedetherupture. Patel-lartendonrupturescanbecausedbytrauma,associatedto systemicdiseases,aftertotalkneearthroplastyorACL recon-struction,andasalatecomplicationfollowingosteosynthesis withtibialintramedullarynailortheadministrationoflocal orsystemiccorticosteroids.4,5
The first reported cases of delayed repair date back to 1927 and since then, several different techniques and grafts have been reported for this treatment.1,5,6,8–10
Direct repair, distraction, reinforcement with autograft (contralateralpatellartendon,semitendinosustendon), allo-graft (extensor mechanism), Achilles tendon and syn-thetic materials are technique options that have been described.5
When using the contralateral BPTB autograft, we can reconstruct the extensor mechanism ofthe affected knee, accurately restore patellar height and ensure good stabil-ity and bone contactfor the consolidationof boneblocks, in addition to being a simple and reproducibletechnique, without the use of allografts or the even complementary materials.3,8Themaindisadvantagedescribedforthis
tech-niqueis morbidity ofthe donorsite, althoughShelbourne and Urchhave demonstrated thatthe removalofthe con-tralateral graft from a healthy knee does not affect its function.7
Gilmoreetal.5reportedthattechniquesusingautografts
ledtonofailuresintheseriesassessedandhadlower com-plicationratesthan any ofthe primary repairmethods.In the same study, they detected that chronic rupture repair withautografthadalowerfailureratethananyofthe com-bined main methods. This suggests that the repair using this technique would bethe method ofchoice forchronic ruptures.
The combination of the bone procedure with semi-tendinosus and gracilis tendon augmentation has some advantages:easytoremoveautografts,nosignificantincrease insurgicaltime, goodmechanicalstrength andno require-ment of synthetic implants or their removal in a second procedure.Thetibialinsertionpreservationofthehamstrings seemstopreserveviabilityandstability,inadditionto provid-ingbloodsupplyatsufficientquantitytoacceleratehealing.6
Alltheseprinciplesallowearlymobilizationandreducethe riskofstiffness.5,6,10
Jainetal.10 demonstratedimprovementinallfunctional
parameterswith80%recoveryofquadricepsstrengthwhen thereconstructionwasperformedwithflexortendonsina 4.5-yearfollow-up.Ourchoicetocombinebothtechniquesaims tosumthepositivepointsofeachinacaseofchronicrupture withaggressiverehabilitation.
The limitations ofthis study are the fact that this is a casereport,witharelativelyshort-termfollow-up.However, the resultswere significant, duetothe rarity ofthe injury and the particularity of the implemented treatment. Due tothe low incidenceofthis injury,mostpublished studies presentcasereportswithdifferentformsoftreatment. Com-parativestudies arenecessary todefine thebest treatment option.
Thisarticlemaybeusefulindailyclinicalpracticefor help-ing orthopedicsurgeonsintheirindicationsand treatment of this rare, but limiting, injury. It demonstrates a simple reproducibletechnique,whichdoesnotrequire supplemen-tarymaterial.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgement
ToDr.CláudioBeling,forhishelpcreatingtheschematic draw-ing.
r
e
f
e
r
e
n
c
e
s
1.GallieWE,LeMesurierAB.Thelaterepairoffracturesofthe patellaandruptureoftheligamentumpatellaand quadricepstendon.JBoneJointSurg.1927;9: 47–54.
2.RamseierLE,WernerCML,HeinzelmannM.Quadricepsand patellartendonrupture.Injury.2005;37(6):516–9.
3.DejourH,DenjeanS,NeyretP.Treatmentofoldorrecurrent rupturesofthepatellarligamentbycontralateralautograft. RevChirOrthopReparatriceApparMot.1992;78(1): 58–62.
4.GreisPE,LahavA,HolmstromMC.Surgicaltreatmentoptions forpatellatendonrupture,PartII:Chronic.Orthopedics. 2005;28(8):765–9.
5.GilmoreJH,Clayton-SmithZJ,AguilarM,PneumaticosSG, GiannoudisPV.Reconstructiontechniquesandclinicalresults ofpatellartendonruptures:evidencetoday.Knee.
2014;(November7),pii:S0968-0160(14)00255-5.
6.SundararajanSR,SrikanthKP,RajasekaranS.Neglected patellartendonruptures:asimplemodifiedreconstruction usinghamstringstendongraft.IntOrthop.
2013;37(11):2159–64.
7.ShelbourneKD,UrchSE.Primaryanteriorcruciateligament reconstructionusingthecontralateralautogenouspatellar tendon.AmJSportsMed.2000;28(5):651–8.
autograft:acasereport.KneeSurgSportsTraumatol Arthrosc.2007;15(12):1445–8.
9. CaseyMTJr,TietjensBR.Neglectedrupturesofthepatellar tendon.Acaseseriesoffourpatients.AmJSportsMed. 2001;29(4):457–60.