SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
article
Osteoid
osteoma
–
radiofrequency
ablation
treatment
guided
by
computed
tomography:
a
case
series
夽
Rosana
Raquel
Endo
a,∗,
Natalia
Fabris
Gama
a,
Suely
Akiko
Nakagawa
b,
Chiang
Jeng
Tyng
c,
Wu
Tu
Chung
b,
Fábio
Fernando
Eloi
Pinto
baHospitalServidorPúblicoMunicipaldeSãoPaulo,DepartamentodeOrtopediaeTraumatologia,SãoPaulo,SP,Brazil
bHospitalACCamargoCancerCenter,NúcleodeOrtopedia,SãoPaulo,SP,Brazil
cHospitalACCamargoCancerCenter,DepartamentodeRadiologiaIntervencionista,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received2June2016 Accepted7July2016
Availableonline28April2017
Keywords: Osteoidosteoma Radiofrequency
Boneneoplasms
Ablationtechniques
Computedtomography
a
b
s
t
r
a
c
t
Theosteoidosteomaisabenignprimarybonetumorthataffectsmainlymalesinthesecond andthirddecadesoflife.Radiographicfindingsshowaradiolucentnidussurroundedby reactivescleroticbone,particularlyinthelongbonesofthelowerextremity.Clinically,it presentspersistentpain,whichisworseatnightandimproveswithsalicylates.Itcanbea self-limitinginjury,withanaveragedurationofthreeyears,butbecauseofpainintensity andintolerancetoprolongeduseofnonsteroidalanti-inflammatories,surgicaltreatment isanoption.Thediagnosisissuspectedaccordingtothehistoryandradiographicfindings, andtheconfirmationismadebyhistologicalanalysis.Thetraditionalsurgicaltreatmentis thecompleteexcisionofthenidus,butsomedisadvantageshavebeendescribed,suchas difficultiesinlocalizingthelesionandriskoffractureduringtheprocedure,hospitalstayfor paincontrol,andunfavorableestheticoutcome.Theauthorsreportaseriesofcasestreated withthermalradiofrequencyablationguidedbycomputedtomographyinthisservice.Itis asafeandaneffectivepercutaneousmethodthataimstocure,minimizingthetraumaand morbiditywhencomparedwiththeconventionalblock-resectionmethod.
©2017PublishedbyElsevierEditoraLtda.onbehalfofSociedadeBrasileiradeOrtopedia eTraumatologia.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http://
creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedattheHospitalACCamargoCancerCenter,SãoPaulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](R.R.Endo).
http://dx.doi.org/10.1016/j.rboe.2017.04.005
338
rev bras ortop.2017;52(3):337–343Osteoma
osteoide
–
Tratamento
com
radioablac¸ão
guiada
por
tomografia
computadorizada:
uma
série
de
casos
Palavras-chave: Osteomaosteoide Radiofrequência Neoplasiasósseas Técnicasdeablac¸ão
Tomografiacomputadorizada
r
e
s
u
m
o
Oosteomaosteoideéumtumorósseoprimáriobenignoqueacometemaisosexo mas-culinonasegundaeterceiradécadasdavida.Radiograficamente,caracteriza-sepor um nichoradiolucentecercadoporossoescleróticoreativo,principalmenteemossoslongosda extremidadeinferior.Clinicamente,apresentaumadorpersistentedelongadurac¸ão,com piorianoturnaemelhoriacomsalicilatos.Emborapossaserumalesãoautolimitada,com durac¸ãomédiadetrêsanos,aressecc¸ãodalesãoéumaopc¸ãodetratamentodevidoà inten-sidadedadoreintolerânciaaousoprolongadodeanti-inflamatóriosnãohormonais.Sua suspeitadiagnósticabaseia-seprincipalmentenahistóriaclínicaenosachados radiográfi-cos,aconfirmac¸ãoéfeitapeloestudoanatomopatológico.Otratamentocirúrgicoclássicoé aexcisãocirúrgicacompletadonicho,porémsãodescritasdesvantagenscomoadificuldade paraalocalizac¸ãointraoperatóriadalesão,riscodefraturaduranteoprocedimento,tempo deinternac¸ãohospitalarparacontroleálgicoeresultadoestéticodesfavorável.Relatamos umasériedecasostratadoscomtermoablac¸ãoporradiofrequênciaguiadaportomografia computadorizadaemnossoservic¸o.Trata-sedeummétodopercutâneoseguroeeficazque temcomoobjetivoacura,minimizaotraumaeamorbidadedoprocedimento,quando comparadocomométodoconvencionalderessecc¸ãoembloco.
©2017PublicadoporElsevierEditoraLtda.emnomedeSociedadeBrasileirade OrtopediaeTraumatologia.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND
(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Osteoid osteoma is a benign primary bone tumorinitially
reported by Heine1; Bergstrand2 described its histology. In
1935,Jaffe3classifiedthisneoplasmasaclinicaland
patho-logicalentity,differentiatingitfromothertumors.
Thisisabenignprimaryneoplasmwhosenidusisformed byhypervascularizedimmatureosteoidtissue,surroundedby reactivescleroticbone.Itaccountsfor10%ofthebenignbone tumors4–6;itmostlyaffectsmales,inaratiorangingfrom1.6:1
to4:1.6,7Themostprevalentagegroupisthesecondtothird
decadesoflife.8
Osteoid osteoma can be observed in almost any bone
region,but it hasa higherincidenceinlongbones,mainly inthediaphysealregionofthetibiaandfemur.1,6
Clinically,it presentswithapersistent, long-lastingand
vague pain, with nocturnal worsening, that is sometimes
relieved withthe useofsalicylates and non-steroidal anti-inflammatorydrugs(NSAIDs).7,9
Radiographically,itischaracterizedbythepresenceofa radiolucent nidus whose diameter rarely exceeds 2cm,1,4,9
oftensurroundedbyreactivescleroticbone.
Themain radiographic differential diagnoses of osteoid
osteoma are bone infarction, chronic osteomyelitis, and
chondroblastoma.10 Sometimes, complementary imaging
testssuchascomputedtomography (CT)ormagnetic
reso-nanceimagingcanprovideabettercharacterizationofthe niduse11,12;bonescanmay revealanintensenidusactivity
andlowactivityofthesurroundingreactivearea.13Thefinal
diagnosisismadethroughtheanatomopathologicalexam. Macroscopically, the nidus is well-delimited and
wine-colored. Normally, it does not exceed 2cm in diameter.
Microscopically,itiscomposedofarichlyvascularizedosteoid matrixandamatureintertwinedbonetrabeculae;itmayalso featureareasofcentralossification.
Classically, treatment consistsof block resection of the nidus.However,intraoperatively,itmaybedifficultto iden-tifytheexactlocationofthetumor.9Thus,minimallyinvasive
approachessuchasthepercutaneousmethod,aidedby imag-ingmethods,overridethisdifficulty.
CT-guidedradiofrequencyablationisapercutaneous
tech-nique in which the use of electrodes connected to an
energysourceleadstoproteindenaturationandcoagulative necrosis.14However,adisadvantageofthemethodisthelack
ofmaterialforanatomopathologicalexaminationand
diag-nosticconfirmation.
This study aimed to demonstrate the efficacy of the
adoptedtreatment,withsatisfactoryresultsinthecontrolof patientswithosteoidosteoma.
Material
and
methods
Theauthorsdescribethecasesoffivepatientswith
diagnos-ticsuspicionofosteoidosteomawhounderwentCT-guided
radiofrequencythermoablationbetweenSeptember2010and
March2013atthisservice.
Theneedforaninformedconsentwaswaived,asdatawas collectedthroughmedicalrecords.
Patients reported pain as main complaint; no patient
reportedapredilectionforthenightperiodandallpresented failuretorespondtodrugtreatmentwithsalicylates.
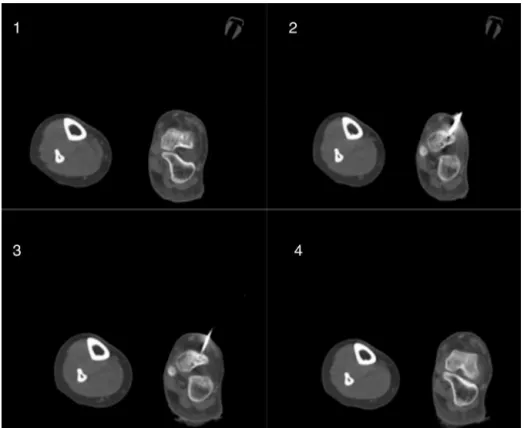
Fig.1–(1)AxialCTscanoftheleftfoot,indicatingosteolyticlesionwithsclerotichalo,locatedinthedomusofthetalus, compatiblewithosteoidosteoma;(2)introductionoftheJamshidineedlethroughthenidus;(3)positioningoftheablation needleinthepathcreatedbytheJamshidineedle;(4)controlCTaftertheprocedure.Case1:B.S.O.C.,16years,female.
340
rev bras ortop.2017;52(3):337–343Fig.3–(1)AxialCTscanoftherightarmshowinganosteolyticlesionwithsclerotichalo,locatedinthehumerus, associatedwithcorticalthickening,suggestiveofosteoidosteoma;(2)beginningofinsertionoftheJamshidineedle;(3) Jamshidineedleinsertedinsidethehumerus;(4)CToftherightarmshowingthecorrectpositioningoftheablationneedle insidethelesion.Case3:R.M.,38years,male.
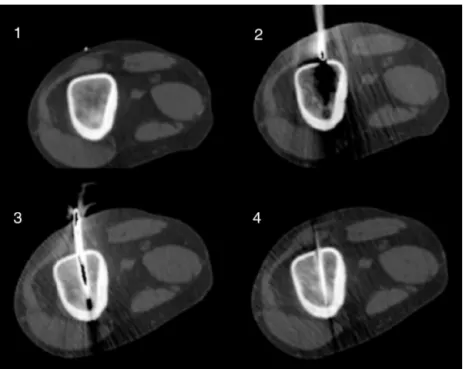
Fig.5–(1)AxialCToftherightthighshowinganosteolyticimageinthefemoralcortex;(2)imageshowingtheJamshidi needleinsidethefemoralcortex;(3and4)CTcontrolofthepathmadebytheJamshidineedle;(5and6)CTcontrolshowing theablationneedlewithinthenidus.Case5:D.C.N.,20years,male.
PatientsincludedinthestudyarelistedinTable1;Figs.1–5
presenttheimagesacquiredduringtheprocedure.
Proceduretechnique
Patientis positionedon the CTframeunder general anes-thesia.Asepsis and antisepsismeasuresperformed forthe procedure.CTimagesaremade,identifyingtheexactlocation ofthenidus,itsrelationshipwithadjacentstructures,andthe bestpathtoitscenter.
AfterCT planning,an8-gaugeboneneedle (Jamshidi)is insertedintothenidus,thusmakingtheorificethroughwhich
Table1–Listofthepatientsincludedinthestudy.
Age Gender Location
Case1 16years Female Talus
Case2 21years Female Olecranon
Case3 38years Male Humerus
Case4 38years Male Tibia
342
rev bras ortop.2017;52(3):337–343thecool-tipsingleradiofrequencyneedle,witha1-cm bone-specificactiveprobe,ispassed.Aftertheneedleisintroduced anditspositioningisconfirmedthroughimagingexam, abla-tionisinitiated.Theclassicalinitialcyclelastsapproximately
12min,andthemaximumtemperatureoftheneedletothe
end ofthe procedure is60◦C. Coolingis providedby 0.9% salineeveryminute,maintainingthetemperatureoftheactive probebelow10◦C.Afterthisfirstcycle,coldsalinecirculation
isturnedoffandthesecondcyclestarts.Thecharringcycle isdonewithoutcooling;itlasts4–6minandthetemperature reaches80◦Cto90◦C.
Results
Follow-up consisted of clinical and radiographic
examina-tionsafterthe firstweekoftheprocedure, aswell asafter thefirst,sixthand12thmonthsoftheprocedure;afterthis period,patientswereconsideredtobeinremissionandtold toreturnyearly.Themostimportantperiodtoevaluatetumor recurrenceiswithinthefirst12months.9Intheablation
treat-ment,nomaterialforanatomopathologicalexaminationwas retrieved.Nointercurrenceswereobservedduringtheablative procedure;patientsevolvedwithoutradiographicrecurrence ofthelesionuntilthepresent,andwithcompleteresolution ofthepain.
Discussion
Osteoidosteomaisabenignbonetumorthatusuallyaffects young individuals.Ithas a typicalclinical presentation; in mostcases,thepainisintermittent,withnocturnal worsen-ing,andasatisfactoryresponsetosalicylates.Itsdiagnostic suspicionisbasedmainlyonclinicalhistory,physical exami-nation,andradiographicfindings.9
Theclassictreatmentrequirescompletesurgicalexcision
ofthe nidus. The disadvantages ofthis procedure include
thedifficultyinlocatingtheintraoperativelesion,evenwith theuseofimage-guidedKirschnerwires;theneedforanew approachwhenresectionisincomplete;theriskofdamaging adjacentstructures;andtheriskofpostoperative complica-tionssuchasunsatisfactoryestheticresultsandvulnerability tofracturesduetothebonedefectcausedbyresection.For this reason,insome casesit isnecessary touse synthetic materialandbonegrafts,whichincreases themorbidityof theprocedure.15,16
TC-guidedradiofrequencythermoablationisaminimally
invasive percutaneous technique with low morbidity and
high accuracyinlocatingthe lesion.Itspossible complica-tions include cellulitis, bleeding, and infection at the site
of entry of the needle into the skin. Care must be taken
regarding the surrounding structures, such as the nerves; respectingthe1-cmdistancelimitfromthesestructurestothe activeprobeavoidsthermallesions.14Theoretically,themain
disadvantageofthismethodistheabsenceof anatomopatho-logicalconfirmationofthediagnosis.However,someauthors defendthatthediagnosisispredominantlyclinicaland radio-graphic;histopathologicalconfirmationisnotnecessary,and itsabsencedoesnotinterfereintheclinicaloutcome.14,15,17,18
Thelimitations ofthis study were the small numberof patientsandtheshortfollow-uptimeelapsedfromthe treat-menttothedraftingofthepresentarticle.
The results obtained in the study are similar to those reportedbyotherauthors.14–16,19,20
Conclusion
CT-guidedradioablationisanappropriateoptionforthe treat-mentofosteoidosteoma,presentinggoodresults.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgement
ToCassiada Silvaforthehelpprovidedinconductingthis study.
r
e
f
e
r
ê
n
c
i
a
s
1.HeineJ.EinheilenderKnochensequesterundder
GrundphalanxdesRingfingers.ArchKlinChir.
1927;146:737–53.
2.BergstrandH.Übereineeigenartige,wahrscheinlichbisher
nichtbeschriebeneosteoblastischeKrankheitindenlangen
KnochenderHandunddesFusses.ActaRadiol.
1930;11(6):596–613.
3.JaffeHL.Osteoidosteoma.Abenignosteoblastictumor
composedofosteoidandatypicalbone.ArchSurg.
1935;31(5):709–28.
4.GreenspanA.Benignbone-forminglesions:osteoma,osteoid
osteoma,andosteoblastoma.SkeletalRadiol.
1993;22(7):485–500.
5.BusserWM,HoogeveenYL,VethRP,SchreuderHW,BalguidA,
RenemaWK,etal.Percutaneousradiofrequencyablationof
osteoidosteomaswithuseofreal-timeneedleguidancefor
accurateneedleplacement:apilotstudy.Cardiovasc
InterventRadiol.2011;34(1):180–3.
6.KransdorfMJ,StullMA,GilkeyFW,MoserRPJr.Osteoid
osteoma.Radiographics.1991;11(4):671–96.
7.BoscainosPJ,CousinsGR,KulshreshthaR,OliverTB,
PapagelopoulosPJ.Osteoidosteoma.Orthopedics.
2013;36(10):792–800.
8.AkhlaghpoorS,AzizAhariA,ArjmandShabestariA,
AlinaghizadehMR.Radiofrequencyablationofosteoid
osteomainatypicallocations:acaseserie.ClinOrthopRelat
Res.2010;468(7):1963–70.
9.CampanacciM,RuggieriP,GasbarriniA,FerraroA,
CampanacciL.Osteoidosteomadirectvisualidentification
andintralesionalexcisionoftheniduswithminimalremoval
ofbone.JBoneJointSurgBr.1999;81(5):814–20.
10.BecceF,TheumannN,RochetteA,LarousserieF,CampagnaR,
CherixS,etal.Osteoidosteomaandosteoid
osteoma-mimickinglesions:biopsyfindings,distinctive
MDCTfeaturesandtreatmentbyradiofrequencyablation.Eur
Radiol.2010;20(10):2439–46.
11.LiuPT,KujakJL,RobertsCC,deChadarevianJP.Thevascular
groovesign:anewCTfindingassociatedwithosteoid
12.YipPS,LamYL,ChanMK,ShuJS,LaiKC,SoYC.Computed
tomography-guidedpercutaneousradiofrequencyablationof
osteoidosteoma:localexperience.HongKongMedJ.
2006;12(4):305–9.
13.MotamediD,LearchTJ,IshimitsuDN,MotamediK,KatzMD,
BrienEW,etal.Thermalablationofosteoidosteoma:
overviewandstep-by-stepguide.Radiographics.
2009;29(7):2127–41.
14.RosenthalDI,HornicekFJ,TorrianiM,GebhardtMC,Mankin
HJ.Osteoidosteoma:percutaneoustreatmentwith
radiofrequencyenergy.Radiology.2003;229(1):171–5.
15.BareiDP,MoreauG,ScarboroughMT,NeelMD.Percutaneous
radiofrequencyablationofosteoidosteoma.ClinOrthopRelat
Res.2000;373:115–24.
16.CantwellCP,ObyrneJ,EustaceS.Currenttrendsintreatment
ofosteoidosteomawithanemphasisonradiofrequency
ablation.EurRadiol.2004;14(4):607–17.
17.WoertlerK,VestringT,BoettnerF,WinkelmannW,HeindelW,
LindnerN.Osteoidosteoma:CT-guidedpercutaneous
radiofrequencyablationandfollow-upin47patients.JVasc
IntervRadiol.2001;12(6):717–22.
18.RehnitzC,SprengelSD,LehnerB,LudwigK,OmlorG,MerleC,
etal.CT-guidedradiofrequencyablationofosteoidosteoma
andosteoblastoma:clinicalsuccessandlong-termfollowup
in77patients.EurJRadiol.2012;81(11):3426–34.
19.LindnerNJ,OzakiT,RoedlR,GoshegerG,WinkelmannW,
WörtlerK.Percutaneousradiofrequencyablationinosteoid
osteoma.JBoneJointSurgBr.2001;83(3):391–6.
20.CribbGL,GoudeWH,CoolP,TinsB,Cassar-PullicinoVN,
ManghamDC.Percutaneousradiofrequency
thermocoagulationofosteoidosteomas:factorsaffecting