rev bras ortop.2017;52(5):621–624
SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Case
Report
Dynamic
ulnar
impaction
syndrome
in
tennis
players:
report
of
two
cases
夽
Edgard
de
Novaes
Franc¸a
Bisneto
UniversidadedeSãoPaulo,HospitaldasClínicas,InstitutodeOrtopediaeTraumatologia,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received5August2016 Accepted22August2016 Availableonline16August2017
Keywords: Wristinjuries Tennis/injuries Fibrocartilage/injuries Ulnocarpalimpaction
a
b
s
t
r
a
c
t
Inthisreport,twotennisplayerswithsymptomsofulnarimpactionsyndromearereviewed. Bothplayershaveneutralulnarvariance.Thesecasesrepresentdynamiculnarimpaction syndrome,whentheimpactbetweenulnaandcarpusoccursduringconditionsofpronated grip.Theliteratureandthetreatmentofthesetwocasesarediscussed.
©2017SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http://
creativecommons.org/licenses/by-nc-nd/4.0/).
Síndrome
do
impacto
ulnocarpal
dinâmico
em
tenistas:
relato
de
dois
casos
Palavras-chave:
Traumatismosdopunho
Tênis/lesões
Fibrocartilagem/lesões Impactoulnocarpal
r
e
s
u
m
o
Orelatoapresentaoscasosdedoistenistasportadoresdedornobordoulnardocarpo comsinaisdeimpactonosemilunar.Ambossãoportadoresdeulnaneutra.Essescasos representamumaentidadedenominadasíndromedoimpactoulnocarpaldinâmiconaqual ocorreoimpactoentreacabec¸adaulnaeocarpoemsituac¸ãodepronac¸ãocompunho fechadoduranteaatividadefísica.Aliteraturaeotratamentodosdoiscasossãodiscutidos noartigo.
©2017SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevierEditora Ltda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://
creativecommons.org/licenses/by-nc-nd/4.0/).
夽
PaperdevelopedatUniversidadedeSãoPaulo,HospitaldasClínicas,InstitutodeOrtopediaeTraumatologia,SãoPaulo,SP,Brazil. E-mail:[email protected]
http://dx.doi.org/10.1016/j.rboe.2017.08.003
622
rev bras ortop.2017;52(5):621–624Introduction
Ulnocarpal impaction syndrome (UCIS) is a degenerative
lesion characterizedbycompression or impactofthe ulna
head against the semilunar bone and/or the pyramidal
bone,withor withoutlesionofthetriangularfibrocartilage complex.1–3
Generallyassociatedwiththepresenceofulnaplus,UCIS may alsooccur inthe presenceofneutralorminus ulna.4 Duringpronationthereisarelativeshorteningbetweenthe radiusandtheulna,andinsituationsofneutralorminusulna
shorterthan2mmanimpactcanoccurbetweenthecarpus
andtheulnahead,thisconditioniscalleddynamiculnocarpal impactionsyndrome(UCIS).4
UCISinthepresenceofneutralorminusulnaisdescribed inpronationsituationsassociatedwithgripstrength,common insportsactivitiessuchastennisorbaseball.5
Inthisreport,twocasesoftennisplayerswithUCISwill bepresented,andtreatedarthroscopically.Afterthe presen-tation of the cases, a discussion of the literature will be performed.
Case
report
1
A20-year-old female patient, who isa tennis playerat an Americanuniversity,witharightwristtriangular fibrocarti-lagelesion,diagnosedattheuniversity.
Whensheunderwentarthroscopyatthatmedicalservice withfibrocartilagedebridementandwristsynovectomy,
asso-ciatedsemilunarchondromalaciawasdiagnosed.
Aftersevenmonthsofsurgery,andintenserehabilitation, thepainpersistedpreventingherfromplaying.
Onphysicalexamination,sheshowedpainatmaximum
supination;positivefoveasign(painatulnarvolarpalpation oftheulnahead);absenceofinstabilityofthedistalradioulnar joint(DRUJ);normalwristROMandlowpaintoulnardeviation againstresistance.
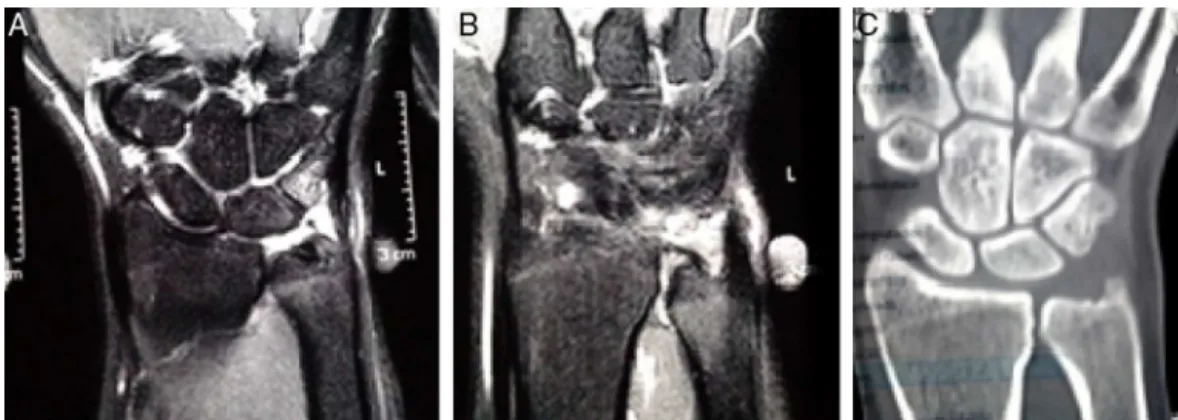
Imaging demonstrates triangular fibrocartilage lesion, intensesynovitisandedemaofthesemilunarandpyramidal bones.Presenceofneutralulna(Fig.1)wasalsonoted.
Patientunderwentnewarthroscopyofthewristwith evi-dentsituationofimpactionseenintheintraoperativeperiod duringpronosupinationofthewrist.Arthroscopicwafer pro-cedure,aswellasdebridementoftriangularfibrocartilageand loosecartilageofthesemilunar(Fig.2),wasperformed.
The patient remained immobilized with an
antebra-chiopalmar orthesis with epicondylar block during three
weeks. She was referred to rehabilitation, and returned
to her sports activities with no pain four months after
surgery.
Case
report
2
A49-year-oldmalepatient,amateurtennisplayer,whoplayed
every weekend, presented with chronic, progressive pain,
mainly when performing forehand technique while playing
tennis.
Onphysicalexamination,hepresentedwithpainat max-imumsupination;positivefoveasign,absenceofinstability ofthedistalradioulnarjoint(DRUJ);normalwristROMand no pain at ulnar deviationagainst resistance.This patient
also presented pain on palpation of the projection of the
interosseousscaphosemilunarligament(SLL),buttheWatson testwasnegative.
Magneticresonanceimagingshowedsemilunarand
pyra-midalboneedema,triangular fibrocartilagelesionand sus-picionofpartiallesiononthescaphosemilunarinterosseous ligament,confirmedintraoperatively(GeisslerIIItypelesion). Neutralulna(Fig.3)wasalsonoted.
Thepatientunderwentwristarthroscopy,andulnocarpal
impactionwasalsoobservedduringpronosupinationofthe
wrist(Fig.4).Arthroscopicwaferanddebridementoftriangular fibrocartilage,therewasnolooselunarcartilage.Inthiscase,
SLL debridementwasperformed,alongwith
scaphosemilu-narandscaphocapitatepercutaneousfixationwithKirschner wires.Inthiscase,duetoSLLtreatment,immobilizationwas maintainedfor6weeks.
Discussion
Whenconsideringpainfulsyndromesinathleteswrists, sev-eralaffectionscanbementioned4–7:
• Fractures ofthedistalextremity oftheradius, scaphoid,
hamate,pisiform.
• Temporaryorpermanenttraumaticepiphysiodesis.
• Synovitis(dorsalwristimpactionsyndrome).
• Ligament lesions, scaphosemilunar ligament, triangular
fibrocartilagecomplex.
• Pseudoarthrosisofthehamatehook.
• Tendinopathyorcarpalulnarextensortendondislocations.
• Degeneration,duetoimpact,ofthetriangularfibrocartilage
complex.
Regardingthedynamiculnar-carpalimpact,thisshouldbe consideredwhenthereispainattheulnaredgeofthecarpus, inthepresenceofneutralorminusulna,insituationsof fore-armpronationgrip.Onphysicalexaminationthesignalofthe foveamaybepositive,associatedwithulnarpainatmaximum pronation.Wristrangeofmotionisgenerallypreservedand theremaybenopainfordailyactivitieswithnoload.
Magnetic resonance imaging (MRI) or radiographs on
pronationwithpalmargrip(pronatedgripviews)canhelpwith diagnosis8(Fig.5).
Jang etal.9 statethatUCIS isoneofthe mostcommon causesofarthroscopyreviewofthewristduetopersistence ofpain.
Thedynamicvisualizationoftheinsinuationoftheulna headabovetheradiusjointobservedbytheportals3–4,4–5 and6Rwasfundamentalinthediagnosisinthesetwocases, especiallyincase1,inwhichthemagneticresonanceimaging
showed no clearsigns ofulnocarpal impaction. The
chon-drallesioninthesemilunarisalsoasignificantfindingofthe UCIS.
rev bras ortop.2017;52(5):621–624
623
Fig.1–Imagesofcase1.(A)MRIevidencingsynovitisandsemilunarandpyramidaledema;(B)lesionofthetriangular fibrocartilageinthedistalportiononly;and(C)tomographydemonstratingneutralulna.
Fig.2–Arthroscopicwaferprocedure.(A)lesionoffibrocartilagewithulnaheadexposure;(B)semilunarcondrallesion;(C) insinuationoftheulnaheadduringpronationabovetheradiusjointline;and(D)arthroscopicwafer.
Fig.3–(A)MRIevidencestriangularfibrocartilagelesion;(B)edemaontheulnahead;and(C)semilunaredema.
Fig.4–Wafer-likeprocedure.(A)Fibrocartilagelesionwithulnaheadexposure;(B)fibrocartilagebulging(arrow)onwrist
624
rev bras ortop.2017;52(5):621–624Fig.5–Radiographinpronationwithpalmargrip(pronatedgripviews).8(A)Withnopronation;and(B)pronationwith
palmargripthatalterstheulna-radiusrelation.Source:TomainoandElfar(2005).
hadadegenerativelesionandtherewasnoneedtousedistal radioulnarportals.Noneofthepatientspresentedinstability ofthedistalradioulnarjoint.
Thisauthor considers the postoperative immobilization
important after any arthroscopic procedure of the wrist,
for pain control and stabilization of the inflammatory
process.Immobilizationwithawristorthoticswithor
with-out epicondyle block is generally used for three to six
weeks,depending on concomitant procedures.Thepatient
referred to functional limb rehabilitation for four to eight weeks.
TheimportanceofUCISisinthepossibilityofbeingmuch moreprevalentthanisimaginedduetotheimmensenumber ofpeoplewhopractisesportsthatusepalmargripassociated withforearmpronation,suchastennis,golf,baseball, bowl-ing,canoeing,etc.Therecognitionandearlytreatmentofthis syndromeisfundamentalforthereintroductionoftheathlete tohis/hersportspractice.
Conflicts
of
interest
Theauthordeclaresnoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.IwasakiN,IshikawaJ,KatoH,MinamiM,MinamiA.Factors
affectingresultsofulnarshorteningforulnarimpaction
syndrome.ClinOrthopRelatRes.2007;465:215–9.
2.LohYC,VanDenAbbeeleK,StanleyJK,TrailIA.Theresultsof
ulnarshorteningforulnarimpactionsyndrome.JHandSurg
Br.1999;24(3):316–20.
3.CogginsCA.Imagingofulnar-sidedwristpain.ClinSports
Med.2006;25(3):505–26.
4.TomainoMM.Ulnarimpactionsyndromeintheulnarnegative
andneutralwrist.Diagnosisandpathoanatomy.JHandSurg
Br.1998;23(6):754–7.
5.BaerDJ.Dynamiculnarimpactionsyndromeinacollegiate
baseballplayer.IJATT.2014;19(3):15–9.
6.FufaDT,GoldfarbCA.Sportsinjuriesofthewrist.CurrRev
MusculoskeletMed.2013;6(1):35–40.
7.CornwallR.Thepainfulwristinthepediatricathlete.JPediatr
Orthop.2010;302Suppl.:S13–6.
8.TomainoMM,ElfarJ.Ulnarimpactionsyndrome.HandClin.
2005;21(4):567–75.
9.JangE,DanoffJR,RajferRA,RosenwasserMP.Revisionwrist
arthroscopyafterfailedprimaryarthroscopictreatment.J