SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
article
Do
patients
lose
weight
after
total
knee
replacement?
夽
Carlos
Roberto
Schwartsmann
a,b,∗,
Alexandre
Moreira
Borges
b,
Geraldo
Luiz
Schuck
de
Freitas
b,
Eduardo
Zaniol
Migon
b,
Gustavo
Kaempf
de
Oliveira
b,
Marcos
Wainberg
Rodrigues
baUniversidadeFederaldeCiênciasdaSaúdedePortoAlegre(UFCSPA),PortoAlegre,RS,Brazil
bComplexoHospitalardaSantaCasadePortoAlegre,PortoAlegre,RS,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received4November2015 Accepted29March2016 Availableonline24January2017
Keywords:
Obesity
Kneearthroplasty Bodymassindex
a
b
s
t
r
a
c
t
Objective:Severalstudiesshowthatpatientsundergoingtotalkneearthroplasty(TKA)tend tomaintainorgainweightaftertheprocedure,whichwouldresultinincreasedwearofthe prosthesisandnewsurgicalinterventionsinasmallerperiodoftimeincomparisonwith patientswithadequatebodymassindex(BMI).Theaimofthisstudywastoinvestigatethe effectofTKAsurgeryonthesepatients’BMI.
Methods:Initiallytherecordswereanalyzed,chosenatrandomfrom91patientsundergoing TKAduringtheperiodfromAugust2011toJuly2013.PatientswerestratifiedbyBMIas normalweight(BMIbetween20and25),overweight(BMIbetween25and30),andobesity (BMI>30).Theywerere-evaluatedinaminimumperiodof18months.
Results:Themeanageofthesamplepopulationwas68.1years;69.1formenand67.2for women.ThemeanpreoperativeBMIwas27.24kg/m2.Amongthestudyparticipants,inthe
preoperativeperiod,17patientshadnormalweight,65wereoverweight,andninewere obese.Postoperativeanalysisshowedweightlossin41patients(46%),andweightgainin 50patients(54%).ThemeanpostoperativeBMIwas27.16kg/m2,ingeneral,experiencinga
slightdeclineinthemeanBMIof0.08kg/m2.
Conclusion: PatientswhounderwentTKAdidnotachievesignificantreductioninBMIafter surgery.
©2017PublishedbyElsevierEditoraLtda.onbehalfofSociedadeBrasileiradeOrtopedia eTraumatologia.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedattheSantaCasadePortoAlegre,Servic¸odeOrtopediaeTraumatologia,PortoAlegre,RS,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](C.R.Schwartsmann). http://dx.doi.org/10.1016/j.rboe.2017.01.003
Os
pacientes
emagrecem
após
artroplastia
total
de
joelho?
Palavras-chave:
Obesidade
Artroplastiadojoelho Índicedemassacorporal
r
e
s
u
m
o
Objetivo: Diversosestudosdemonstramquepacientessubmetidosàartroplastiatotaldo joelho(ATJ)tendemamanterouaganharpesocorporalapósoprocedimento,oque acar-retaria aumentonodesgasteda próteseenovasintervenc¸õescirúrgicasemumtempo inferioràquelesquesemantémemíndicedemassacorporal(IMC)adequado.Oobjetivo desteestudofoiinvestigaroefeitodacirurgiadeATJnoIMCdessespacientes.
Métodos:Inicialmenteforamanalisadososprontuários,escolhidosaoacaso,de91pacientes submetidosàATJdeagostode2011ajulhode2013.Ospacientesforamestratificadospelo IMCcomopesonormal(IMCentre20-25),sobrepeso(IMCentre25-30)eobesidade(IMC>30) ereavaliadosem18mesesnomínimo.
Resultados: Amédiadeidadedapopulac¸ãoamostralfoide68,1anos,69,1parahomense 67,2paramulheres.OIMCmédiopré-operatóriofoide27,24kg/m2.Entreosparticipantesdo
estudo,noperíodopré-operatório,17pacientesapresentavampesonormal;65,sobrepesoe nove,obesidade.Aanálisepós-operatóriademonstroudiminuic¸ãonopesoem41pacientes (46%)eganhoponderalem50(54%).OIMCmédiopós-operatóriofoide27,16kg/m2,de
formageral,ocorreuumaligeiraquedadoIMCmédioem0,08kg/m2.
Conclusão: OspacientessubmetidosàATJnãoobtiveramreduc¸ãosignificativadoIMCapós oprocedimentocirúrgico.
©2017PublicadoporElsevierEditoraLtda.emnomedeSociedadeBrasileirade OrtopediaeTraumatologia.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Obesityisaseriousprobleminbothdevelopedanddeveloping countries.Itislikelyoneofthefactorsthatismostassociated withtheincreaseinthemorbimortalityoftheglobal popula-tionnowadays.1Theincreaseinobesitywilllikelycausean
increaseintheincidenceofkneeosteoarthritisandhencein thenumberoftotalkneearthroplasties(TKA).2
EvidenceindicatesthattherelativerisktoundergoaTKA variesfrom3.20foroverweightindividuals to32.73in indi-vidualswithmorbidobesitygradeIII.3Highbodymassindex
(BMI)hasbeenshowntobeariskfactorforworseningofknee osteoarthritis.1–5 Therelationshipbetweenarthroplastyand
increasedBMIisthereforeincreasinglyimportantinrelation totheoutcomesinthepostoperativeperiodandthe expecta-tionsofpatients.5
Todate,the gold standard treatmentforobese patients withkneeosteoarthritisremainsthesubjectofdebate,since patients with a high BMI (>30kg/m2) are at higher risk of
developingcomplicationsafterTKA.6Kerkhoffsetal.7suggest
thatthesepatientsshouldfirstundergoabodyweightcontrol programinordertoreducetheriskofpostoperative compli-cations,whichiswhymanysurgeonsarereluctanttoperform TKAinthispopulation.8TheimpactofbodyweightonTKA
hasnotbeenfullyexplored.Clinicallysignificantbodyweight gainafterTKAcouldposepotentiallyharmfulhealthrisks.9
However, preoperative weight loss inTKA is an impor-tant measure that should be strongly encouraged, since highBMIhasbeenshowntobeariskfactorforworsening kneeosteoarthritis.10–15 Thebenefitsofweightlossinclude
decreasedsurgicalriskandincreasedlongevityofthe pros-theticimplant.However,severalstudieshavedemonstrated
thatpatientswhoundergoTKAtendtomaintainorgainbody weightafterthesurgicalprocedurewhencomparedwiththe periodbeforethe placementoftheprosthesis,whichleads toanacceleratedincreaseinprosthesiswear.Therefore,the obesepatientwillhavetoundergoanewsurgicalintervention inashortertimeintervalthanthosewithanadequateBMI.1,3,4
The rate of obesity among the adult population has increased inepidemic proportions. Statistical datasupport thehypothesisthatobesityrateswillcontinuetogrowuntil 2030.16Accordingtothemedicalliterature,theobeseand
over-weightpopulations,assessedbyBMI,aremorelikelytohave conditions such as knee osteoarthritis.1–3,14 In the present
study,itwasobservedthatthevastmajorityofpatientseligible forTKAareabovetheiridealweight(82%).
Thesignificantimprovementinjointpainandfunctional limitations after TKA14,15 does not change the patients’
lifestylehabits.17–20
Theresultsofthesestudiesarealarming,sincethenumber ofyoungpatientsundergoingkneearthroplastyisgradually increasing.13,16 Furthermore,ahigher-than-ideal BMIraises
concernsregardingthelowerdurabilityoftheprosthesis.13,20
ThepresentstudyaimedtoinvestigatetheeffectofTKA ontheBMIofpatientsundergoingthisprocedure.
Material
and
methods
whounderwentkneearthroplasty,withaminimum1.5years ofpost-operativefollow-up.Patientswithincompletedataand recordsandthosewhowerenotweighed(ineitherthe pre-orpostoperativeperiods) wereexcluded.Ofthe100records analyzed,91 met the aforementioned criteria. Ofthese, 21 (24%)were menand 70(76%)werewomen.Inthe preoper-ativeperiod,themeanageofthesamplepopulationwas68.1 years(SD±2);69.1±2formenand67.2±2forwomen.
Bothweightand heightinthe preoperativeperiodwere measuredonaconventionalscalewithaheightgauge.BMI wascalculatedusingthebodymass/height2formula.The
cur-rentweightofthe patientswas assessedagain atleast1.5 yearsaftersurgery.PatientswerestratifiedbyBMIasfollows: normalweight(between20and25),overweight(between25 and30),andobese(over30),asproposedbytheWorldHealth Organization.11,12
Datawere analyzedbySPSSsoftwareforWindows, ver-sion17;descriptivestatisticsandfrequencydistributionwere observed.Groupswere correlatedusing theMann–Whitney test.BMIvariationswerecomparedbetweenmaleandfemale patients,andacomparisonofthegroupsstratifiedaccording toBMIwasalsomade.
Results
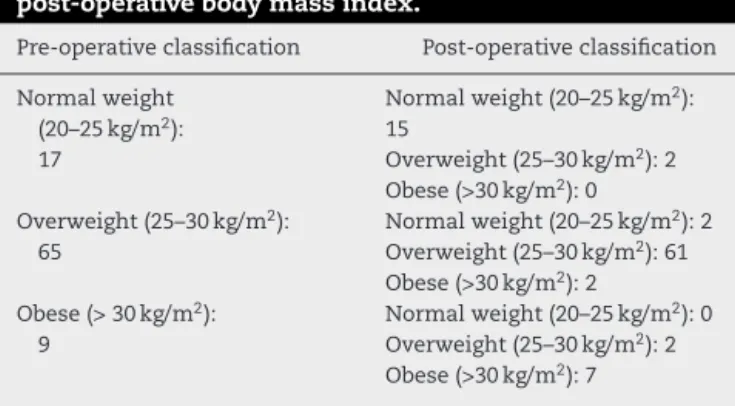
MeanpreoperativeBMIwas27.24kg/m2.AsshowninTable1,
inthepreoperativeperiod17patientshadnormalweight(BMI 20–25),65wereoverweight(25–30),andninewereobese(>30). Postoperativeanalysisshowedadecreaseinweightin41 patients(46%)andweightgainin50(54%).Meanpostoperative BMIwas27.16kg/m2;overall,aslightdecreaseof0.08kg/m2
wasobserved.Therefore,meanBMIofthestudypopulation remainedpracticallyunchanged.
Fig.1presentstheBMIvariationwithineachgroup.Inthe groupwithpreoperativeBMIfrom20to24.9,aslighttendency towardincreasedBMIwasobserved,withariseof0.04kg/m2
(23.91vs.23.95).Thesamepatternwasobservedinthegroup withBMIfrom 25 to 29.9;the preoperativemean was 27.1 and the postoperative mean was 27.12, i.e. an increase of 0.02kg/m2. Conversely,adownward trend wasobserved in
those withpreoperative BMIgreater than 30kg/m2, with a
fallof0.42kg/m2(31.66vs.31.24).Onceagain,themeanBMI
remainedpracticallyunchanged.
Table1–Stratificationofpatientsbypre-and post-operativebodymassindex.
Pre-operativeclassification Post-operativeclassification
Normalweight (20–25kg/m2):
17
Normalweight(20–25kg/m2):
15
Overweight(25–30kg/m2):2
Obese(>30kg/m2):0
Overweight(25–30kg/m2):
65
Normalweight(20–25kg/m2):2
Overweight(25–30kg/m2):61
Obese(>30kg/m2):2
Obese(>30kg/m2):
9
Normalweight(20–25kg/m2):0
Overweight(25–30kg/m2):2
Obese(>30kg/m2):7
BMI range ; 20-24.9(Pre); 23.91 ; 20-24.9(Post); 23.95 ; 25-29.9(Pre); 27.1 ; 25-29.9(Post); 27.12 ; >30(Pre);
31.66 ; >30(Post); 31.24
IMC
Fig.1–Comparisonbetweenpre-andpostoperativebody massindex(BMI).
Discussion
As observedin thepresent study, therewas no significant reductioninbodymassaftersurgery,and54%ofthepatients presentedweightgain.Ofthe threegroups,onlythegroup ofpatientswithpreoperativeBMIabove30kg/m2presenteda
trendofbodymassreduction.Somestudiesreportedthata post-operativeweightgainofmorethan5%–10%hada nega-tiveimpactonpainandfunction.21,22AccordingtoTeichtahl
etal.,22asignificantpredictorofpostoperativeweightlossis
worsepreoperativefunction.Thepresent studyisin agree-ment with a study published byZeni et al., in which 47% ofthepatientsstudiedpresentedweightgainoneyearafter thesurgicalprocedure.23 Asimilartrendofmaintenanceof
BMIlevelsabovetheidealwasobservedinmenandwomen. Otherstudieshaveobservedagreatertendencyofwomento loseweightpost-surgeryandalowerpropensityformento eitherloseorgainweightinboththepre-andpostoperative periods,inadditiontoalowerpropensityforweightgainin older patients.24,25 Stetsetal.26 alsofoundthat only21.5%
oftheirpatientspresentedareductioninBMI;intheother patients,weightwasmaintained(59.2%)orincreased(19.9%). Regardingobesepatients,Järvenpääetal.27observedalower
lossofperiprostheticbonemineraldensityinthe postopera-tiveperiod,probablyrelatedtoagreaterinducedstressdueto highbodyweight.
Thepresent study corroboratesthe findings retrievedin the literature, in which no significant decrease in BMI is observed.17,18,20
Thelimitationsobservedinthepresentstudyincludethe lackofacontrolgroupanddataonnutrition,physicalactivity level,socioeconomicprofile,andeducationallevelofthe stud-iedpatients.Althoughsomestudiesdidnotshowsignificant differenceintheimpactofpreoperativeweightlosson surgi-calsiteinfectionandhospitalreadmissionrates,28thepresent
study showsthe importanceofthe decreaseinBMI imme-diatelyinthepreoperativeperiod,sincethereisatendency toincreaseormaintainweightamongpatientssubmittedto kneereplacement.5,6
anthropometricmeasurementsinpatientswithBMIbetween 20and30kg/m2;however,inpatientswhowereobesepriorto
surgery,therewasaslighttrendtowardareductioninBMI. The reasons why patients undergoing TKA cannot lose weightneedtobebetterevaluatedandmaybethesubject offuturestudies.
Conclusion
Patients who underwent TKA did not obtain a significant reductionofBMIafterthesurgicalprocedure.Ofthese,46% lostand54%gainedweightinthepostoperativeperiod.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.