REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
SCIENTIFIC
ARTICLE
Influence
of
different
body
positions
in
vital
capacity
in
patients
on
postoperative
upper
abdominal
Bruno
Prata
Martinez
a,b,c,
Joilma
Ribeiro
Silva
c,
Vanessa
Salgado
Silva
c,d,
Mansueto
Gomes
Neto
d,
Luiz
Alberto
Forgiarini
Júnior
e,f,∗aHospitalAlianc¸a,Salvador,BA,Brazil
bEscolaBaianadeMedicinaeSaúdePública(EBMSP),Salvador,BA,Brazil
cFaculdadeSocialdaBahia(FSBA),Salvador,BA,Brazil dUniversidadeFederaldaBahia(UFBA),Salvador,BA,Brazil
eCentroUniversitárioMetodista(IPA),PostgraduatePrograminRehabilitationandInclusionandBiosciencesandRehabilitation,
PortoAlegre,RS,Brazil
fLaboratoryofAirwayandLung,HospitaldeClínicasdePortoAlegre,PortoAlegre,RS,Brazil
Received26March2014;accepted2June2014 Availableonline20February2015
KEYWORDS
Positioningthe patient;
Forcedvitalcapacity; Postoperative complications; Abdominalsurgery
Abstract
Rationale: Thechangesinbodypositioncancausechangesinlungfunction,anditis neces-sarytounderstandthem,especiallyinthepostoperativeupperabdominalsurgery,sincethese patientsaresusceptibletopostoperativepulmonarycomplications.
Objective: Toassessthevitalcapacityinthesupineposition(headat0◦and45◦),sittingand standingpositionsinpatientsinthepostoperativeupperabdominalsurgery.
Methods:Across-sectionalstudyconductedbetweenAugust2008andJanuary2009inahospital inSalvador/BA.Theinstrumentusedtomeasurevitalcapacitywasanalogicspirometer,the choiceofthesequenceofpositionsfollowedarandomorderobtainedfromthedrawofthe fourpositions.Secondarydatawerecollectedfromthemedicalrecordsofeachpatient.
Results:The sample consisted of 30 subjects with a mean age of 45.2±11.2 years, BMI 20.2±1.0kg/m2.Thepositiononorthostasisshowedhighervaluesofvitalcapacityregarding
standing (mean change: 0.15±0.03L; p=0.001), the supine to 45 (average difference: 0.32±0.04L;p=0.001)and0◦(0.50±0.05L;p=0.001).Therewasapositivetrendbetweenthe valuesofforcedvitalcapacitysupinetouprightposture(1.68±0.47;1.86±0.48;2.02±0.48 and2.18±0.52L;respectively).
Conclusion: Bodypositionaffectsthevaluesofvitalcapacityinpatientsinthepostoperative upperabdominalsurgery,increasinginpostureswherethechestisvertical.
© 2014SociedadeBrasileirade Anestesiologia.Publishedby ElsevierEditoraLtda.Allrights reserved.
∗Correspondingauthor.
E-mail:[email protected](L.A.ForgiariniJúnior).
http://dx.doi.org/10.1016/j.bjane.2014.06.002
PALAVRAS-CHAVE
Posicionamentodo paciente;
Capacidadevital forc¸ada; Complicac¸ões pós-operatórias; Cirurgiaabdominal
Influênciadediferentesposic¸õescorporaisnacapacidadevitalempacientesno pós-operatórioabdominalsuperior
Resumo
Justificativa:Asalterac¸õesnoposicionamentocorporalpodemocasionarmudanc¸asnafunc¸ão respiratóriaeénecessáriocompreendê-las,principalmentenopós-operatórioabdominal supe-rior,jáqueospacientesestãosuscetíveisacomplicac¸õespulmonarespós-operatórias.
Objetivo:Verificaracapacidadevitalnasposic¸õesdedecúbitodorsal(cabeceiraa0◦ e45◦), sentadoeemortostaseempacientesnopós-operatóriodecirurgiaabdominalsuperior.
Métodos: Estudotransversal,feitoentreagostode2008ejaneirode2009,emumhospitalna cidadedeSalvador(BA).Oinstrumentousadoparamensurac¸ãodacapacidadevital(CV)foio
ventilômetroanalógicoeaescolhadasequênciadasposic¸õesseguiuumaordemaleatóriaobtida apartirdesorteiodasquatroposic¸ões.Osdadossecundáriosforamcolhidosnosprontuáriosde cadapaciente.
Resultados: Aamostrafoicompostapor30indivíduoscomidademédiade45,2±11,2anose IMC20,2±1,0kg/m2.Aposic¸ãoemortostaseapresentou valoresmaioresdaCVemrelac¸ão
àsedestrac¸ão(médiadas diferenc¸as: 0,15±0,03litros;p=0,001),ao decúbitodorsal a45◦ (médiadasdiferenc¸as:0,32±0,04litros;p=0,001)e0◦ (0,50±0,05litros;p=0,001).Houve um aumentopositivoentreosvalores deCVFdodecúbitodorsal paraaposturaortostática (1,68±0,47;1,86±0,48;2,02±0,48e2,18±0,52litros;respectivamente).
Conclusão:Aposic¸ãodocorpoafetaosvaloresdaCVempacientesnopós-operatóriodecirurgia abdominalsuperior,comaumentonasposturasemqueotóraxencontra-severticalizado. ©2014SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
Upper abdominal surgical procedures account for a large number of postoperative pulmonary complications (PPC) because these procedures directly interfere with lung mechanics and tend to induce restrictive ventilatory dis-orders, as well as reflex inhibition of phrenic nerve and consequentdiaphragmaticdysfunction.1---3Duringearly
post-operative period, patients may present hypoventilation
relatedtothe anestheticprocess,aswellaslimiting ven-tilatorychangesduetopaininsurgicalsite.4
TheprevalencerateofPPCinupperabdominalsurgery
varies between 17% and 88%.5 These changes are more
marked in laparotomy procedures, but are also seen in
laparoscopicsurgeries.1
Pulmonary functiontests playan importantrole inthe
assessment,diagnosis,quantificationoftheventilatory dis-orders intensity, and treatment course.6 The forced vital
capacity(FVC)isapulmonaryfunctionmeasureoftenused
forthispurposeandisdefinedasthemaximumvolumeofair
exhaledfromaftermaximuminspiration.6,7DecreasedFVC
isafairlyobviousabnormalityinpatients withrespiratory muscleweaknessorchangesinlungmechanicsthatoverload
these muscles.7,8 These decreases after upper abdominal
surgery rangefrom 20% to30% of the preoperative value
andmayachievemoresignificantvaluesupto50%.7,9---11
Changeinbodypositioningandtheconsequentchangeof
gravityeffect,amongotherfactors,causechangein respi-ratoryfunction atdifferentintensities.12 Thus,knowledge
ofthe physiological effectsof different bodypositions on pulmonaryfunctionisessentialtoguidethephysical ther-apyprocedures,includingspirometryinclinicalpractice,so
that itsvalues are comparablebetween different periods
andpatients.13Therefore,theobjectiveofthisstudywasto
investigatethefunctionalvitalcapacityinthesupine(head at0◦and45◦),sittingonthebedwithhangingdownlegs,and
uprightpositionsinpatientsafterupperabdominalsurgery.
Method
Cross-sectional study conducted in the wards of Hospital
Santo Antônio ---Obras SociaisIrmãDulce, Salvador, Bahia State,acityreferenceinabdominalsurgery.
Patientsagedover18years,onthesecondpostoperative
day of upper abdominal surgery, with history of previous
functional independence and medical release and
stand-up were included. Exclusion criteria were patients with
irreversiblepainwithpainkillers,neurologicaland/or
cogni-tiveimpairmentthatpreventedtheFVCmeasurementand
adecreaseinbloodpressuregreaterthan20%frombaseline duringpositionchange.
The study was approved by the Research Ethics
Com-mitteeofthehospital,protocolnumber40/06.Allpatients
signedaninformedconsentform(ICF).
DatacollectionwasconductedfromAugust2008to
Jan-uary 2009. Forced vital capacity (FVC) measurement was
defined according to the 2002 guidelines for pulmonary
function tests.6 The toll used for this measurement was
the analog spirometer (Ferraris --- Mark 8 Respirometer
Wright,Louisville,CO,USA)coupledtoasiliconfacemask.
The sequence of positions was randomized by blocks of
envelopes.Subsequently,subjectswereplacedinselected
Table 1 Demographic data of patients included in the study.
Mean±SD Percentage(n)
Age(years) 45.2±11.2
BMI(kgm−2) 20.2±1.0
Tipo
ELcholecystectomy 16.7(5)
VLCcholecystectomy 50.0(15)
Nephrectomy 10.0(3)
Gastrectomy 3.3(1)
Pancreaticoduodenectomy 16.7(5)
Cystectomy 3.3(1)
EL,exploratorylaparoscopic;VLC,videolaparoscopic.
lung capacity (TLC) followed by a maximal expiration to residualvolume(RV). The vitalcapacity valueadopted in eachpositionwasthehighestvalueamongthree measure-mentswithlessthan10%differencebetweenthem.Thefour positionsusedinthepresentstudyweresupineat0◦,supine
at45◦sittingwithhangingdownlegs,andupright.All
mea-surementswereperformedbythesameinvestigator.Clinical datawereobtainedthroughmedicalrecordsofeachpatient. Meanandstandarddeviationwereusedtorepresentthe FVCvaluesobtainedinbodypositionsanalyzed.Analysisof Variance(ANOVA)withposthocBonferronitestwasusedto comparethemeanvaluesofFVCbetweeneachbody posi-tion.AllanalyseswereperformedusingSPSSversion14.0.
Results
The population consisted of 30 subjects, mean age of 45.2±11.2 years,BMIof 20.2±1.0kgm−2,predominantly
female(76.7%).Table1showsthedemographic character-isticsandoperationsperformed.ValuesofFVCindifferent positionsareshowninTable2.Thehighest valueobtained
was for the upright position (FVC 2.18±0.52; 95% CI
1.99---2.37).
Compared withtheother threepositions,upright
posi-tionshowedsignificantlyhighervaluesinrelationtositting (meanofdifferences:0.15±0.03;p=0.001),supineat45◦
(meanofdifferences:0.32±0.04;p=0.001),andsupineat 0◦(0.50±0.05;p=0.001).Therewerealsosignificant
differ-encesbetweenthesittingpositionwithhangingdownlegs
andsupinepositionat45◦(meanofdifferences:0.17±0.04;
Table2 Evaluation oftheforced vitalcapacity (FVC)in liters (L)indifferent body positions,with 95%confidence interval(95%CI).
Bodyposition Mean Standard
deviation
Confidence interval(95%CI)
Supine(0◦) 1.68 0.47 1.51---1.85
Supine(45◦) 1.86 0.48 1.68---2.04
Sitting 2.02 0.48 1.84---2.21
Upright 2.18 0.52 1.99---2.37
Dataare expressedasmeanandstandarddeviationofforced vital capacity (FVC) in liters (L) in different body positions (n=30).
2.20
2.10
2.00
1.90
1.80
1.70
1.60
Forced vital capacity (liters)
1 2 3 4
Body positions: 1) dorsal decubitus at 0°; 2) dorsal decubitus at 45°; 3) sitting with hanging legs; 4) upright.
Figure1 MeanVC(L)indifferentpositions:(1)dorsal decu-bitusat0◦;(2)dorsaldecubitusat45◦;(3)sittingwithhanging legs;and(4)upright.
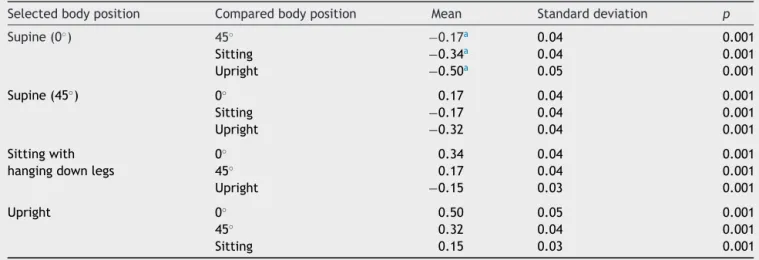
p=0.001) and at 0◦ (mean of difference: 0. 34±0.04; p=0.001),aswell asbetween supineat45◦ and0◦ (mean
difference:0.17±0.04;p=0.001)(Fig.1).Therewasa
pos-itivetrendbetween supineFVCvalues touprightposition
(Table3).
Discussion
The present study found that FVC increases progressively
betweensupineat0◦anduprightpositionsinpatientsafter
upperabdominalsurgery.Thisisthefirststudytoevaluate
respiratory mechanics throughVC in this type of surgical
patients,whichissomewhatrelevant,astheuppersurgeries
predisposetocomplicationsandpositioningmayminimize
someventilatorychanges.
Compared to other positions evaluated in this study,
therewasagreaterdecreaseinFVCinsupinepositionat0◦,
afindingthatisinagreementwiththatofotherstudies.14,15
Thisdecreasemaybeattributedtodecreaseddynamiclung
compliance and increased resistance to pulmonary blood
flow, resulting from reduced FRC in this position.15,16 In
supineposition,anatomicalchangesoccurinthepharynx,
suchasthereductionofitsdiameter,whichincreasesthe
upperairwayresistance.Thecephalicdisplacementofthe
diaphragm due to increased abdominalpressure, and the
increasedintrathoracicbloodvolume,arealsofactorsthat resultinreducedlungvolumeatrestandjustifyanincrease inairwayresistanceinthisbodyposition.15
In the present study, the sitting position showed an
increaseof20.2%inFVCcomparedtosupineposition.This
finding corroborates other studies that showed increased
FVCin this positionranging from4.6% to 20% in patients
undergoingabdominalprocedure.14---17 This findingmaybe
Table3 Comparisonofforcedvitalcapacity(FVC)inliterswithmeandifferencesbetweendifferentbodypositions(n=30).
Selectedbodyposition Comparedbodyposition Mean Standarddeviation p
Supine(0◦) 45◦ −0.17a 0.04 0.001
Sitting −0.34a 0.04 0.001
Upright −0.50a 0.05 0.001
Supine(45◦) 0◦ 0.17 0.04 0.001
Sitting −0.17 0.04 0.001
Upright −0.32 0.04 0.001
Sittingwith hangingdownlegs
0◦ 0.34 0.04 0.001
45◦ 0.17 0.04 0.001
Upright −0.15 0.03 0.001
Upright 0◦ 0.50 0.05 0.001
45◦ 0.32 0.04 0.001
Sitting 0.15 0.03 0.001
aSignificantdifference(p<0.05).
and overcomes the tendency to airway closure related
tochanges in lung complianceand lower pressure of the
abdominalorgansinrelationtothediaphragm.18
TheuprightpositionshowedthehighestincreasesinFVC. Asimilarfindingwasreportedbyotherauthorswhosuggest thattheuprightpositionprovidesgreatermechanical
advan-tagetotherespiratorymuscles, asabdominalcontentsdo
notinterferewithdiaphragmdisplacementand,thus,
gen-erateshigher ventilation pressures.19,20 In contrast,Costa
etal.andDomingos-Benícioetal.foundnostatistically sig-nificantdifferenceinFVCbetween thesittingandupright
positions, but these studies were conducted with a
non-surgical, healthy, and young population.17,21 According to
Pereira et al., FVC in adults and elderly is higher in the upright position (1---2%) and lower in the supine position
(7---8%) compared to the sitting position, which does not
occurinyoungerpeople.6
The main explanationfactorfor the increasein FVCin
amorevertical chestpositionis thepossible reductionin transthoracic pressure, as even in the 45◦ position there
isless compressiveeffectoftheabdominalwall, whichis greaterinthe0◦ horizontalposition.Valenzaetal.
demon-stratetheimpactof increasedpleural pressureunderthe
diaphragm,astheforceexertedontheTrendelenburg posi-tionwashighercomparedwiththesittingposition,16which
was also shown in a study by Behrakis et al. regarding
compliance.15
AnotherexplanationforFVCreductioninsupineposition at0◦maybeduetothereductioninalveolararea,andnot
onlybytheincreasedfrequencyofatelectasis,asreported byPankowetal.22However,inthepresentstudythis
find-ingwasnotevident sincethereducedFVC maybedue to
inhibitionofphrenicnervereflexandnotnecessarilytothe
increased respiratory system elastance by the abdominal
surgicaltrauma.
The upper abdominal surgery induces a
diaphrag-matic dysfunction lasting for about a week and may
be a major cause of postoperative pulmonary restrictive
pattern.2Reduceddiaphragmaticfunctionmaybe
responsi-bleforatelectasis,reducedvitalcapacity,andhypoxemia.3
Althoughanesthesiaandpainmayberesponsiblefor respira-torymuscledysfunction,studiessupportthehypothesisthat aninhibitoryreflexduetotheabdominalcavity manipula-tionisthemainmechanism.1---3,23---25Therefore,thelowFVC
valuesseeninpatientsinthepresentstudyindifferent
pos-itions maybedue todiaphragmatic dysfunctionmediated
byreflexmechanismofafferentphrenicnerveinhibition.
Thus, knowledge of body positions that favor lung
function can be used as a therapeutic measure, aiming
at improving lung volume, oxygenation, and respiratory
mechanicsandminimizingdisturbancesproducedbymajor
surgical procedures,withreducedincidenceofatelectasis andpreventionofpulmonarycomplications.16,26---29
Thisstudyhassomelimitations,suchasthelackof intra-abdominalpressure(IAP)measurement,asitselevationmay bepresentafterabdominalsurgeryandgeneratechangesin
spirometricdata.However,IAPmeasurementisaninvasive
procedure requiring specializedprofessional,which would
hinderthestudyconduction.Anotherpossiblelimitationis
the use ofa facemask asa measuringtool insteadof the
nozzle.AccordingtoFioreetal.,30 VCevaluationsmaybe
done using a facemask without interfering in the results
and become accessible topatients whohave difficulty in
performingtheevaluation,aslippressurebecomes
unnec-essary.
Conclusion
Body position affects VC values in patients after upper
abdominalsurgery,withanincreaseinpostureswherethe
chestismoreverticallypositioned.Themostfavored respi-ratoryfunction is inthe uprightposition, followedby the sittingposition,comparedwiththesupinepositionat0◦and
45◦.
Conflicts
of
interest
References
1.Erice F, Fox GS, Salib YM, et al. Diaphragmatic function beforeandafterlaparoscopiccholecystectomy.Anesthesiology. 1993;79:966---75.
2.SimonneauG,VivienA,SarteneR,etal.Diaphragmdysfunction inducedbyupperabdominalsurgery.Roleofpostoperativepain. AmRevRespirDis.1983;128:899---903.
3.FordGT,WhitelawWA,RosenalTW,etal.Diaphragmfunction afterupperabdominalsurgeryinhumans.AmRevRespirDis. 1983;127:431---6.
4.ArozullahAM, Conde MV,Lawrence VA. Preoperative evalua-tionforpostoperativepulmonarycomplications.MedClinNAm. 2003;87:153---73.
5.OverendTJ,AndersonCM,LucySD,etal.Theeffectofincentive spirometryonpostoperativepulmonarycomplications.Chest. 2001;120:971---8.
6.Sociedade Brasileira de Pneumologia e Tisologia. Diretrizes paratestes de func¸ãopulmonar. J Pneumol. 2002;28 Suppl. 3:S1---238.
7.GibsonJ,WhitelawW,SiafakasN.Testsofoverallrespiratory function.AmJRespirCritCareMed.2002;166:521---6.
8.ChevroletJC,DeleamondP.Repeatedvitalcapacity measure-mentsaspredictiveparametersformechanicalventilationneed andweaningsuccessinGuillain---Barrésyndrome.AmRevRespir Dis.1991;144:814---8.
9.Frazee RC, Roberts JW, Okeson GC, et al. Open versus laparoscopiccholecystectomy.Acomparisonofpostoperative pulmonaryfunction.AnnSurg.1991;213:651---3.
10.Hasuki´c S, Mesi´c D. Postoperative pulmonary changes after laparoscopiccholecystectomy.MedArh.2001;55:91---3.
11.Ravimohan SM, Kaman L, Jindal R, et al. Postoperative pulmonaryfunction in laparoscopicversus open cholecystec-tomy:prospective,comparativestudy.IndianJGastroenterol. 2005;24:6---8.
12.GeaJ.La especie humana: unlargocamino para elsistema respiratorio.ArchBronconeumol.2008;44:263---70.
13.WallaceJL,GeorgeCM,TolleyEA,etal.Peakexpiratoryflowin bed?Acomparisonof3positions.RespirCare.2013;58:494---7.
14.Meysman M, Vincken W. Effect of body posture on spiro-metric values and upper airway obstruction indices derived fromtheflow-volumeloopinyoungnonobesesubjects.Chest. 1998;114:1042---7.
15.Behrakis PK, Baydur A, Jaeger MJ, et al. Lung mechan-ics in sittingand horizontal bodypositions. Chest. 1998;83: 643---6.
16.Valenza F, Vagginelli F, Tiby A, et al. Effects of the beach chair position, positive end-expiratory pressure, and
pneumoperitoneumonrespiratoryfunction inmorbidlyobese patients during anesthesia and paralysis. Anesthesiology. 2010;107:725---32.
17.Domingos-Benício NC, Gastaldi AC, PerecinJC, et al. Medi-dasespirométricasempessoaseutróficaseobesasnasposic¸ões ortostática,sentada.RevAssocMedBras.2004;50:142---7.
18.TsubakiA,DeguchiS,YonedaY.Influenceofpostureon respi-ratory function and respiratory muscle strength in normal subjects.JPhysTherSci.2009;21:71---4.
19.TownsendMC.Spirometricforcedexpiratoryvolumemeasured inthestandingversusthesittingposture.AmRevRespirDis. 1984;130:123---4.
20.GudmundssonG,CervenyM,ShasbyDM.Spirometricvaluesin obeseindividuals.Effectsofbodyposition.AmJRespirCritCare Med.1997;155:998---9.
21.CostaGM,LimaJGM,LopesAJ.Espirometria:ainfluênciada posturaedoclipenasaldurantearealizac¸ãodamanobra. Pul-mão.2006;15:143---7.
22.PankowW,PodszusT,GutheilT,etal.Expiratoryflowlimitation andintrinsicpositiveend-expiratorypressureinobesity.JAppl Physiol.1998;85:1236---43.
23.VassilakopoulosT,MastoraZ,KatsaounouP,etal.Contribution ofpaintoinspiratorymuscledysfunctionafterupperabdominal surgery.Arandomizedcontrolledtrial.AmJRespirCritCare Med.2000;161:1372---5.
24.SprungJ,ChengEY,NimphiusN,etal.Diaphragmdysfunction and respiratoryinsufficiency after upper abdominal surgery. PlucneBolesti.1991;43:5---12.
25.Dureuil B, ViiresN, Cantineau JP, et al. Diaphragmatic con-tractility after upper abdominal surgery. J Appl Physiol. 1986;61:1775---80.
26.DeanE.Effect ofbodyposition onpulmonary function.Phys Ther.1985;65:613---8.
27.Tucker B, Jenkins S. The effectof breathing exercises with body positioning on regional lung ventilation. Aust J Phys. 1996;42:219---27.
28.LunardiAC,ResendeJM,CerriOM,etal.Efeitodacontinuidade dafisioterapiarespiratóriaatéaaltahospitalarnaincidência de complicac¸ões pulmonaresapósesofagectomiapor câncer. FisioterPesqui.2008;15:72---7.
29.Franc¸a EET, Ferrari F, Fernandes P, et al. Fisioterapia em pacientescríticosadultos:recomendac¸õesdoDepartamentode FisioterapiadaAssociac¸ãodeMedicinaIntensivaBrasileira.Rev BrasTerIntensiv.2012;24:6---22.