REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
SCIENTIFIC
ARTICLE
Effectiveness
of
dexmedetomidine
for
emergence
agitation
in
infants
undergoing
palatoplasty:
a
randomized
controlled
trial
Aiji
Boku
a,∗,
Hiroshi
Hanamoto
a,
Aiko
Oyamaguchi
a,
Mika
Inoue
a,
Yoshinari
Morimoto
b,
Hitoshi
Niwa
aaDepartmentofDentalAnesthesiology,GraduateSchoolofDentistry,OsakaUniversity,Osaka,Japan bSpecialPatientOralCareUnit,KyushuUniversityHospital,Fukuoka,Japan
Received29October2014;accepted7January2015 Availableonline31March2015
KEYWORDS
Dexmedetomidine; Sevoflurane; Palatoplasty; Agitation; Infant;
Postoperativepain
Abstract
Objectives: Ininfants,thereisahighincidenceofemergenceagitation(EA)aftersevoflurane
(Sev)anesthesia.Thisstudyaimedtotestthehypothesisthatdexmedetomidine(Dex)
admin-istrationwouldreducetheincidenceandseverityofEAafterSev-basedanesthesiaininfants
undergoingpalatoplasty.
Methods:Aprospectiverandomizedclinicaltrialwasconductedwith70patientsundergoing
palatoplasty,aged10---14months.Infantswererandomlyallocatedintotwogroups:Dex(n=35)
andsaline(n=35).IntheDexgroup,Dex(6g/kg/h)wasadministeredapproximately10min
beforetheendofthesurgeryfor10min,followedby0.4g/kg/huntil5minafterextubation.In
thesalinegroup,anequivalentamountofsalinewasadministeredinasimilarmanner.Afterthe
surgery,patientsweretransferredtothepostanestheticcareunit(PACU).Theinfant’sbehavior
andpainwereassessedwithscoringsystemforEA(5-pointratingscale)andpainscale(PS;
10-pointratingscale),respectively.EAandPSwereestimatedatsixtimepoints(afterextubation,
leavingtheoperatingroom,0,30,60,and120minafterarrivalinPACU).
Results:EA andPSscoresweresignificantlylowerintheDexgroupthaninthesalinegroup
fromextubationto120minafterarrivalinPACU.
Conclusions: DexadministrationhastheadvantageofareducedEAandPSwithoutanyadverse
effects.Dexprovidedsatisfactoryrecoveryininfantsundergoingpalatoplasty.
© 2015SociedadeBrasileirade Anestesiologia.Publishedby ElsevierEditoraLtda.Allrights
reserved.
∗Correspondingauthor.
E-mail:[email protected](A.Boku).
http://dx.doi.org/10.1016/j.bjane.2015.01.001
PALAVRAS-CHAVE
Dexmedetomidina; Sevoflurano; Palatoplastia; Agitac¸ão; Bebê;
Dorpós-operatória
Eficáciadedexmedetomidinaparaosurgimentodeagitac¸ãoemlactentessubmetidos àpalatoplastia:estudoclínicorandomizado
Resumo
Objetivos: Emcrianc¸as,é elevadaa incidênciade surgimento deagitac¸ão (SA)em seguida
àanestesiacomsevoflurano(Sev).Esteestudotevecomo objetivotestarahipótesedeque
a administrac¸ão de dexmedetomidina (Dex) reduziria a incidência e gravidade do SAapós
anestesiacomSevemlactentessubmetidosàpalatoplastia.
Métodos: Estudoclínicoprospectivorandomizado,realizado com70pacientessubmetidosa
uma palatoplastia, com idadesentre 10-14 meses. Ascrianc¸as foram divididas
randomica-menteemdoisgrupos:Dex(n=35)esoluc¸ãosalina(n=35).NogrupodeDex,Dex(6g/kg/h)
foi administradacerca de10 minutosantes dofinaldacirurgia durante10min,seguidade
0,4g/kg/h até5 minutosapós aextubac¸ão.No grupo de soluc¸ão salina, uma quantidade
equivalentedesalinafoiadministradacomomesmoesquemadedosagem.Apósacirurgia,os
pacientesforamtransferidosparaaunidadedecuidadospós-anestésicos (UCPA).O
compor-tamentoeadordosbebêsforamavaliadoscomumsistemadepontuac¸ãoparaSA(escalade
classificac¸ãode5pontos)ecomumaescaladedor(ED;escaladeclassificac¸ãode10pontos),
respectivamente.SAeEDforamestimadosemseispontoscronológicos(apósaextubac¸ão,ao
deixarasaladecirurgia,e0,30,60e120minutosapósachegadaàUCPA).
Resultados: OsescoresSAeEDforamsignificativamentemenoresnogrupoDexversusgrupo
salina,desdeaextubac¸ãoaté120minapósachegadaàUCPA.
Conclusões:Aadministrac¸ãodeDextemavantagemdeumareduc¸ãonoSAenaED,sem
quais-querefeitosadversos.Dexproporcionouumarecuperac¸ãosatisfatóriaemlactentessubmetidos
àpalatoplastia.
©2015SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos
direitosreservados.
Introduction
Sevoflurane(Sev)isapopularinhalationalanestheticin chil-dren.Itis characterizedbya morerapidonsetandoffset becauseof a lowerblood/gas partitioncoefficient, a less pungentandirritation tothe airway,and aless cardiode-pressiveeffectwhencomparedwithother potent inhaled anesthetics.1,2However,theincidenceofemergence
agita-tion(EA)afterSevanesthesiaishighininfants,3,4andthe
etiologyforthehigherincidenceofEAininfantsisunknown.
EA is not only a major source of dissatisfaction for
par-entsandcaregiverspostoperatively,butitalsomayleadto
somecomplicationssuchasincreasedbleedingfrom
opera-tivesitesandpullingoutanintravenouscatheter.Possible
etiologicalfactorsforEAincludearapidrecovery,
psycho-logical immaturity, otolaryngology procedures, anesthesia
time,and concurrent medications.5---8 Pediatric
anesthesi-ologistsshould considermethods toreduce therisk of EA
afterSevanesthesia.
Inthepresentstudy,wefocusedonEAinspecificpatients
agedapproximately1year(10---14months)andundergoing
palatoplastyformorereliableresultsbecausetheincidence
andseverityofEAdependsonpatient’sageandprocedure.9
Otolaryngologyproceduressuch astonsillectomy and
ade-noidectomyaswell aschildren arerisk factorsforEA.10 A
senseof suffocation in airwayprocedures is considered a
majorcauseofthehighincidenceofEA.
The immediatepostoperative periodafterpalatoplasty
isdifficult because thissurgery hasspecific complications
associated with the surgical procedure. Severe pain is
suspected and narrowing of the upper respiratory tract
mayresultintransientworseningofobstructivesymptoms
and hypoxemia. Because EA after palatoplasty is a mild
complicationincomparisonwithlingualswellingandother
airway-relatedcomplications,11rapidemergencefrom
anes-thesiamaybedesirabletoallowforfullairwaycontrolafter
extubation. Therefore,it is important thatprophylaxis or
treatmentforEAafterpalatoplastyshouldnothavean
unfa-vorableimpactonairway.
Various medications, including benzodiazepines,
keta-mine,andpropofol,wereusedtoreduce theincidenceof
EA.12 However,thereis nowell-established prophylaxisor
treatment for EA. Although supplemental opioids and/or
sedatives are often used to reduce the incidence and
severityofEA,anesthesiologistsshouldalwaysconsiderthe
riskofpostoperativerespiratorycomplications.
Dexmedetomidine (Dex), a potent ␣2-adrenoceptor
agonist, has sedative, analgesic, and anxiolytic
proper-ties without respiratory depression.13 Some studies have
shown the effectiveness of Dex in postoperative
recov-eryinapediatricpopulationundergoingtonsillectomyand
adenoidectomy.14,15 However, the effectiveness of Dex in
younger infants undergoingpalatoplasty has notyet been
wellestablished.
Theobjectiveofthisstudywastotestthehypothesisthat
theadministrationofDexwouldreducetheincidenceand
severityofEAafterSev-basedanesthesiaininfants
Materials
and
methods
This randomized anddouble-blind study was approvedby
theInstitutionalEthicalCommitteeofOsakaUniversity
Den-talHospital,Suita,Japan(ChairpersonProf.S.Wakisaka)on
August 23,2011 and theprotocol number is H23-E9.
Reg-istrationfor this study(UMIN000009869) can befound at
http://upload.umin.ac.jp. Patient’s parents were advised
about the risk and benefits of participation and written
informedconsentwasobtained.
Patients
Seventypatientsundergoingpalatoplastywereenrolledin
this study. Participants were required tobe ASA physical
status class I, aged 10---14 months old, weight between
7 and 10kg. Exclusion criteria included lack of consent,
ASA class>II, cardiovascular disease, or a history of
air-way obstruction. Randomization was performed using a
computer-generatedrandomnumbertable.Five
anesthesi-ologistsparticipatedinthisstudy,andeachhadover7years’
experience.The patient’sparentsandtheattending
anes-thesiologistwereblindedtothegroupallocation.Patients
wererandomlyallocatedintotwogroups:Dex(n=35)and
saline(n=35).
Anesthesiaprotocol
Afterstandard monitoring (includingpulseoximetry,
elec-trocardiogram, noninvasivearterial blood pressure)in the
operating room, anesthesia was induced with Sev (4%).
After induction, endotracheal intubation was facilitated
with0.6mg/kgrocuronium.Anesthesiawasmaintainedwith
1%---2%end-tidalSevand66%nitrousoxideinoxygen.
Fen-tanyl (20g) was administered as a bolus to patients in
bothgroups,andlocalanesthetics(1%lidocainecontaining
adrenalin:2ml)wasalsoinjectedintotheoperativesite.In
theDex group,Dex(6g/kg/h)wascontinuously
adminis-teredapproximately10minbeforetheendofthesurgeryfor
10min,followedby0.4g/kg/huntil5minafterthe
extu-bation.Inthesalinegroup,anequivalentamountofsaline
was administered in a similar manner. At the end of the
surgery, anesthetic gases were discontinued. The trachea
wasextubated when patients were awake. Patients were
then transferred to the postanesthetic care unit (PACU),
andboth groups receivedrectalacetaminophen (200mg).
InPACU,parentswereallowedtobewiththeirchild.
Sup-plementaloxygen wasadministeredwhenSpO2 decreased
tolessthan95%.
Table1 Scoringsystemforemergenceagitation.
Score Behavior
1 Sleeping
2 Awake,Calm
3 Irritable,crying
4 Inconsolablecrying
5 Severerestlessness,disorientation
Weevaluatedtimetoextubation(TE),whichwasdefined asthetimefromdiscontinuationofSevandnitrousoxideto extubation.Heartrate(HR),meanarterial bloodpressure (MAP),andSpO2weredocumentedbefore,undergoing,and aftertheadministrationofDexor saline.ToassesstheEA and painscale (PS) score, the scoring system for EA and PSscorewere used.EAwasassessed witha5-point scale (Table1).5PSscorewasassessedbyFace,Legs,Activity,Cry,
Consolability(FLACC)Scale(Table2).16Thispainassessment
scalewasusedfornonverbalpatients.Eachscalehasthree
categories.Weaddedeachscale andexpresseditastotal
points.EAand PSscorewereestimatedat sixtimepoints
(afterextubation,leavingtheoperatingroom,0,30,60,and
120minafterarrivalinPACU).Dataforeach patientwere
obtainedbytheblindedanesthesiologist.
Statisticalanalysis
Beforeinitiatingthestudy,apoweranalysissuggestedthat
a sample size of 35 patients in each groups are required
toshowthattheadministrationofDexwoulddecreasethe
incidenceofsevere EA(point 4or 5)afterthe surgeryby
40%with80%power(˛=0.05)incomparisonwiththecontrol
group.
Dataarepresentedasnumber(n),mean(SD),ormedian
(IQR)asappropriate.Student’st-testwasusedforheight,
weight,age, anesthesia time,surgery time, and TE.
Chi-squarefor independence test2×2contingency table was
used for sex. Two-factor repeated-measures ANOVA and
multiplecomparison wasusedfor HRandMAP. EA andPS
scorewerecomparedbetweengroupswithMann---Whitney’s
U-test. p-valuesof<0.05wereconsideredstatistically
sig-nificant.
Results
Eighty infants presenting withpalatoplasty under general
anesthesiawereassessedforeligibilityfromAugust2011to
July2012. Fig.1 shows theCONSORT flow chartdetailing
Table2 Scoringsystemforpainscale.
Category Score0 Score1 Score2
Face Noparticularexpressionorsmile Occasionalgrimace Frequenttoconstantfrown
Legs Normalposition Uneasy,restless Kickingorlegsdrawnup
Activity Lyingquietly,moveseasily Squirming,shiftingback Archedrigid
Cry Nocrying Moansorwhimpers Cryingsteadily,screams
Consolability Content,relaxed Reassuredbyoccasionaltouching,hugging Difficulttoconsole
Enrollment
Assessed for eligibility (n=80)
Randomized (n=70)
Excluded (n=10)
Not meeting inclusion criteria (n=2)
Declined to participate (n=8)
Allocated to intervention (n=35)
Received allocated intervention (n=35)
Did not receive allocated intervention (give reasons) (n=0)
Lost to follow-up (give reasons) (n=0)
Discontinued intervention (give reasons) (n=0)
Analysed (n=35)
Excluded from analysis (give reasons) (n=0)
Analysed (n=35)
Excluded from analysis (give reasons) (n=0) Lost to follow-up (give reasons) (n=0)
Discontinued intervention (give reasons) (n=0)
Did not receive allocated intervention (give reasons) (n=0)
Allocated to intervention (n=35)
Received allocated intervention (n=35)
Figure1 ConsolidatedStandardsofReportingTrials(CONSORT)recommendeddescriptionofpatientrecruitment.
patientrecruitment. Dataanalysis wasperformed on two groups(Dexgroup,n=35;salinegroup,n=35).
Detailsofdemographiccharacteristicsaresummarizedin Table3.Therewerenodifferencesbetweenthetwogroups
inpatientdemographics,surgerytime,andanesthesiatime.
TotaldosageofDexwas11.5(2.5)g.TEwassignificantly
longerin the Dex group [8.1 (2.9)min] than in thesaline
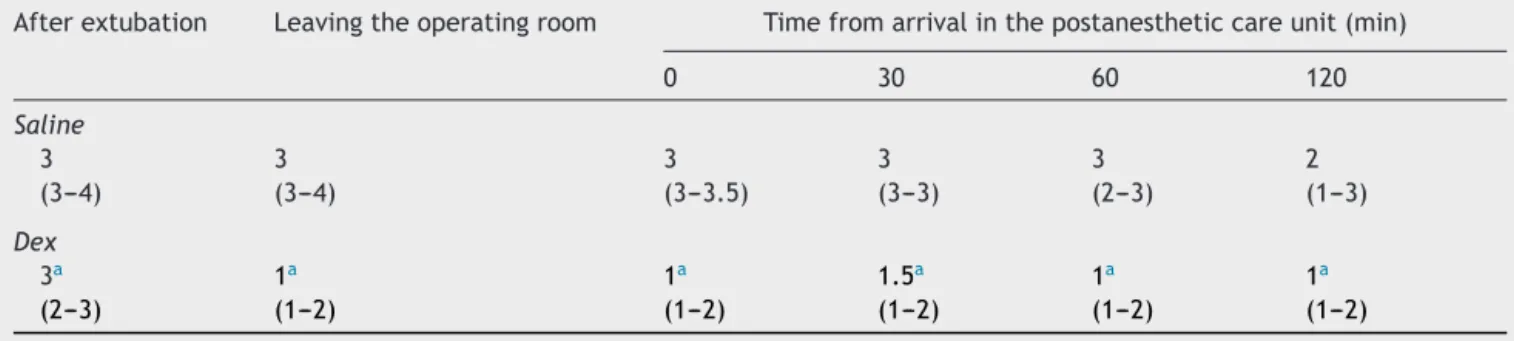
group[6.4(1.9)min].Tables4and5demonstratedthe
sco-ring system for EA and PS score. EA and PS scores were
significantlylowerintheDexgroupthaninthesalinegroup
duringtheobservationperiod.
Twopatientsin eachgrouprequired supplemental
oxy-gen becauseof reducedSpO2 (Table 6);however, none of
thesepatientsexhibitedanysignsofairwayobstructionand
prolongedoxygenrequirement.
MAP and HR after extubation (after administration of
Dex) were significantly lower in the Dex group [59.7
(5.3)mmHg, 128.1(9.8)beats/min, respectively] than in
the saline group [67.3(6.6)mmHg, 142.5(9.7)beats/min,
respectively].Hemodynamicinstabilitydidnotoccurinany
ofthepatients,andvitalsignsremainedwithin20%of
base-lineinallpatients(Figs.2and3).
Table3 Demographicdata.
Dex(n=35) Saline(n=35) pvalue
Patientcharacteristics
Age(month) 12.2(1.5) 11.9(1.6) 0.44NS
Male/Female 14/22 16/19 0.21NS
Height(cm) 74.9(3.1) 74.0(3.8) 0.23NS
Weight(kg) 8.8(1.0) 8.9(1.2) 0.32NS
Surgerycharacteristics
Surgerytime(min) 76.5(22.2) 74.5(15.1) 0.18NS
Anesthesiatime(min) 148.5(19.8) 143.0(25.0) 0.39NS
TE(min)a 8.1(2.9) 6.4(1.9) 0.01
TotalamountofDex(g) 11.5(2.5)
Dataareexpressedbymean(SD);NS,notsignificant.
Table4 Thescoringsystemforemergenceagitationatsixpointsoftime.
Afterextubation Leavingtheoperatingroom Timefromarrivalinthepostanestheticcareunit(min)
0 30 60 120
Saline
3 3 3 3 3 2
(3---4) (3---4) (3---3.5) (3---3) (2---3) (1---3)
Dex
3a 1a 1a 1.5a 1a 1a
(2---3) (1---2) (1---2) (1---2) (1---2) (1---2)
Dataareexpressedasmedian(IQR).
a p<0.05;Dexvs.saline.
Table5 Thescoringsystemforpainscaleatsixpointsoftime.
Afterextubation Leavingtheoperatingroom Timefromarrivalinthepostanestheticcareunit(min)
0 30 60 120
Saline
9 8 8 6 5 5
(8---9) (7---9) (6---9) (5---8) (3.5---6) (3.5---6)
Dex
7a 1a 1.5a 2a 1a 0a
(2.75---9) (0---4.25) (0---4) (0---3.25) (0---2.25) (0---2)
Dataareexpressedasmedian(IQR).
a p<0.05;Dexvs.saline.
Table6 DesaturationepisodewithSpO2below95%after
extubation.
Saline 2/35
Dexmedetomidine 2/36
Discussion
Theresults ofthisstudyshowthatDex hastheadvantage ofa reducedEAandPSscorewithout anyadverse effects
Map
Before administration
Under administration
After administration
Dex Saline 0
20 40 60 80
MAP mmHg
Figure2 Meanarterialbloodpressure(MAP)responsesatthe
timeofbefore,undergoing,afteradministrationof
dexmedeto-midine (Dex) or saline.Data aremean (SD). *p<0.05versus
beforeadministration.
afterSevanesthesiaininfantsundergoingpalatoplasty.The effectsonEAandPSscorelastedformorethan2hafterthe surgery.
Dex is a potent ␣2-adrenoceptor agonist and primar-ily used as a postoperative sedative in ICU.17 Recently,
Dex is increasingly used for procedural sedation during
awakefiberopticintubation,18colonoscopy,19 andmagnetic
resonance imaging (MRI) for young children.20---22 Dex is
also extremely useful as a sedative for children
under-going tonsillectomy and adenoidectomy.10 These reports
suggestapossiblebeneficialeffectofDexforpostoperative
managementafterpalatoplasty. The present studyclearly
HR
Before administration
Under administration
After administration
Dex Saline 0
40 80 120 160
HR beats/min
demonstratedtheeffectivenessofDexonthereductionin
EAscore.
Pain is a major factor increasing the severity and
fre-quencyof agitation, and sufficient analgesia leads tothe
reductioninagitation.23,24 Dexisbeneficialforpain
treat-ment.Dexdemonstratesperipheralandcentrallymediated
antinociceptionvia receptor activation in the dorsal horn
andthe locuscoeruleus.25,26 Dex administered beforethe
endofsurgeryreducedmorphinerequirementinthe
imme-diate postoperative period in adult patients undergoing
majorabdominalororthopedicprocedures.27 Pateletal.14
also reported that an intraoperative infusion of Dex
sig-nificantlyreducedthepostoperativeopioidrequirementin
children. Our PS score results indicate that Dex provides
considerableanalgesiafollowingpalatoplasty.
Somestudieshavedemonstratedthatopioidsare
effec-tivetorelieve EAafter Sev anesthesia.28 However,in the
postoperativeperiodfollowingpalatoplasty,effective
anal-gesiawithopioidalonewouldbedifficulttoprovidewithout
anyeffectsonairway.Incontrast,thereareevidencesthat
evenpain-freechildrenwithcaudalblockorundergoingMRI
becomeagitatedduringemergencefromanesthesia.29,30EA
oftenoccursevenafter adequatepain treatmentor after
proceduresthatarenotassociatedwithpain.BecauseDex
hasboth sedativeandanalgesicproperties,itisbeneficial
eveninsuchsituations.
Dex can leadtodose-dependent bradycardia, hypo-or
hypertension in children, when Dex is applied as a sole
agent for sedation.31,32 Bloor et al.33 reported that after
the administrationof Dex, there is a decrease in the HR
and biphasic blood pressure response with a short
ini-tial increase, followed by a prolonged decrease of the
bloodpressure.ThedecreaseinbloodpressureandHRare
the result of the stimulation of central presynaptic ␣2a
-adrenergicreceptor.31,33
Inthisstudy,Dexwasadministeredatanintraoperative
initial loadingdose of 6g/kg/h, followed by an infusion
at0.4g/kg/h.HRandMAPafterextubationwere
signifi-cantlylowerintheDexgroupthaninthesalinegroup,butno
seriouscirculatorydepressionwasobservedafterthe
admin-istrationof Dex. Arecent meta-analysis revealed alower
riskforEAfollowingDexincomparisonwithplacebo.34
How-ever,therewerelargedifferencesinDexregimen(lowdose:
0.15g/kg, high dose: 4g/kg) between studies. Shurky
etal.35 also reportedthatDex wasusedsuccessfully asa
continuousinfusion(0.2g/kg/h)for15mininthe
postop-erativeperiodtopreventorreduceEAinchildren.Onthe
other hand, Guler et al.10 and Ibacache et al.36 reported
thatasingledoseofDex(0.5g/kg)5minbeforetheendof
surgeryand0.3g/kgafterinductionofanesthesiareduced
EA without significant hemodynamic effects, respectively.
Thus, the administration of Dex at a slow rate may
con-tributetohemodynamicstability.
Inourstudy,twopatientsineachgrouprequired
supple-mentaloxygenbecauseofreduced SpO2afterextubation;
however,none ofthese patientsexhibitedsigns ofairway
obstructionandprolongedoxygenrequirement.
Therearesome limitationsinourstudy.First,although
pain is definitely a major reason for EA, screaming as a
resultof pain should be distinguished fromEA. However,
itisimpossibletodistinguishbetweenthem inchildrenin
thepreverbalstageofdevelopment.Furthermore,thereare
some difficultiesininterpreting behavior withother
influ-encingfactorssuchashungerorfearofstrangers.Although
itisuncertainwhetherpostoperativerectalacetaminophen
providedtheexpectedlevelofanalgesia,theanalgesicand
sedative effects of Dex would tobe advantageous tothis
situationininfants.
Second, we used the scoring system for EA and PS
score.5,16 Five anesthesiologists participated to assess EA
and PS score in our study. Although the method we used
iswellacceptedandhasbeenvalidatedinotherstudies,5,30
theremaybeadifferenceinanevaluationofEAandPSscore
duetoexperimenter’sbias.Ifweuseanothercriterion,
dif-ferentresultsmaybeobtained.
Third,itisimportanttonotethatwestudiedrelatively
healthyinfants andexcluded infantswithahistoryof
air-wayproblems becauseDex required inthe studyprotocol
maysubjecttheseinfantstounacceptablygreaterrisksfor
postoperativeairwaycomplications.Intheabsenceofsuch
astudy,wewouldurgecautionintheuseofDexininfants
withdocumentedairwayobstruction.Furtherstudies
focus-ingonobstructiveairwaycomplicationsduetoDexininfants
withRobinsequenceand/orTreacherCollinssyndromeare
needed.
Inconclusion,althoughoursamplesizeissmall,itseems
that theuse ofDex reducedEA andPS scorewithout any
adverseeffectsandprovidedsatisfactoryrecoverywith
sta-blehemodynamicsininfantsundergoingpalatoplasty.
Funding
The pharmaconusedinthisstudywassupportedbyOsaka
UniversityGraduateSchoolofDentistry.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgments
TheauthorsthanktheDepartmentofDentalAnesthesiology
atOsakaUniversityDentalHospitalfortheiraccommodation
inhelpingrecruitpatientsinthisstudy.
References
1.LermanJ, DavisPJ, WelbornLG, et al.Induction, recovery, andsafetycharacteristicsofsevofluraneinchildrenundergoing ambulatorysurgery.Acomparisonwithhalothane. Anesthesiol-ogy.1996;84:1332---40.
2.BaumVC,YemenTA,BaumLD.Immediate8%sevoflurane induc-tioninchildren:acomparisonwithincrementalsevofluraneand incrementalhalothane.AnesthAnalg.1997;85:313---6.
3.Keaney A, Diviney D, Harte S, et al. Postoperative behav-ioralchangesfollowinganesthesia withsevoflurane.Paediatr Anaesth.2004;14:866---70.
4.CohenIT,FinkelJC,HannallahRS,etal.Rapidemergencedoes notexplainagitationfollowingsevofluraneanesthesiaininfants and children:a comparisonwithpropofol.PaediatrAnaesth. 2003;13:63---7.
6.AonoJ,UedaW,MamiyaK,etal.Greaterincidenceofdelirium duringrecoveryfromsevofluraneanesthesiainpreschoolboys. Anesthesiology.1997;87:1298---300.
7.WellsLT,RaschDK.Emergencedeliriumaftersevoflurane anes-thesia:aparanoiddelusion?AnesthAnalg.1999;88:1308---10.
8.WelbornLG,HannallahRS, Norden JM,etal. Comparison of emergenceandrecoverycharacteristicsofsevoflurane, desflu-rane,andhalothaneinpediatricambulatorypatients.Anesth Analg.1996;83:917---20.
9.VeyckemansF.Excitationanddeliriumduringsevoflurane anes-thesiainpediatricpatients.MinervaAnestesiol.2002;68:402---7.
10.GulerG,AkinA,TosunZ,etal.Single-dosedexmedetomidine reducesagitationandprovidessmoothextubationafter pedi-atricadenotonsillectomy.PaediatrAnaesth.2005;15:762---6.
11.Mili´cM,Goranovi´cT,Knezevi´cP.Complicationsof sevoflurane-fentanyl versus midazolam-fentanyl anesthesia in pediatric cleftlipand palatesurgery:arandomizedcomparisonstudy. IntJOralMaxillofacSurg.2010;39:5---9.
12.ChenJ,LiW,HuX,etal.Emergenceagitationaftercataract surgeryinchildren:acomparisonofmidazolam,propofoland ketamine.PaediatrAnaesth.2010;20:873---9.
13.HallJE,UhrichTD,BarneyJA,etal.Sedative,amnestic,and analgesicpropertiesofsmall-dosedexmedetomidineinfusions. AnesthAnalg.2000;90:699---705.
14.PatelA,DavidsonM,TranMC,etal.Dexmedetomidineinfusion foranalgesiaandpreventionofemergenceagitationinchildren withobstructive sleep apneasyndrome undergoing tonsillec-tomyandadenoidectomy.AnesthAnalg.2010;111:1004---10.
15.OlutoyeOA, Glover CD, Diefenderfer JW, et al. The effect ofintraoperativedexmedetomidineonpostoperativeanalgesia andsedationinpediatricpatientsundergoingtonsillectomyand adenoidectomy.AnesthAnalg.2010;111:490---5.
16.MerkelSI, Voepel-LewisT,ShayevitzJR,et al.TheFLACC:a behavioralscalefor scoringpostoperativepaininyoung chil-dren.PaediatrNurs.1997;23:293---7.
17.VennRM,GroundsRM.Comparisonbetweendexmedetomidine andpropofolforsedationintheintensivecareunit:patientand clinicianperceptions.BrJAnaesth.2001;87:684---90.
18.GrantSA,BreslinDS,MacLeodDB,etal.Dexmedetomidine infu-sionforsedationduringfiberopticintubation:areportofthree cases.JClinAnesth.2004;16:124---6.
19.Jalowiecki P, Runder R, Gonciarz M, et al. Sole use of dexmedetomidinehaslimitedutilityforconscioussedation dur-ingoutpatientcolonoscopy.Anesthesiology.2005;103:269---73.
20.NicholsDP,BerkenboschJW,TobiasJD. Rescuesedationwith dexmedetomidinefordiagnosticimaging:apreliminaryreport. PaediatrAnaesth.2005;15:199---203.
21.Koroglu A, Demirbilek S, Teksan H, et al. Sedative, haemodynamicandrespiratoryeffectsofdexmedetomidinein
childrenundergoingmagneticresonanceimagingexamination: preliminaryresults.BrJAnaesth.2005;94:821---4.
22.Young ET. Dexmedetomidine sedation in a pediatric cardiac patientscheduledforMRI.CanJAnaesth.2005;52:730---2.
23.Watcha MF, Ramirez-Ruiz M, White RF, et al. Perioperative effectsoforalketorolacandacetaminopheninchildren under-goingbilateralmyringotomy.CanJAnaesth.1992;39:649---54.
24.Galinkin JL, Fazi LM, Cuy RM,et al. Use of intranasal fen-tanylinchildrenundergoingmyringotomyandtubeplacement duringhalothane andsevoflurane anesthesia.Anesthesiology. 2000;93:1378---83.
25.FairbanksCA,StoneLS,WilcoxGL.Pharmacologicalprofilesof alpha 2 adrenergicreceptor agonistsidentified using geneti-callyalteredmiceandisobolographicanalysis.PharmacolTher. 2009;123:224---38.
26.Correa-Sales C, Rabin BC, Maze M. A hypnotic response to dexmedetomidine,analpha2agonist,ismediatedinthelocus coeruleusinrats.Anesthesiology.1992;76:948---52.
27.Arain SR, Ruehlow RM, Uhrich TD, et al. The efficacy of dexmedetomidineversusmorphineforpostoperativeanalgesia aftermajorinpatientsurgery.AnesthAnalg.2004;98:153---8.
28.CohenIT,FinkelJC,HannallahRS,etal.Theeffectoffentanyl ontheemergencecharacteristicsafterdesfluraneor sevoflu-raneanesthesiainchildren.AnesthAnalg.2002;94:1178---81.
29.WeldonBC,Bell M,CraddockT.Theeffectofcaudal analge-siaonemergenceagitationinchildrenaftersevofluraneversus halothaneanesthesia.AnesthAnalg.2004;98:321---6.
30.IsikB,ArslanM,TungaAD,etal.Dexmedetomidinedecreases emergence agitation in pediatric patients after sevoflurane anesthesiawithoutsurgery.PaediatrAnaesth.2006;16:748---53.
31.Tobias JD. Dexmedetomidine: Applications in pediatric criti-calcareand pediatricanesthesiology.Pediatr CritCareMed. 2007;8:115---31.
32.BejianS,ValasekC,NigroJJ,etal.Prolongeduseof dexmedeto-midine in the pediatric cardiothoracic intensive care unit. CardiolYoung.2009;19:98---104.
33.BloorBC,WardDS,BellevilleJP,etal.Effectsofintravenous dexmedetomidineinhumans.II.Hemodynamicchanges. Anes-thesiology.1992;77:1134---42.
34.SchnabelA,ReichlSU,PoeppingDM,etal.Efficacyandsafetyof intraoperativedexmedetomidineforacutepostoperativepain in children:a meta-analysis of randomizedcontrolledtrials. PaediatrAnaesth.2013;23:170---9.
35.ShurkyM,ClydeMC,KalarickalPL,etal.Doesdexmedetomidine preventemergencedeliriuminchildrenaftersevoflurane-based generalanesthesia?PaediatrAnaesth.2005;15:1098---104.