w w w . r b o . o r g . b r
Original
Article
Transtrochanteric
fractures:
evaluation
of
data
between
hospital
admission
and
discharge
夽,夽夽
Christiano
Saliba
Uliana
a,b,∗,
Marcelo
Abagge
a,b,
Osvaldo
Malafaia
c,
Faruk
Abrão
Kalil
Filho
b,
Luiz
Antonio
Munhoz
da
Cunha
b aHospitaldoTrabalhador,Curitiba,PR,BrazilbHospitaldeClínicas,UniversidadeFederaldoParaná,Curitiba,PR,Brazil
cFaculdadeEvangélicadoParaná,HospitalUniversitárioEvangélicodeCuritiba,Curitiba,PR,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received7March2013
Accepted15May2013
Availableonline18March2014
Keywords:
Hipfractures/etiology
Hipfractures/epidemiology
Datagathering
a
b
s
t
r
a
c
t
Objective:toevaluatethedataobtainedfrompatientswithtranstrochantericfractureswho
wereattendedatatertiary-leveltraumareferralhospital,betweenadmissionanddischarge,
gatheredprospectivelybymeansoftheSINPE©software.
Methods:109consecutivepatientswhowereadmittedbetweenApril2011andJanuary2012
wereevaluatedusinganelectronicstorageandanalysisdatabaseinSINPE©.Thedatawere
gatheredprospectively,includingevaluationsonpersonalinformationaboutthepatients,
history-taking,fractureclassification(Evans–Jensen,AO/OTAandTronzo),treatmentand
discharge.
Results:thesamplewascomposedof43menand66women.Theiragesrangedfrom20to105
years,withameanof69years.Fallingwasthetraumamechanismfor92patientsandtraffic
accidentsfor17.Themostprevalentchronicdiseasesweresystemicarterialhypertension
anddiabetesmellitus.AccordingtotheAO/OTAclassification,thecommonestfracturetype
was31A1.AccordingtotheTronzoclassification,typeIIIwascommonest.Thefracture
wasfixedbymeansofacephalomedullarynailin64casesandaslidingscrew–platein44
cases.Onefracturewasfixedwitha95◦screw–plate.Sevenpatientspresentedsomeform
ofclinicalcomplicationandthreediedduringthehospitalstay.Allthepatientswhowere
dischargedwereinstructedtoonlypartiallybearweightontherepair.
Conclusion: throughSINPE©,itwaspossibletoevaluatethepersonalinformation,
history-taking,classification,treatmentanddischargeofpatientswithtranstrochantericfractures,
fromhospitaladmissiontodischarge.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora
Ltda.Allrightsreserved.
夽Pleasecitethisarticleas:UlianaCS,AbaggeM,MalafaiaO,KalilFilhoFA,daCunhaLAM.Fraturastranstrocantéricas–Avaliac¸ãodos
dadosdaadmissãoàaltahospitalar.RevBrasOrtop.2014;49:121–128.
夽夽
WorkdevelopedintheTraumaGroup,HospitaldoTrabalhador,andintheOrthopedicsService,HospitaldeClínicas,Universidade
FederaldoParaná,Curitiba,PR,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](C.S.Uliana).
2255-4971/$–seefrontmatter©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditoraLtda.Allrightsreserved.
Fraturas
transtrocantéricas
–
Avaliac¸ão
dos
dados
da
admissão
à
alta
hospitalar
Palavras-chave:
Fraturasdoquadril/etiologia
Fraturasdo
quadril/epidemiologia
Coletadedados
r
e
s
u
m
o
Objetivo: avaliarosdadosobtidosdepacientescomfraturatranstrocantéricaatendidos
emumhospitaldereferênciaterciáriadetrauma,desdeaadmissãoatéaaltahospitalar,
coletadosprospectivamentepormeiodoSinpe©.
Métodos: foramavaliados109pacientesconsecutivosadmitidosdeabrilde2011atéjaneiro
de2012.Usou-seumabaseeletrônicadearmazenamentoeanálisededados,osoftware
Sinpe©.Acoletadosdadosdeu-sedemaneiraprospectivaeinformac¸õessobredados
pes-soaisdopaciente,anamnese,classificac¸ãodasfraturas(Evans-Jensen,AO/OTAeTronzo),
tratamentoealtaforamavaliadas.
Resultados: aamostrafoicompostapor43homense66mulheres.Aidadevarioude20a105
anos,commédiade69.Aquedafoiomecanismodetraumaem92pacienteseosacidentes
detrânsitoforamem17.Asdoenc¸ascrônicasmaisprevalentesforamahipertensãoarterial
sistêmicaeodiabetesmellitus.Pelaclassificac¸ãoAO/OTA,otipomaiscomumdefraturafoi
a31A1.Pelaclassificac¸ãodeTronzo,atipoIIIfoiamaiscomum.Afraturafoifixadacom
hastecefalomedularem64casosecomplaca-parafusodeslizanteem44casos.Umafratura
foifixadacomplaca-parafuso95◦.Setepacientesapresentaramalgumacomplicac¸ãoclínica
etrêsforamaóbitoduranteointernamento.Todosospacientesquereceberamaltaforam
orientadosafazerapoioparcial.
Conclusão:pormeiodoSinpe©foipossívelavaliarasinformac¸õesrelacionadasadados
pes-soais,anamnese,classificac¸ão,tratamentoealtadepacientescomfraturatranstrocantérica
desdeaadmissãoatéaaltahospitalar.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier
EditoraLtda.Todososdireitosreservados.
Introduction
Theincidenceofproximalfemoralfractureshasbeen
increas-ing significantly and, because of greater life expectancy
amongthepopulation,itisexpectedtodoubleoverthenext
25 years.1–3 The functional results after treatment remain
unsatisfactorybecauseasignificantnumberofpatientsdonot
returntotheirfunctionalstatuspriortothefracture.4These
fractureshavetheimplicationofsocialandfinancialimpacts
onthepopulationandonthecountry.5
Amongthefracturesoftheproximalfemur,
transtrochant-ericfracturesareanimportantgroup,giventhattheyare
com-monandgenerallyaffectpatientswhohavebeendebilitated
bycomorbiditiesandareofadvancedchronologicalage.6,7
Adequatedata-gatheringwithregardtotheincidenceof
transtrochantericfracturesandtheprofileofthegroupthatis
susceptibletothemmayaidindevelopingpublicpoliciesfor
preventionandtreatment.Itmayalsoaidindeveloping
sci-entificstudies,particularlyifitisdonewithoutfailingsandif
updatedelectronicfilesthatsupplystatisticallyrelevantdata
areobtained.8
Withinthe field of medicalinformation technology,the
Sinpe©software(acronymforintegratedelectronicprotocol
system)hasbeencreated.Sinpe©isatoolusedbyseveral
med-icalspecialtiesforthepurposeofdatagathering,application
andvalidationinrelationtodiseases.9–11
Objective
Thepresentstudyhadtheaimofevaluatingthedata
gath-eredprospectivelybymeans ofSinpe©,from patients with
transtrochantericfractureswhowereattendedata
tertiary-levelreferralhospitalfortrauma,fromadmissiontodischarge.
Materials
and
methods
Thisstudy wasproperly submittedtoandapprovedbythe
EthicsCommitteeofourinstitution,andwasregisteredunder
theprotocolCEP-SESA/HTno.294/2011.
ThedataweregatheredbythefirstauthorandtheSinpe©
softwarewasusedtoelectronicallystoretheinformation.The
dataanalysistovalidatetheresultswasdonebymeansof
theSinpeAnalisador©tool,whichformspartoftheSinpe©
software.12
ThedataweregatheredbetweenApril18,2011,and
Jan-uary30,2012.Allthepatientsincludedwereadmittedtoand
treatedatatertiary-level referralhospitalfortraumainthe
cityofCuritiba.Thedata-gatheringtookplaceprospectively,
and 109consecutivepatientsadmittedtothe hospitalwith
transtrochantericfracturesofthefemurwereevaluated.
Table1showsthedataevaluatedinthisstudy.
Thedataonthepatientswere gatheredbymeans ofan
interview, directly with the individual or with his parents
and/orwiththerescueteam.
Amongthehistoricalclinicaldata,thepainintensitywas
evaluated on numericaland verbal scales.On the
numeri-cal scale,the patient was encouraged toquantifyhis pain
betweenzeroand10.Absenceofpainwasscoredaszeroand
theworstpaineverexperiencedbythepatientwasscoredas
10.Ontheverbalscale,patientswereaskedtoclassifytheir
Table1–Correlationofthedataevaluatedoneachpatientwithatranstrochantericfracture:patient’sdata, history-taking,fractureclassification,treatmentconditionsandhospitaldischarge.
Patient’sdata History-taking Classification Treatment Hospitaldischarge
Sex Intensityofpain Evans–Jensen Surgicalaccess Weight-bearingpermitted
Ethnicity Traumamechanism AO/OTA Implantsused
Age Leveloffall Tronzo Complicationsduringhospitalstay
Associatedchronicdiseases Deathsduringhospitalstay
mildandabsent.13,14Themechanismthroughwhichpatients
sufferedtheirtraumawasstatedbothbythepatientandby
thepre-hospitalrescueteam.Thisitemwassubdividedinto
“trafficaccident”,“fall”,“physicalaggression”and“gunshot
wound”.Thelevelofthefallwasdividedinto“fallfromthe
samelevel”and“fallfromaheight”.Inthecaseoffallsfroma
height,theheightofthefallinmeterswasevaluated.In
tak-ingthehistory,thepatientswereaskedaboutthepresenceof
anychronicdiseasesthattheyknewabout,suchassystemic
arterialhypertension,diabetesmellitusandcerebrovascular
diseases.
The fractures were classified by the first author based
onradiographicanalysis.TheEvans–Jensen,15AO/OTA16and
Tronzo17classificationsystemswereused.
Regarding the treatment, a traction table was used to
reducethe fractureinallcases.Onlyincasesinwhichthe
reduction on the traction table was unsatisfactory was it
decidedtoperformdirectreductionofthefracture.Tostabilize
thefracture,threesurgicalaccesseswereused:alateralaccess
belowthevastuswasusedincasesoffixationwithaplate
andslidingscrew;alateralminimally invasiveaccess
prox-imaltothegreatertrochanterwasusedincasesoffixation
withacephalomedullarynail;and,incasesinwhichdirect
reductionwas necessary, the accessprevious programmed
wasextendedsoastoexposethefocusofthefracture,
inde-pendentofthetypeofimplantused.Theimplantsusedfor
fixationofthefractureswere:slidingplate–screw,shortorlong
cephalomedullarynailand95◦ plate–screw.Theclinicaland
orthopediccomplicationsandthedeathsthatoccurredduring
hospitalizationwererecorded.
Atthetimeofhospitaldischarge,datarelatingtothetype
ofweight-bearingthatthepatientwasallowed(none,partial
orfull)weregathered.
Results
The sample consisted of 43 men (39.45%) and 66 women
(60.55%).Theiragesrangedfrom20to105years,withamean
of69.Themeanamongthemenwas64.3years(20–105),which
wasyoungerthanthemeanamongthewomenof70.3years
Zero 1 Number of patients
0 0
0 1
2 5
13
25 29
33
35 30 25 20 15 10 5 0 One
Two
Three Four Five Six Seven Eight Nine
Ten
Fig.2–Representationofpainintensityreportedbythe patientsatthetimeofadmission,accordingtothe numericalpainscale.
(20–104). Amongthe109patients ofthesample, 90(82.5%)
were morethan54yearsofageatthetimeofthefracture.
Regardingethnicity,100patientswerewhite,twowereblack,
two were mixed and five were classified as indeterminate
(Fig.1).
Thenumericalscaleshowedthatthegreatestnumberof
thepatientsreportedpainatlevel10(30.28%),followedbypain
atlevel9(26.61%)andlevel8(22.94%)(Fig.2).
The verbalscale demonstrated that the majorityof the
patientsclassifiedtheirpainas“intense”(53.21%),followed
by those who considered that their pain was “intolerable”
(30.28%)(Fig.3).
Falls were the most prevalent trauma mechanism and
occurredin92patients(84.40%),followedbytrafficaccidents
in17(15.6%)(Table2).
Amongthepatientswhosufferedfalls,85(92.39%)fellfrom
thesamelevel,whileseven(7.60%)fellfromaheight(Table3).
Systemicarterialhypertensionwasthechronicdiseaseof
greatest prevalencein the sample, reportedby 55 patients
(50.45%). Diabetes mellitus was the second most
preva-lent disease in the sample, affecting 21 patients (19.26%).
Other diseases reported included cerebrovascular diseases,
cardiopathies, chronic obstructive pulmonary disease and
Female
Male
White
From 20 to 37 years
Distribution according to age group Distribution according to ethnicity
Distribution according to gender
From 37 to 54 years
From 54 to 71 years
From 71 to 88 years
From 88 to 105 years Indeterminate
Black
Mixed 61%
39%
10% 8% 10%
30% 42%
92% 2% 2% 4%
Without pain 1
0
17
58
33
70 60 50 40 30 20 10 0
Number of patients
Mild
Moderate
Intense
Intolerable
Fig.3–Representationofpainintensityreportedbythe patientsatthetimeofadmission,accordingtotheverbal painscale.
Table2–Traumamechanismthatgaverisetothe fracture,subdividedinto“fall”,“trafficaccident”, “physicalaggression”and“gunshotwound”.
Traumamechanism Numberofpatients
Fall 92(84.40%)
Trafficaccident 17(15.6%)
Physicalaggression 0(0.00%)
Gunshotwound 0(0.00%)
Table3–Sampledistributionaccordingtothelevelof thefallthatgaverisetothefracture.
Leveloffall Numberofpatients
Samelevel 85(92.39%)
1–2m 2(2.17%)
2–3m 4(4.34%)
3–4m 0(0.00%)
>4m 1(1.08%)
chronicrenal disease.Table4 showsthe prevalenceofthe
diseasesanddoesnottakeinto accountthefactthatsome
patientspresentedmorethanonecomorbidity.
InrelationtotheEvans–Jensenclassification,60patients
(55%)presentedtypeIfractures,followedbytypeIIfractures
Evans-jensen
13%
20%
26% IA
IB
IIA
IIB
III
29% 12%
Fig.4–Percentagedistributionofthefracturesaccordingto theEvans–Jensenclassification.
Table4–Distributionofthechronicdiseasespresented bythepatientsofthissample.
Associatedchronicdiseases Numberofpatients
Systemicarterialhypertension 55(50.45%)
Diabetesmellitus 21(19.26%)
Cardiopathies 12(11%)
Cerebrovasculardisease 16(14.67%) Chronicobstructivepulmonarydisease 2(1.83%)
Chronicrenaldisease 1(0.92%)
in35patients(22%)andtypeIIIfracturesin14patients(12%) (Fig.4).
According to the AO/OTA classification, the commonest
typewas31A1,whichwasfoundin45patients(41%),followed
bytype31A2,in40(36%),andtypeIII,in24(22%)(Fig.5).
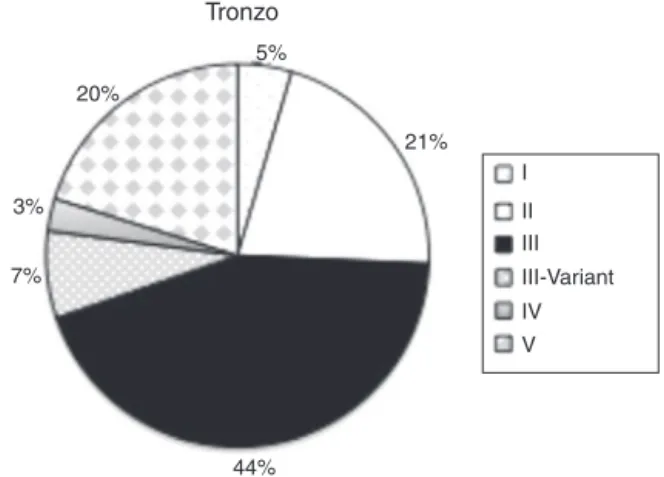
Regarding the Tronzo classification, type III was the
commonestandaffected48patients(44%).Thesecond
com-monestwastypeII,in23(21.1%)(Fig.6).
Regarding the surgical approach, a limited minimally
invasive accessproximaltothe greater trochanterwas the
approach most used (56.88%), followed bya lateral access
belowthevastus(40.36%)(Table5).
Theimplantsusedforfixationofthefracturewereasliding
plateandscrewin44cases(40%),ashortcephalomedullary
nailin43(40%),alongcephalomedullarynailin21(19%)and
a95◦plateandscrewinone(1%)(Fig.7).
AO/OTA
31.A1 31.A2 31.A3 22% 41%
37%
25%
33%
42% 25%
28% 13%
37% 50%
47%
Subdivision AO type 31 A1 Subdivision AO type 31 A2 Subdivision AO type 31 A3
A1.1 A1.2 A1.3
A2.1 A2.2 A2.3
A3.1 A3.2 A3.3
Tronzo
20%
3%
7%
44%
21% 5%
I II III III-Variant IV V
Fig.6–Percentagedistributionofthefracturesaccordingto theTronzoclassification.
40%
Short cephalomedullary nail
Implants used
Long cephalomedullary nail 95° plate-screw
Sliding plate-screw 1%
19%
40%
Fig.7–Percentagedistributionoftheimplantsusedfor fracturefixation.
Inall the109patients studied,82 (75%)didnotpresent
anytypeofcomplicationduringthehospitalstay.Amongthe
20(18%)whopresentedlocalcomplications,16(15%)evolved
withsuperficialinfection,three(3%)evolvedwithdeep
infec-tionandone(1%)presentedafractureofthelateralcortical
boneofthefemurduringtheoperation.Inthiscase,inwhich
fixationusingasliding plate andscrew hadbeen planned,
thesurgeondecidedtochangetheplanandperformthe
fix-ationusinga95◦ plateand screw.Afurthersevenpatients
(7%)presentedclinicalintercurrencesduringthehospitalstay
(Fig.8).
Duringthehospitalstay,threepatients(2.75%)evolvedto
deathand106(97.25%)weredischargedfromhospital(Fig.9).
Table5–Distributionofaccessesusedforfracture fixation.
Surgicalaccess Numberofpatients
Limitedminimallyinvasiveproximalto greatertrochanter
62(56.88%)
Lateralbelowvastus 44(40.36%)
Extendedfordirectreduction 3(2.75%)
7%
18%
75%
No complications
Complications during hospital stay
Local complications
Clinical intercurrences
Fig.8–Percentageincidenceofcomplicationspresentedby thepatientsduringhospitalstay.
3%
97%
Death
Hospital discharge
Deaths during hospital stay
Fig.9–Relationshipbetweendeathsduringhospitalstay andpatientswhoweredischarged.
Forallthe106patients(97.25%)whoweredischargedfrom hospital,itwasrecommendedthattheyshouldonlypartially bearweightonthelimb(Fig.10).
Discussion
The present study used the Sinpe© system as the storage
database,whichenabledsecuredatarecordingandprovided
statistical analysisthroughtheanalyzer moduleofSinpe©.
Otherstudiesthathavegivensupportforusingmedicalfiles
120
100
80
60
40
20
0
Full Partial None
Load-bearing
Load-bearing
Fig.10–Demonstrationthat106patientswhowere
incomputerizedmannerhavealsousedSinpe©andhave
cor-roboratedtheefficacyandgoodfunctioningofthissystem.9,10
Likeinthe present study,onthe other occasionsinwhich
Sinpe©wasused,adatabasewasfirstlydevelopedwith
biblio-graphicsupportandthenwasincorporatedelectronicallyinto
theprotocol.
Electronicdata-gatheringhasmanyadvantagesinrelation
tomanualgathering.Tociteafewofthem,datathatare
gath-eredmanuallyaregenerallynotstructuredorstandardized,
suchthat they may present flawsat the time of
interpre-tation.Theprotocol usedinthis study laidoutthe datain
astructuredandhierarchicalmanner.Theinformationwas
gatheredprospectively,withdirectinputtothesoftwareby
meansofapersonal-uselaptop.Thisdata-gatheringmethod
madeitpossibletostandardizeandvalidatetheinformation
withahighstatisticalpoweratthetimeoftheepidemiological
evaluations.8
Theprotocolthatwasdevelopedandappliedinthisstudy
madeitpossibletogathermorethan18,000datarecordson
eachpatientwithatranstrochantericfracture.Thisamount
ofinformationthatcould beextractedfromeachcasegave
the researchermanypossibilities fordatacorrelation, thus
makingitpossibletogenerateawidespectrumofstatistically
relevantanalyses.
Despitethehighqualityofthedatagathered,in
statisti-calterms,theprotocolappliedpresentedsomeflaws.Some
informationthatisconsideredrelevantwithinorthopedics,
suchas preoperative planning,date ofthe operation, date
ofhospitaldischarge,timeintervalbetweenadmissionand
theoperationandadmissiontoandreleasefromthe
inten-sivecareunit,couldnotbegatheredbecausetheprotocoldid
notallowtheirentry. However,thiswas thefirst timethat
thisprotocol was appliedtothe field oforthopedicsand it
isexpected that the protocol willundergo correctionsand
updatinginordertoprovidesupportforotherstudiesinthe
future. Another pointthat could be adisadvantage isthat
thedata-gatheringwasveryextensiveandbecametiringfor
thepatients.
Thedemographicdataregardingpredominantsexandage
demonstratedthatfemalesandthepopulationovertheageof
50yearsweremoreprevalentinthesample.Previously
pub-lishedstudiesalsoshowed thissexand agepredominance
inrelationtofracturesoftheproximalfemur.6,7However,we
foundproportionsof3:2betweenfemaleandmalepatients,
whereas theliteraturegeneralindicates proportions of2:1.
Thisfinding may beexplainedbythe fact thatmost
stud-iesrelatingtofracturesoftheproximalfemurhaveevaluated
elderlypatients,i.e.overtheageof65years.Whenyounger
patientswereincludedinthesample,thepredominanceof
female patients was inverted, given that younger patients
sufferhigh-energytraumaandthemalepopulationismore
susceptibletotrafficaccidentsorfallsfromaheight.Among
the 24 victims ofhigh-energy trauma, there were 16 male
patients(66.66%).
Regardingtheintensityofthepainthatpatientspresent
aftertranstrochantericfractures,thereislittleinformationin
theliterature.Moststudieshavedealtwithpostoperativepain
and statethat thepain isgenerally intense,but it may be
mildifthefracturedoesnotpresentanydisplacement.18The
dataanalyzedconfirmthatmostofthepatientsexperience
episodes ofintense pain. Curiously, the two patients who
reported lower intensity of pain (0 and 4 on the
numeri-calscale)presenteddisplacedandcomminutedfractures.In
comparingthetwosystemsformeasuringpainintensity, it
wasperceivedthattherewasnocorrelationbetweenthem,
giventhatonthenumericalscale,themajorityofthepatients
reported having pain of level 9or 10, while on the verbal
scale,themajorityreported“intense”painandnot
“intoler-able”pain,whichwouldhavebeenthetermcorrespondingto
“9”and“10”.Thisshowsthedifficultyinobjectivelymeasuring
subjectivecomplaintssuchaspain.Anotherpointthatneeds
tobeanalyzedisthatpatientsmayfinditeasiertotranslate
into words,suchas“intense” or“mild”,thaninto numbers
from0to10.
Morrisonetal.indicatedthatlow-energycomplaintsare
responsible for 86–95%of osteoporoticbone fractures.19 In
our sample,the commonesttraumamechanismwas afall
fromthesameleveland,inagreementwiththeliterature,this
accountedfor84.4%ofthecases.Inoursetting,Pereiraetal.
conductedastudythatincluded246patientsovertheageof
65yearswhowerevictimsoffracturesoftheproximalfemur.
Inthatstudy,thefemalepopulationaccountedfor72.7%of
thesample.20Inthepresentstudy,incorrelatingthedataon
fallsfrom thesame levelwithsex, wefoundthat78.8%of
the patientswerefemale, whichrepresentsaproportionof
approximately4:1.
Amongthe24patientswhowerevictimsofhigh-energy
trauma,themeanagewas50years,14(58.33%)wereunder
the ageof65years and16 weremale (66.66%),which
con-firms the bimodal epidemiological profile of patients with
transtrochantericfractures.
Inastudythatincluded1904patientswhosuffered
frac-tures,Gerberetal.21gathereddatarelatingtotheassociation
betweenfracturesoftheproximalfemurinelderly
individ-ualsandthepresenceofcomorbidities.Theyfoundthatthe
most prevalent disease was systemic arterialhypertension
(SAH)(66%),followedbycerebrovasculardiseases(33%)and
diabetesmellitus(16%).Inoursample,theprevalentdisease
wasalsoSAH(50.45%),butthesecondmostprevalentwas
dia-betesmellitus(19.26%),followedbycerebrovasculardiseases
(14.64%).
Thefractureswereclassifiedbythefirstauthorusingthree
systemsthathavebecomeestablishedintheliterature.15–17
Since the protocol can be used in a multicenter manner,
thesoftwareallowsresearcherstoclassifythefracturesinto
seven different systems. In comparing the incidences of
the fracture typesAO31 A3,Tronzo Vand Evan–Jensen III
of the present study with the articles that describe these
classification systems, it could be seen that the
preva-lenceofthesefracturetypesofgreaterseveritywerehigher.
This demonstrates the current trend toward trauma
pro-duced by mechanisms of higher energy, such as traffic
accidents.
Regarding the implants used for fixation, the literature
suggests thatforstabletranstrochantericfractures,surgical
fixationwithaslidingplateandscrewprovidesresultsthat
aresimilartothoseusingcephalomedullarynails.22–24
How-ever,forunstablefractures,fixationusingnailsora95◦plate
andscrewisrecommended.25Inthepresentstudy,therewas
that59%ofthefractureswerefixedinthismanner.Itislikely
thattheavailabilityandeasyaccesstonailsthatexistsinour
institutionisthereasonwhysomestablefractureswerealso
fixedusingnails.Alltheunstablefracturesandthose
extend-ingtothediaphysiswerefixedusingcephalomedullarynails
ora95◦plateandscrew.
The deep infection rate was found to be 3%, which is
within the parameters expected in trauma referral
hospi-tals.Harrisonet al.studied6905casesofhip fracturesand
foundadeepinfectionrateof0.7%.26Thereportsinthe
lit-eraturedemonstratethatthedeepinfectionratefollowinga
transtrochantericfracture ranges from0.15% to15%.27 The
mortalityrateintheliteratureishigh,witharangefrom12%
to41%overthe firstsixmonthsaftertheoperation.28,29 In
oursample,threedeathsoccurredduringthehospitalstay,
allresultingfromclinicalcomplications.Thesethreepatients
weresmokersandalcoholabusers,andtheypresented
comor-bidities.
Whileinthehospital,thepatientshad daily
physiother-apysessions,duringwhichtheywereencouragedtogetout
ofbedearlyonandtakesomestepswiththeaidofawalking
frame.Sinceoneoftheobjectivesofthesurgerywastoreturn
tothepreviouslevelofphysicalactivity,allthepatientswere
instructedatthetimeofhospitaldischargetopartiallyplace
weightontheoperatedlimb.
Conclusion
Through Sinpe©, it was possible to evaluate the
infor-mation relating to personal data, history-taking,
classifi-cation, treatment and hospital discharge of patients with
transtrochantericfractures,fromadmissiontodischarge.
Conflicts
of
interest
Theauthorsdeclarethattherewerenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. GulbergB,DuppeH,NilssonB.Incidenceofhipfracturesin Malmo.Sweden(1950–1991).Bone.1993;14Suppl.1: 23–9.
2. KannusP,ParkkariJ,SievänenH,HeinonenA,VuoriI, JärvinenM.Epidemiologyofhipfractures.Bone.1996;18 Suppl.1:57–63.
3. ZuckermanJD,KovalKJ,AharonoffGB,HiebertR,SkovronML. Afunctionalrecoveryscoreforelderlyhipfracturepatients:I. Development.JOrthopTrauma.2000;14(1):20–5.
4. KuzykPR,LoboJ,WhelanD,ZderoR,McKeeMD,Schemitsch EH.Biomechanicalevaluationofextramedullaryversus intramedullaryfixationforreverseobliquityintertrochanteric fractures.JOrthopTrauma.2009;23(1):31–8.
5. HaidukewychGJ.Intertrochantericfractures:tentipsto improveresults.JBoneJointSurgAm.2009;91(3): 712–9.
6. HungriaNetoJS,DiasCR,AlmeidaJDB.Características epidemiológicasecausasdafraturadoterc¸oproximaldo fêmuremidosos.RevBrasOrtop.2011;46(6):660–7.
7. RochaMA,CarvalhoWS,ZanquetaC,LemosSC.Estudo epidemiolo′gicoretrospectivodasfraturasdofêmurproximal
tratadosnoHospitalEscoladaFaculdadedeMedicinado TriânguloMineiro.RevBrasOrtop.2001;36(8):311–6.
8.ShahJ,RajgorD,PradhamS,McCreadyM,ZaveriA,Pietrobon R.Electronicdatacaptureforregistriesandclinicaltrialsin orthopaedicsurgery.ClinOrthopRelatRes.
2010;(468):2664–71.
9.YabumotoS.Baseeletrônicadedadosclínicosecirúrgicos semtromboembolismovenoso[tese].Paraná:Universidade FederaldoParaná;2011.
10.MottinCC.Protocoloeletrônicomultiprofissionaldecoletade dadosclínicosecirúrgicoseminsuficiênciavenosacrônica [tese].Paraná:UniversidadeFederaldoParaná;
2011.
11.BergerCAS.Coletadedadoseletrônicosparaanálisede manobrascirúrgicasempacientessubmetidosarinoplastia [tese].Paraná:UniversidadeFederaldoParaná;
2011.
12.PintoJSP.Interfacedeviabilizac¸ãodeinformac¸õ˜esparao SistemaIntegradodeProtocolosEletrônicos.[tese].Paraná: UniversidadeFederaldoParaná;2005.
13.EppsCD.Recognizingpainintheinstitutionalizedelderwith dementia.GeriatrNurs.2001;22(2):71–9.
14.CaumoW,SchmidtAP,SchneiderCN,BergmannJ,Iwamoto CW,AdamattiLC,etal.Preoperativepredictorsofmoderateto intenseacutepostoperativepaininpatientsundergoing abdominalsurgery.ActaAnaesthesiolScand.
2002;46(10):1265–71.
15.EvansEM.Thetreatmentoftrochantericfracturesofthe femur.JBoneJointSurgBr.1949;31(2):190–203.
16.MullerME,AllgowerM,ShneiderR.Thecomprehensive classificationoffracturesoflongbones.In:MullerME, AllgowerM,editors.Manualofinternalfixation:techniques recommendedbytheAO-ASIFgroup.3rded.Berlin: Springer-Verlag;1991.p.118.
17.TronzoRG,editor.Surgeryofthehipjoint.Philadelphia:Lea& Febiger;1973.
18.KovalK.Intertrochantericfractures.In:Rockwoodand Green’sfractureinadults.Philadelphia:LippincottWilliams& Wilkins;2006.p.1794–825.
19.MorrisonA,FanT,SenSS,WeisenfluhL.Epidemiologyoffalls andosteoporoticfractures:asystematicreview.Clinicoecon OutcomesRes.2013;5:9–18.
20.PereiraSR,PutsMT,PortelaMC,SayegMA.Theimpactof prefractureandhipfracturecharacteristicsonmortalityin olderpersonsinBrazil.ClinOrthopRelatRes.
2010;468(7):1869–83.
21.GerberY,Melton3rdLJ,McNallanSM,JiangR,WestonSA, RogerVL.Cardiovascularandnoncardiovasculardisease associationswithhipfractures.AmJMed.
2013;126(2):169.e19–26.
22.LittleNJ,VermaV,FernandoC,ElliottDS,KhaleelA.A prospectivetrialcomparingtheHollandnailwiththe dynamichipscrewinthetreatmentofintertrochanteric fracturesofthehip.JBoneJointSurgBr.2008;90(8):1073–8.
23.LiuM,YangZ,PeiF,HuangF,ChenS,XiangZ.A
meta-analysisoftheGammanailanddynamichipscrewin treatingperitrochantericfractures.IntOrthop.2010;34(3): 323–8.
24.BhandariM,SchemitschE,JönssonA,ZlowodzkiM,
HaidukewychGJ.Gammanailsrevisited:gammanailsversus compressionhipscrewsinthemanagementof
intertrochantericfracturesofthehip:ameta-analysis.J OrthopTrauma.2009;23(6):460–4.
26.HarrisonT,RobinsonP,CookA,ParkerMJ.Factorsaffecting theincidenceofdeepwoundinfectionafterhipfracture surgery.JBoneJointSurgBr.2012;94(2):237–40.
27.Intertrochanterichipfractures.BaumgaertnerMR,Browner BD,JupiterJB,LevineAM,TraftonPG,editors.Skeletaltrauma. Philadelphia:Elsevier;2007.p.1776–816.
28.DahlE,Mortality.lifeexpectancyafterhipfractures.Acta OrthopScand.1980;51(1):163–70.