w w w . r b o . o r g . b r
Original
Article
Intra-focal
reduction
and
percutaneous
fixation
of
neck
fractures
of
the
fifth
metacarpal:
description
of
surgical
technique
夽
,
夽夽
Gustavo
Pacheco
Martins
Ferreira
a,∗,
Paulo
Randal
Pires
a,
André
Lopes
Portugal
b,
Henrique
de
Gouvêa
Schneiter
c aHospitalMariaAméliaLins,BeloHorizonte,MG,BrazilbHospitalRisoletaTolentinoNeves,BeloHorizonte,MG,Brazil
cHospitalEládioLasserre,Cajazeiras,Salvador,BA,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received11December2012 Accepted7May2013
Availableonline27March2014
Keywords:
Metacarpal Bonefractures Upperlimb BoneWires
a
b
s
t
r
a
c
t
Objective:to demonstrate a surgical technique for treating neck fractures of the fifth metacarpal,bymeansofreductionthroughintra-focalmanipulationandpercutaneous fix-ationusingKirschnerwires,withtheaimsofmakingiteasiertoachieveandmaintainthe reductionduringtheoperationandenablingreductionofthesefracturesevenifafibrous callushasformed.
Methods:aseriesoftenpatientswithneckfracturesofthefifthmetacarpalpresenting pal-maranglesgreaterthan30◦underwentthesurgicaltechniquedescribed,asexamples,and
theirresultswereevaluatedthroughpostoperativeradiographsandclinicalexaminations.
Results:allthepatientsachievedreductionsthatwereclosetoanatomicalandevolvedto consolidationofthefractureinthepositionobtained.
Conclusion:thesurgicaltechniquedescribediseffective,easytocarryout,minimally inva-siveandlow-cost,therebyenablingadequateclinicalandradiographicreduction,evenin subacutefracturesalreadypresentingafibrouscallus.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Reduc¸ão
intrafocal
e
fixac¸ão
percutânea
das
fraturas
do
colo
do
quinto
metacarpo
–
descric¸ão
de
técnica
cirúrgica
Palavras-chave:
Metacarpo Fraturasósseas Membrosuperior Fiosortopédicos
r
e
s
u
m
o
Objetivo:demonstrarumatécnicacirúrgicaparaotratamentodasfraturasdocolodoquinto metacarpopormeiodereduc¸ãopormanipulac¸ãointrafocalefixac¸ãopercutâneacomfios deKirschner,visandoafacilitaraobtenc¸ãoemanutenc¸ãodareduc¸ãonointraoperatórioe possibilitarareduc¸ãodessasfraturas,aindaquecomcalofibrosoformado.
夽
Pleasecitethisarticleas:FerreiraGPM,PiresPR,PortugalAL,Schneiter,HG.Reduc¸ãointrafocalefixac¸ãopercutâneadasfraturasdo colodoquintometacarpo–descric¸ãodetécnicacirúrgica.RevBrasOrtop.2014;49:116–120.
夽夽
WorkperformedatHospitalMariaAméliaLins,BeloHorizonte,MG,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](G.P.M.Ferreira).
2255-4971/$–seefrontmatter©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditoraLtda.Allrightsreserved.
Métodos: dezpacientesportadoresdefraturadocolodoquintometacarpocomangulac¸ão palmarsuperiora30◦foramsubmetidos,comoexemplos,àtécnicacirúrgicadescrita.Os
resultadosforamavaliadospormeioderadiografiaseexameclínicopós-operatório.
Resultados: todosospacientesobtiveramreduc¸ãopróximadaanatômicaeevoluírampara consolidac¸ãodafraturanaposic¸ãoobtida.
Conclusão:atécnicacirúrgicadescritaéeficaz,desimplesexecuc¸ão,minimamenteinvasiva, debaixocustoepermitereduc¸ãoclínicaeradiográficaadequadas,mesmoem fraturas subagudascomcalofibrosoformado.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Fractures of the neck of the fifth metacarpal generally result from an axial impact mechanism on the head of the metacarpal with the fist closed. For this reason, they are known as boxer’s fractures, even though they only rarelyoccuramongprofessionalpugilists.1–4Thesefractures
generallypresentpalmarangulationbecauseofthe deform-ing force of the interosseous muscles and comminution ofthe volarcortex,withconsequent instability.4 Asagittal
angle greater than 30◦ or shortening of more than 5mm
is associated with alteration of the biomechanics of the flexor system and may lead to dysfunction. Presence of rotationaldeviationgreaterthan5◦ mayleadto
superimpo-sition ofthe affected ray, with obstruction ofthe adjacent fingers.1,2,4,5
In1938,Jahss6describedamaneuverforreducingfractures
ofthemetacarpals withpalmar displacementthat became establishedboth forconservative treatment and for main-tainingthereductionduringsurgicalfixation.However,this maneuverrequiresanassistanttomaintainthereduction dur-ingtheoperation,whichalsoaddsdifficultytopercutaneous insertionoftheKirschnerwiresunderradioscopybecausethe assistant’sandthepatient’shandsoverlapandalsobecause thereductionoftenbecomeslostifthereisanymovementof thehand.Furthermore,themaneuverisincapableofreducing subacutefractureswithafibrouscallusalreadyformed,which typicallyoccursafter7–10days.
In1987,Kapandji7describedanewtechniqueforreduction
andintrafocalfixationoffracturesofthedistalradius.Because ofthesuccessofthistechnique,itbecameestablishedandwas extrapolatedfortreatingseveraltypesoffracture.Thisserved asmotivationforapplicationtofracturesoftheneckofthe fifthmetacarpal.
Inthepresentstudy,atechniqueforintrafocalreduction andpercutaneousfixationwithKirschnerwiresfortreating fracturesoftheneckofthefifthmetacarpalisdescribed,the radiographicresultsobtainedarepresentedand the advan-tagesofthistechniquearediscussed.
Materials
and
methods
BetweenSeptemberandOctober2012,tenpatientswithneck fracturesofthefifthmetacarpalweretreatedsurgicallyusing thetechniquedescribed, andthe radiographicresultswere
Fig.1–Measurementoffracturedisplacementangle.
recorded todemonstratetheefficacy ofthetechnique.The othercharacteristicsofthepatientsaredescribedinTable1.
All the patients were operated by a single professional hand surgeon. Theinclusion criteria were as follows: frac-turewithvolardisplacementinthesagittalplanegreaterthan 30◦ and/orrotationaldisplacement greaterthan 5◦ on
clin-icalexamination; andlength ofevolutionafterthe trauma ofbetween1and21days.Theexclusioncriteriawere skele-tal immaturity,exposedfracture, previousfracturing ofthe fifthmetacarpal and fracturing extendingtothe joint.The preoperativeandpostoperativedisplacementsofthefracture weremeasuredonradiographsinposteroanteriorandoblique (semipronatedat30◦)viewsoftheaffectedhand,bymeansof
astandardmethodfordeterminationoftheanatomicalaxis. Theangleswere measuredusingtheAdobePhotoshopCS3 Extended10.0software(Fig.1).
Descriptionofthetechnique
Table1–Patients’characteristics.
Patient Sex Age Palmarangulation Rotation Lengthofevolution(days)
1 M 27 56.9 No 15
2 M 36 32.8 No 20
3 M 18 42.1 No 10
4 M 19 55.9 No 15
5 M 19 42.8 No 17
6 M 18 64.1 No 5
7 M 30 59.6 No 21
8 M 19 49.4 No 19
9 M 19 50.2 No 14
10 M 22 49.2 No 9
Mean=22.7 Mean=50.3◦ Mean=14.5
Fig.2–Introductionoftheintrafocalwire.Positionconfirmedbymeansofradioscopy.
Fig.3–Reductionofthefracture.
Fig.4–Mobilityofthemetacarpophalangealjointwithoutlossofreduction.
metacarpalspresentsubcutaneouslocationsonthedorsumof thehand(Fig.3).Maintainingthewireinthispositionenabled metacarpophalangealjointmobilitywithoutlossofthe reduc-tion,which facilitatedevaluation ofthe possiblerotational
Fig.5–Fixationofthefracture.
anchoredatthebaseofthemetacarpalforbetterstabilization ofthefixation(Fig.5)and wereleftprotrudingthroughthe skinwiththepointsfoldedover.
Afterfixation,radiographswereproducedin posteroante-rior,lateralandoblique(semipronatedat30◦)viewsinorderto
measuretheanglesobtained.Thepatientswerethen immobi-lizedbymeansofashortulnarplastercastsplintthatcovered the fourthand fifthfingers inintrinsic-plus position.They weredischargedfrom hospitalafterrecoveryfrom anesthe-sia,withaprescription foranalgesicstouse athome.The Kirschnerwireswereremovedasanoutpatientprocedurein thefourthweekandthepatientswerethenreferredforhand therapy. In the sixth postoperative week, newradiographs wereproducedinordertomeasuretheanglesandassessthe radiographicconsolidation.
Results
Allthepatientsachievedangulationoflessthan30◦onthe
oblique radiograph semipronated at 30◦ in the immediate
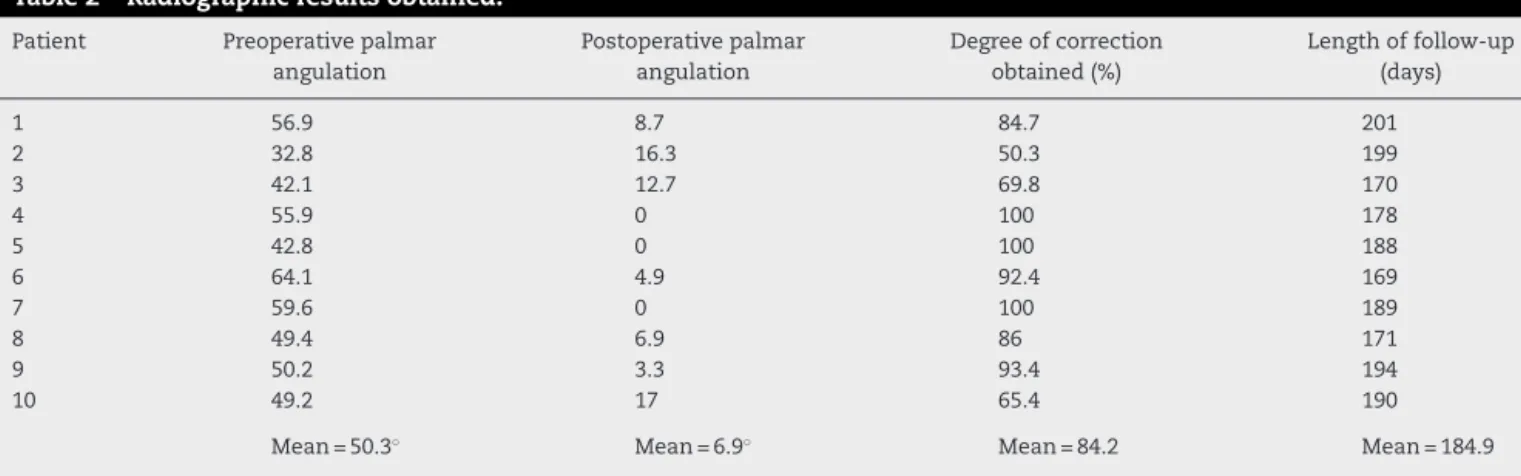
postoperativeperiod. Noneofthe casespresentedresidual angulationinthecoronalplane,malrotationorshorteningin theclinicalorradiographicexamination.Themeanlengthof follow-upwas184.9days(minimumof169)(Table2).Innone ofthecaseswasconversiontoopensurgerynecessary.
Inallcases,theradiographobtainedinthesixth postopera-tiveweekshowedradiographicconsolidationwithouttheloss ofthereductionthatwasinitiallyobtained.Nocomplications suchashyper-reduction,translationaldisplacement,increase
inthefractureline,extensorinjuryorinfectiononthepaths oftheKirschnerwireswereobserved.
Discussion
Fracturesoftheneckofthefifthmetacarpalareamongthe onesmostcommonly treatedbytraumatologistsand hand surgeons.Althoughthereisnoconsensusregardingwhatthe acceptable volarangulation ofthese fractures is,and even thoughsomeauthorshaveacceptedangulationofupto70◦
inthesagittalplaneinsedentarypatients,thereisevidence ofvariabledegreesofdysfunctionatangulationsgreaterthan 30◦,albeit thatinsomecasesthe functional deficitis
sub-jectiveandpoorlyassessedbythefunctionalquestionnaires currentlyinuse.1,2,4,5 Thereisnodoubtthatmanyofthese
fractures canbe treatedconservatively.However,reduction as close as possible to the anatomical position should be sought,especiallyduringsurgicaltreatment,butminimizing theadditionaltraumatotheadjacentsofttissuesandtheir complications.
Thereisnoconsensusregardingthebestwaytomeasure theanglesonradiographs.Somestudieshaveshownlowto moderate degrees ofintra-and inter-observerconcordance formethodsofdeterminingtheanatomicalaxis(medullary canal)andthelinestangentialtothedorsalcorticalbone.1,3,8
Anatomicalobservationshaveshownthatthemetacarpalsare notrectilinear,butpresentwide-radiuscurvaturealongtheir axisinthesagittalplane,withvolarconcavity,andanormal angleofaround15◦betweentheneckandthediaphysis.Thus,
Table2–Radiographicresultsobtained.
Patient Preoperativepalmar
angulation
Postoperativepalmar angulation
Degreeofcorrection obtained(%)
Lengthoffollow-up (days)
1 56.9 8.7 84.7 201
2 32.8 16.3 50.3 199
3 42.1 12.7 69.8 170
4 55.9 0 100 178
5 42.8 0 100 188
6 64.1 4.9 92.4 169
7 59.6 0 100 189
8 49.4 6.9 86 171
9 50.2 3.3 93.4 194
10 49.2 17 65.4 190
measurementbymeansoflinestangentialtothedorsal cor-ticalbonetendstooverestimatethedisplacementangleand becomesparticularlydifficultinfracturesthataremoredistal, becauseoftheellipticalshapeofthemetacarpalhead,andin lateralprojection,becauseoftheoverlappingofimagesfrom theothermetacarpals.8
Measurement ofthe anglefrom the anatomical axis in obliqueprojection,semipronatedat30◦,waschosenbecause
oftheease ofidentifyingthemedullarycanalofthe proxi-malfragmentofthemetacarpalandbetterevaluationofthe fractureline,withoutoverlappingofimagesfromtheother metacarpals, which enables measurements that are more reproducible. Oblique view tend to underestimate the real angleofthefracture,butitisknownthatthemaximum dif-ferenceis4◦intheobliqueprojectionat30◦inrelationtothe
absoluteprofile.9
ThemaneuverdescribedbyJahssin1938wasdestinedfor conservative treatmentof thesefractures but, despite pro-motingsatisfactoryreductioninacutecases,theseunstable fracturesalmostinvariablyconsolidatewithsomedegreeof lossofthereductionthatwasinitiallyobtained.1,4,6,8During
thesurgicalprocedure, wealsoobservedthatthereduction obtained through the maneuver was difficult to maintain becauseittendedtobecomelostthroughmovementofthe patient’shandintheoperatingfield.Anassistantwasneeded inordertoperformthemaneuverandmaintaintheposition throughoutthefixation,withtheinconvenienceof overlap-pingoftheimagesofthepatient’shandandtheassistant’s handintheradioscopy,aswellastheexposureofthe assis-tant’shandstoradiation.Lastly,incasesthathaveevolvedfor morethan7–10days,eitherinpatientswhohaveundergone anattempttoprovideconservativetreatmentandmayhave evolvedtolossofthereduction,orincasesofdelayed sur-gicaltreatment,themaneuverisnotcapableofreducingthe fracture.Insuchcases,openreductionandfixationwith mini-platesandscrewsorwithKirschnerwireswillbenecessary, i.e.surgeryoflargerscale,highercostandgreater potential forcomplications,particularlyadherencesoftheextensor ten-donsandjointcontracturesthatleadtolossofmovement.
Thetechniquedescribedinthe presentstudy iseasy to performandcanevenbedonewithoutanassistant.Itenables adequatefracturereduction,independentofthedegreeof dis-placementinthesagittal andcoronalplanes.In casesthat haveevolvedfor7–21days,reductionisstillpossiblebecause oftheleverageforcethatisapplieddirectlytothedistal frag-ment, and the principles and advantages ofpercutaneous surgeryaremaintained.Thesurgeon’shandscanbekeptout oftheirradiationbandwhileobtainingintraoperative radio-scopicimages,withoutlossofreduction,therebyminimizing theexposuretoradiation.
WeonlyusedKirschnerwiresasthe implant:theseare widelyavailableand havealowcost.Wechosetoperform fixationusingcrossedwiresinaretrogrademanner,withan entrypointintheextra-articularpartofthemetacarpalhead, soasnottoblockmovement.However,thesamereduction techniquecan beused forfixation withlongitudinal wires (intramedullary)ortransversewires(anchoredinthefourth metacarpal),asdescribedbyGallanakisetal.10Sofar,thereis
nodefinitiveevidencetoshowthatonemethodisbetterthan theothers.1–4
Theaimofthisstudywastogiveexamplesand demon-stratethesurgicaltechnique,andforthisreason,thesample was limited toten patients.We believethat thelong-term results would be equivalent to those from traditional sur-gical treatmentinacutecases,sincetheadditionaltrauma is negligible and the postoperative approach is the same. Subacutecaseswithoutthepossibilityofreductionthrough a closed maneuver may benefit from intrafocal reduction because of the lower aggressiveness and morbidity of the procedure, inrelation to open reduction. New studies will be necessary to verify possible changes in the functional results.
Conclusion
Thesurgicaltechniqueofintrafocalmanipulationand percu-taneousfixationdescribedherefortreatingneckfracturesof thefifthmetacarpaliseasytoperformandenablesclinical sat-isfactoryclinicalandradiographicreductionevenforsubacute fractureswithafibrouscallusalreadyformed.Itisminimally invasive,hasalowcostandbecomesanoptionfortreating thesefractures.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.BeredjiklianPK.Smallfingermetacarpalneckfractures.J HandSurgAm.2009;34(8):1524–6.
2.HofmeisterEP,KimJ,ShinAY.Comparisonof2methodsof immobilizationoffifthmetacarpalneckfractures:a prospectiverandomizedstudy.JHandSurgAm. 2008;33(8):1362–8.
3.SoongM,GotC,KatarincicJ.Ringandlittlefingermetacarpal fractures:mechanisms,locations,andradiographic
parameters.JHandSurgAm.2010;35(8):1256–9.
4.FreelandAE,GeisslerWB,WeissAP.Surgicaltreatmentof commondisplacedandunstablefracturesofthehand.Instr CourseLect.2002;51:185–201.
5.MeunierMJ,HentzenE,RyanM,ShinAY,LieberRL.Predicted effectsofmetacarpalshorteningoninterosseousmuscle function.JHandSurgAm.2004;29(4):689–93.
6.JahssSA.Fracturesofthemetacarpals–anewmethodof reductionandimmobilization.JBoneJointSurgAm. 1938;20:178–86.
7.KapandjiA.Focalpinningofradialdistalfractures.Cahier Cirurg.1987;63:258.
8.LeungYL,BeredjiklianPK,MonaghanBA,BozentkaDJ. Radiographicassessmentofsmallfingermetacarpalneck fractures.JHandSurgAm.2002;27(3):443–8.
9.CostaAC,FonsecaGM,RibeiroAG,GonzalesDH,Fonseca FilhoJM,ChakkourI.Qualoângulorealdodesviodafratura docolodometacarpianonasincidênciasoblíquas?Estudo radiográfico.[TemaLivreapresentadono31◦Congresso
BrasileirodeCirurgiadaMão,2011].SantaCasadeSãoPaulo; 2011.