w w w . r b o . o r g . b r
Technical
Note
Reconstruction
of
chronic
tearing
of
the
distal
triceps
using
the
double-row
configuration:
technical
note
夽
Alexandre
Firmino
Paniago
a,
Thiago
Medeiros
Storti
a,∗,
Rafael
Salomon
Silva
Faria
a,
Dennys
Carlos
Aragão
de
Morais
a,
Murillo
Pablo
de
Souza
baInstitutodoOmbrodeBrasília,Brasília,DF,Brazil
bClínicaVidere,Brasília,DF,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received25August2014 Accepted6October2014 Availableonline29August2015
Keywords:
Tendoninjury Tendonsurgery Elbow
a
b
s
t
r
a
c
t
Tearingofthedistaltricepsisuncommonandmaybedifficulttodiagnose,especiallyin situationsofpartialtearing.Imagingmethodssuchasultrasonographyandmagnetic reso-nanceimagingshouldbeusedtoconfirmthediagnosisanddefinetheextentoftheinjury. Thepreferredtreatmentforcompletetearingofthetricepsissurgical,unlikeincasesof partialtearing,inwhichthetreatmentdependsonfactorssuchaspain,functionaldeficit andthepatient’sexpectations.Here,wedescribethecaseofapatientwithpartial tear-ingofthedistaltricepsafterfallingtotheground,whichwasnotdiagnosedatthetimeof firstattendanceandevolvedwithpainandgreatfunctionalloss.Thesurgicalprocedurewas performedninemonthsaftertheinjury,withreconstructionofthetricepsbymeansof rein-forcementusingthetendonoftheipsilateralsemitendinosusandfixationintheolecranon usingthedouble-rowconfiguration.Thepatientremainedimmobilizedusingaslingforone weekandthengainsinpassiverangeofmotion(ROM)wereintroduced.Threeweekslater, thepatientwasreleasedforgainsinactiveROM.Musclestrengtheningwasstartedafter12 weeks.Sixweeksafterthesurgicalprocedure,thepatientwasfreefrompainandpresented completeROM,gradeVelbowextensionforceandhypertrophyofthetriceps.Thetechnique
describedherewasshowntobeusefulfortreatingtearsofthetendonofthedistaltriceps. ©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Reconstruc¸ão
de
ruptura
crônica
do
tríceps
distal
sob
a
configurac¸ão
de
dupla
fileira:
nota
técnica
Palavras-chave:
Traumatismosdostendões
r
e
s
u
m
o
Rupturasdotrícepsdistalsãoincomunsepodemserdedifícildiagnóstico,especialmente asparciais.Métodosdeimagem,comoUSGeRNM,devemserusadosparaaconfirmac¸ão
夽
WorkperformedintheServic¸odeCirurgiadeOmbroeCotovelo,HospitalOrtopédicoeMedicinaEspecializada(HOME),Brasília,DF, Brazil.
∗ Correspondingauthor.
E-mail:[email protected](T.M.Storti).
http://dx.doi.org/10.1016/j.rboe.2015.08.010
Tendões/cirurgia Cotovelo
diagnósticaeparadefinic¸ãodaextensãodalesão.Otratamentodeescolhaparaasrupturas completasdotrícepséocirúrgico,diferentementedasparciais,quedependemdefatores comodor,déficitfuncionaleexpectativasdopaciente.Descrevemosocasodeumpaciente comrupturaparcialdotrícepsdistalapósquedaaosolo.Nãofoidiagnosticadonomomento doprimeiroatendimentoeevoluiucomdoregrandeperdafuncional.Oprocedimento cirúr-gicofoifeitoapósnovemesesdotrauma,comareconstruc¸ãodotrícepspormeiodereforc¸o comotendãodosemitendíneoipsilateralefixac¸ãonoolécranosobaconfigurac¸ãodedupla fileira.Opacientepermaneceuimobilizadocomtipoiaporumasemanaeiniciou-se,apartir daí,oganhodeamplitudedemovimento(ADM)passiva.Apóstrêssemanasfoiliberadopara oganhodeADMativa.Ofortalecimentomusculariniciou-seapós12semanas.Apósseis mesesdoprocedimentocirúrgicoopacienteapresenta-sesemdor,ADMcompleta,forc¸ade extensãodocotovelograuVehipertrofiadotríceps.Atécnicadescritasemostrouútilpara
otratamentoderupturasdotendãodotrícepsdistal.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Tearing ofthe tendon ofthe distaltriceps is arare injury thataccountsforlessthan1%ofthetendoninjuriesofthe upperlimbs.1Forthisreason,fewstudiesintheliteraturehave defined any treatment patterns or made any comparisons betweenthetypesoftreatment.Thisinjurygenerallyoccurs asanavulsionattheboneinsertionofthetendon,inthe ole-cranon.Morerarely,itoccursasalesionwithinthemuscle2or atthemuscle-tendonjunction.3Theinjurymechanism con-sistsoffallingwiththehandextended,butdirecttraumato theposteriorfaceoftheelbow4hasalsobeendescribed.
Casesofcompletetearingrequiresurgicaltreatment,with primaryrepairorreconstruction.Ontheotherhand,casesof partialtearingareoftendifficulttodiagnoseimmediatelyafter theinjury.Theseareusuallydiagnosedafterlongperiodsof painand functionallimitation ofthe limb.5 Imaging meth-odssuchasultrasonography(USG)andmagneticresonance imaging(MRI) are generallyused forthe diagnosis and for ascertainingtheextentoftheinjury.
Surgical treatment of partial tearing is generally done whenthepatientcontinuestopresentsymptomsdespitethe non-surgicaltreatment.Primaryrepairoftheinjuryisoften difficultincasesinwhichalongperiodoftimehaselapsed sincetheinjury.Inthesecases,tendonreconstruction tech-niquesneedtobeapplied.5
Thisarticlepresentsadescriptionofapatientwhosuffered chronictearingof thedistal tendonofthe brachial triceps muscleandthenunderwentreconstructionusingagraftfrom thetendonofthesemitendinosusmuscle,withfixationtothe olecranoninadouble-rowconfiguration.Thetechniquewas showntobereproducible,withgoodresults.
Case
report
Thepatientwas38yearsofageandhadsufferedafalltothe groundduringsportspracticeninemonthsearlier.Sincethen, hehad presentedpainanddifficulty intasksthat required elbowextensionforce,suchaspushingacardoortoopenit.
Hehadinitiallybeenattendedatanotherinstitution,where theinjuryhadnotbeendiagnosed.Instead,hehadbeen diag-nosedashavingbruisingonhiselbow.Hereceivedthecorrect diagnosiseightmonthsafterthetrauma.Hewasthenreferred toourserviceforthecorrecttreatment.Conservative treat-ment had already been administered over this period,but withoutanyimprovementinhiscondition.
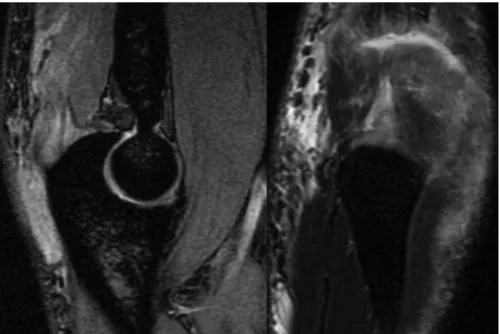
Atthephysicalexamination,hepresentedbulginginthe posteriorregionofthedistalthirdoftheupperarm,acomplete rangeofflexion–extension,gradeIVelbowextensionstrength andpainwhenperformingextensionagainstresistance.MRI showedpartialtearingoftheinsertionofthetricepstendon intheolecranon(Fig.1).
Surgical
technique
Surgicaltreatmentwasindicated.Reconstructionsurgeryon theinjuredtendonwaschosenbecauseofthelengthoftime sincetheinjuryandthedegreeofretractionofthetornfibers. The techniqueoftransferring the tendonof theipsilateral semitendinosusmusclewasusedbecauseofourfamiliarity withthistechniqueandwiththecharacteristicsofthe trans-ferredtendon.
Thepatientwaspositionedondorsaldecubitusbecauseof theneedtoremovethetendonfromtheknee,andthelimb wasfixedtothepositioningdeviceofthetable(Trimano).
Fig.1–Magneticresonanceimaging(sagittalandcoronal)showingpartialtearingofthetendonofthedistaltriceps.
Twotransosseoussuturesweremademoreposteriorly,using no.2high-resistancethread,whichwaspassedthroughthe tricepsgraftcombinationwiththesuturelocked.Theexitwas atthemostdistalextremityofthetendon(Figs.3and4).The suturesweremadewiththeelbowflexedat90◦.
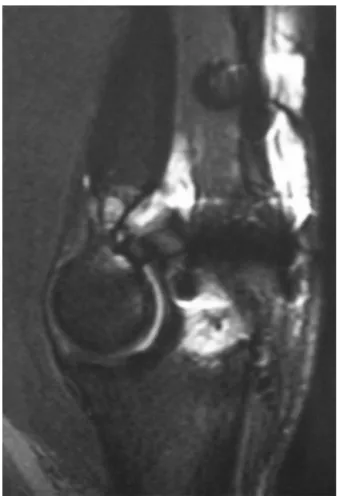
Thepatient was kept immobilized by means ofa sling foroneweek.Subsequently,self-performedpassiveexercises were started.Three weekslater,gains ofactivemovement were started. Muscle strengthening exercises were started afterthethirdpostoperativemonth.Sixmonthsafterthe oper-ation,MRIwasproducedagain,andthisshowedthatcomplete tendonhealinghadbeenachieved(Fig.5).
Fig.2–Intraoperativeimagingshowingthegraftfromthe
semitendinosusinterlacedinthetricepstendon.
Thepatientevolvedinaverysatisfactorymanner.A com-plete range of motion was achieved and grade V muscle strengthwasreached,freefrompain.Thepatientisvery sat-isfiedwiththetreatmentthatwasperformed.
Discussion
Tearingofthedistaltendonofthetricepsisarareinjurythat accountsforlessthan1%ofalltendontears.1Thereislittle informationintheliteraturetoguidesurgicaltreatment.The
Fig.3–Intraoperativeimagingshowingthepositioningof
thetwoanchorsinananteriorpositionintheolecranon
Fig.4–Intraoperativeimagingshowingthefinalfixationof
thetendontotheolecranon.
meanageatwhichitoccursis36years(range:7–75),andit occursmorecommonlyinmales(3:1).6
This injury is generally caused by a fall to the ground withthewristextended,whichgeneratesaneccentric con-tractionofthetriceps.7Substantialforceisusuallyrequired forthetricepstendontotear;However,whenthestructural integrityofthetendonisaltered,tearingmayoccurasa conse-quenceofminimaltomoderateforce.7Hyperparathyroidism secondarytochronickidneydisease,hypocalcemia, rheuma-toidarthritis,imperfectosteogenesis,useofanabolicsteroids andinsulin-dependentdiabetesaresystemicfactorsthathave been reported asrelated totearing ofthe tricepstendon.7 Amongthelocalfactorsthathavebeencited,localinjectionof corticoids,degenerativearthritisandbursitisoftheolecranon havebeenthemostfrequent.7
Thediagnosis of acute tearingofthe triceps can easily gounnoticed.Whentearingoccurs,elbowextensionagainst gravitybecomesdifficultorimpossible.Apalpabledefect prox-imaltotheolecranonmaybedetected,butthelocalswelling inacutecasesmaylimitinitialidentification.7
Theradiographicfindings associatedwithtearingofthe distaltricepsareminimal.Avulsionofabonefragmentfrom thetipoftheolecranonhasbeendescribedintheliterature, andthis findingmay beveryuseful inmakingthe diagno-sis. MRIenables accurate demarcation of the location and extentoftheinjuryanditiscommonlythepreferred exami-nationformakingthediagnosis.5Finally,ultrasonographyhas beendescribedasanimportantdiagnosticmethodforthese injuries,giventhatitprovidesdynamicimagesandisamuch cheapermethodthanMRI,althoughthequalityoftheimages dependsonthetechniqueused.7
In most cases, complete tearing of the distal triceps is immediately treated surgically, comprising repair or reconstruction.7Ontheotherhand,incasesofpartialtearing,
Fig.5–Postoperativemagneticresonanceimaging
showingtendonhealedintheolecranon.
theinitialtreatmentisusuallynon-surgical.Whenpartorall ofthetendonhasbecomedetachedfromtheproximalulna andpersistentpain,weaknessorfunctionaldeficitispresent, primarysurgicaltreatmentshouldbeconsidered.8
Severalsurgicaltechniqueshavebeendescribedfor treat-ingpartialorcompletetearingofthetricepstendon.Primary repairofacute complete tearsusing non-absorbable sutur-ing with locking stitches across the tendon and passing through perforations in the olecranon has been proposed when possible.8 Anauto or allograftshould beused when primaryrepairisimpossible.8
InaseriespresentedbyvanRietetal.,7casesoftearingof thedistaltendonofthetricepswereidentified.Reconstruction wasnecessaryinninecasesandtransferofautogenoustissue wasnecessaryinsixpatients.Thetendonstransferredwere theAchilles, plantar, semitendinosus,latissimus,anconeus andpalmartendons.Ineachcase,thetendontransferredwas interlacedwiththedistalstumpofthetricepsandthesuturing waspassedthroughperforationsintheolecranon.7
Inthe case ofour patient, an autograftfrom the semi-tendinosushad tobeused,eventhoughthiswasacaseof partialtearing, becauseofthechronicnatureoftheinjury. Thetendon-graftcombinationwasfixedtotheolecranonby meansoftransosseoussuturingandsutureanchors,which reinforcedthefixationandmadeitmoresecure.
The technique described here is easy to carry out and enablesearlygainsofrangeofmotion,thusmaking active extensionofthe elbowpossiblesix weeksafterthe opera-tion, with good long-term functional results. We observed thatbecausethisisarareinjury, thereisgreatdifficulty in undertakinglargeprospectivestudiestocomparethe surgi-caltreatmentmethodsforthisinjury.However,thetechnique describedaboveseemstobeagoodoptionforcasesofchronic tearingofthedistaltriceps.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.AnzelSH,CoveyKW,WeinerAD,LipscombPR.Disruptionof musclesandtendons;ananalysisof1,014cases.Surgery. 1959;45(3):406–14.
2.AsoK,TorisuT.Musclebellytearofthetriceps.AmJSports Med.1984;12(6):485–7.
3.BachBRJr,WarrenRF,WickiewiczTL.Tricepsrupture.Acase reportandliteraturereview.AmJSportsMed.1987;15(3):285–9.
4.ShermanOH,SnyderSJ,FoxJM.Tricepstendonavulsionina professionalbodybuilder.Acasereport.AmJSportsMed. 1984;12(4):328–9.
5.ScolaroJA,BlakeMH,HuffmanGR.Tricepstendon
reconstructionusingipsilateralpalmarislongusautograftin unrecognizedchronictears.Orthopedics.2013;36(1):e117–20.
6.WeistrofferJK,MillsWJ,ShinAY.Recurrentruptureofthe tricepstendonrepairedwithhamstringtendonautograft augmentation:acasereportandrepairtechnique.JShoulder ElbowSurg.2003;12(2):193–6.
7.vanRietRP,MorreyBF,HoE,O’DriscollSW.Surgicaltreatment ofdistaltricepsruptures.JBoneJointSurgAm.
2003;85(10):1961–7.
8.MorreyBF.Ruptureofthetricepstendon.In:MorreyBF,editor. Theelbowanditsdisorders.Philadelphia:Saunders;2008.p. 536–46.