rev bras ortop.2017;52(6):676–684
SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
article
Dorsal
capsulodesis
associated
with
arthoscopy-assisted
scapholunate
ligament
reconstruction
using
a
palmaris
longus
tendon
graft
夽
Victor
Bignatto
Carvalho
a,
Carlos
Henrique
Vieira
Ferreira
b,
Andresa
Ramires
Hoshino
b,∗,
Viviane
Alves
Bernardo
b,
Gustavo
Mantovani
Ruggiero
b,
Márcio
Aurélio
Aita
baFaculdadedeMedicinadoABC,SantoAndré,SP,Brazil
bFaculdadedeMedicinadoABC,Servic¸odeOrtopediaeTraumatologia,SantoAndré,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received24September2016 Accepted1November2016 Availableonline28October2017
Keywords:
Lunatebone Jointinstability Arthroscopy Ligaments Articular
a
b
s
t
r
a
c
t
Objectives:Tomeasurethequalityoflife,thetimetoworkreturn,andclinical,functional, andradiographicparametersofpatientstreatedwithdorsalcapsulodesisassociatedwith scapholunate(SL)reconstruction,assistedbyarthroscopy.
Methods:FromJanuary2015toSeptember2016,14adultpatientswithSLdissociation under-wentsurgicaltreatmentwiththeSLreconstructionprocedureassistedbyarthroscopy,using thenewtechniqueproposedinthisstudy.Allpatientswereassessedbytheoccupational therapydepartmentatregularintervalsaftersurgeryandperformedthesamesequenceof rehabilitation.Theparametersanalyzedwere:rangeofmotion(ROM),DisabilityoftheArm, Shoulder,andHand(DASH),visualanalogscale(VAS),andradiographicanalysisto visu-alizethepre-andpostoperativeSLgapandthepre-andpostoperativedorsalintercalated segmentinstability(DISI)deformitythe.Thecomplicationsandthetimetoreturntowork activitiesweredescribed.
Results:Thefollow-uptimewas12months(3–17).TheROMaveraged321◦(96.9%ofthe
normalside).VASwas1.79/10(1–6).DASHwas6.50/100(1–30).Thetimetoworkreturnwork was4.42months(2–17).Asforcomplications,onepatientdevelopedSLAC,andunderwent four-cornerfusiononeyearafterligamentreconstruction.Currently,hehasexperienced painrelief,withafunctionalrangeofmotionofthewrist,andhasnot yetreturnedto professionalactivities.
ThepreoperativeSLgapwas4.29mm(2–7);inthepostoperativeperiod,itwas1.79mm (1–4).TheDISIdeformity waspresentinten patientswithSLangle>70◦ (preoperative)
anditwascorrectedaftersurgery,inallpatients.SLACstageIwasidentifiedinapatient.
Arthroscopywasperformedinallcases.TheSLinstabilitywasclassifiedasGeisslergrade
IIIinfourcasesandasgradeIVintencases.
夽
StudyconductedattheFaculdadedeMedicinadoABC,Servic¸odeOrtopediaeTraumatologia,SantoAndré,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](A.R.Hoshino). http://dx.doi.org/10.1016/j.rboe.2016.11.010
Conclusion: The newapproach (dorsal capsulodesis associatedwith SLreconstruction, assistedbyarthroscopy)presentedinthisstudyissafeandeffectiveinthetreatmentofSL dissociation,sinceitofferssatisfactoryclinical,radiographicandfunctionalresults,showing lowratesofcomplications.Forpatients,itallowsthereturntotheirsocialandprofessional activities,andincreasestheirlifequality.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Capsulodese
dorsal
associada
à
reconstruc¸ão
assistida
por
artroscopia
do
ligamento
escafossemilunar
com
enxerto
do
tendão
do
músculo
palmar
longo
Palavras-chave:
Ossosemilunar Instabilidadearticular Artroscopia
Ligamentosarticulares
r
e
s
u
m
o
Objetivos: Mensuraraqualidadedevida,otempoderetornoaotrabalho,osresultados clínicos,funcionaiseradiográficosdospacientessubmetidosàcapsulodesedorsalassociada àreconstruc¸ãoligamentarescafossemilunarassistidaporartroscopia.
Métodos: Dejaneirode2015asetembrode2016,14pacientes,esqueleticamentemaduros, adultos,comdissociac¸ãoescafolunar(SL),foramsubmetidosaotratamentocirúrgicocom oprocedimentodereconstruc¸ãodoligamentoescafossemilunarassistidoporartroscopia comanovatécnicapropostanesteestudo.Todosospacientesforamavaliadospelosetorde terapiaocupacionalemintervalosregularesdepós-operatórioefizeramamesmasequência dereabilitac¸ão.Osparâmetrosanalisadosforam:arcodemovimento(ADM),DisabilityArm, ShoulderandHand(Dash),escalavisualanalógica(EVA)eanáliseradiográficaprée pós-operatóriaparavisualizaroespac¸oescafolunar(sinaldeTerry-Thomas)edeformidadeem
DorsalIntercalatedSegmentInstability(DISI)préepós-operatória.Descric¸ãodascomplicac¸ões eotempoderetornoaotrabalho.
Resultados:Otempodeseguimentofoide12meses[3-17].OADMfoiemmédia321,07◦(96,9%
doladonormal).Ovalordaavaliac¸ãosubjetivadador(VAS)foi1,79/10[1-6].Amensurac¸ão daqualidadedevidapeloDashfoide6,50/100[1-30].Otempoderetornoaotrabalhofoide 4,42meses[2-17].Quantoàscomplicac¸ões,umapacienteevoluiucomSLACefoisubmetida àartrodesedosquatrocantosumanoapósareconstruc¸ãoligamentar.Evoluiucom mel-horiadadoreestácomoADMdopunhofuncional,masaindanãoretornouàsatividades profissionais.OintervalodoSL(gap)pré-operatóriofoide4,29mm[2-7]eopós-operatório foide1,79mm[1-4].AdeformidadeDISIestavapresenteemdezpacientes,comumângulo SLacimade70◦(pré-operatório),efoicorrigidaapósacirurgiaemtodosospacientes.SLAC
estágioIfoiidentificadoemumpaciente.Aartroscopiafoifeitaemtodososcasos.A
insta-bilidadeSLfoiclassificadacomoumgrauGeisslerIIIemquatrocasosegrauIVemdez
casos.
Conclusão: Anovaabordagem(capsulodesedorsalassociadaàreconstruc¸ãoligamentar escafossemilunarassistidaporartroscopia)apresentadanesteestudoéseguraeeficazno tratamentodadissociac¸ãoescafolunar,jáqueapresentaresultadosradiográficos,clínicos efuncionaissatisfatórios,demonstrabaixastaxasdecomplicac¸ões,permiteoretornoàs atividadessociaiseprofissionaiseaumentaaqualidadedevidadessespacientes.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Thescapholunate (SL) dissociation,or lesion ofthe SL lig-ament, is the most common form of carpal instability1
(Fig.1).
Numerous surgical techniques have been described to restoreorimprovethestabilityoftheSLjoint,aimingtodelay
orpreventtheprogressionofosteoarthrosisbetweencarpal bones,knownasSLadvancedcollapse(SLAC).
678
rev bras ortop.2017;52(6):676–684Fig.1–Radiographicaspectsofwrist–PAview–showing thescapholunategaportheTerry-Thomassign.
However,suchreconstructionsalterthebiomechanicsof the wrist, since they form a vertical connection between Gilula’sarcs,whichcanalterthemobilityoftheradiocarpal ormidcarpaljoints.
Thepersistenceofthe Terry-Thomas sign(gap between thescaphoidandlunate),looseningofthetendongraft, tech-nicaldifficulty,limitationofwristmobilityandpalmargrip strength,andiatrogenicfracturesduringthecreationofthe scaphoidorlunatetunnelshavebeenreportedasthemain complications.2–11 Theauthorsbelieve thatthese problems
canbeavoidedwiththedevelopmentofnewimplants,such asbio-tenodesisscrewsofspecificsizesforcarpalbones.
Furthermore,mostmethodsonlypromotethe reconstruc-tionofthedorsalanduniplanarportionoftheSLligament. Manystudies havehighlightedthe importanceofthe volar portionofthisligament.12–15
Thesearchfortheidealreconstruction(volaranddorsal portion)began with the biomechanicalstudy byYi et al.16
whousedatendongraftfromthelongpalmarismuscleand introducedit throughholesinthe anteroposteriorplaneof thescaphoidandlunate.TheSLgapwaseffectivelyreduced tonormal,andthe anatomicSLreductionwassignificantly improvedafterreconstruction.
Zderoetal.17assessed19cadaverwrists,andusedbovine
tendonspassedthroughdoublebonetunnelsofthescaphoid andlunate.Seventeenofthe19wristssubmittedtothis recon-structionpresented nodifference inmechanical properties whencomparedwiththenormalside.
Theresultsofthesestudiessupporttheclinicalapplication ofacombined SLligamentreconstruction technique(volar anddorsal).
Hoetal.18publishedaclinicalstudyof17patients,allwith
chronicSLdissociation,whounderwentarthroscopy-assisted reconstructionwiththeuseofafreetendongraftfromthe longpalmarmuscle(LPM);13patientsreturnedtotheir pre-viousworkactivities,allweresatisfiedwiththeresult,four evolvedwithrecurrenceofdorsalintercalatedsegmentation instability(DISI),andoneevolvedwithasymptomaticnecrosis oftheproximalpoleofthescaphoid.
Hagert et al.19 suggested that the wrist ligaments vary
withregardtosensoryandbiomechanicalfunctions. Depend-ingonthestructuralcompositionandinnervation,thewrist ligamentspresentgreatermechanical(denselypacked colla-genbundleswithlimitedinnervation)orsensorialrelevance (richlyinnervated,althoughlessdenseintheconnective tis-sue composition).Itisbelievedthat thedorsalcapsuleand theintrinsicligamentsofthewrist,includingtheSL,havean importantroleintheproprioceptionofthewrist.Thus,the authorssuggestthatsurgicalreconstructionshouldbe imme-diateatdiagnosisandthatthetreatmentmethodemployed shouldhaveaminimalimpactonthedorsalcapsuleofthe wrist.19–21
Overstraetenetal.22describedthepresenceofadistinct
structure,whichconnectstheSLligamenttothedorsal cap-sule,termeddorsalcapsulo-scapholunateseptum(DCSS).The authorsbelievethattheDCSSisasecondarystabilizeroftheSL joint,andthatitmayhavetherapeuticandprognostic impli-cations.Thecapsulodesistechniquesdescribedthusfarfavor this“reconnection”ofthedorsalcapsulewiththeSLligament. Wolfeetal.23conductedakinematicanalysisofthewrist
andshowedthattheproximalcarpalrowisalmoststationary duringthedartthrowmotion(DTM),whichisbelievedto pro-videastableplatformforthegenerationofforceandprecision duringcertainfunctionalactivities,suchaspalmar prehen-sion.Inordertoimprovetherehabilitationofpatientswho underwentwristligamentreconstruction,theauthorsbelieve thatDTMcanbeusedearlyinthefirstpostoperativeweeks, as itavoidsmuscular stiffnessand atrophyinthe affected limb,stimulatesproprioception,anddoesnotinterfereinthe healingofthereconstructedintrinsicligament.
Inthepresentstudy,anewapproachtothetreatmentof SLdissociationwillbedescribed,inordertoimprove clinical-functional outcomes,time-lapseforreturningtosocialand professional activities, surgical management, postoperative rehabilitation,andqualityoflifeofthesepatients.
Thisstudy isalsoaimedatassessingthequality oflife, returntowork,theclinical-functionalandradiographicresults of patients who underwent dorsal capsulodesis associated witharthroscopy-assistedSLligamentreconstruction.
Methods
From January2015toSeptember2016,14skeletallymature adultpatientswithSLdissociation,evaluatedattheoutpatient surgicalclinic,andwho underwentarthroscopy-assistedSL ligamentreconstructionwiththenewtechniqueproposedin thisstudy,wereassessed.
r
e
v
b
r
a
s
o
r
t
o
p
.
2
0
1
7;
5
2(6)
:676–684
679
Identification Age Follow-up Normal
ROM
Final ROM
Final DASH
Final VAS
Watson test
Geissler type
DISI SLgap
pre
SLgap
post
Return
towork
Complications Profession Associated
lesions
I 33 17 315 315 6 1 + 4 Yes 6 2 3rdmonth No Engineer No
II 36 16 345 345 6 1 + 4 Yes 7 4 3rdmonth No Nurse No
III 25 13 345 345 6 1 + 3 N 3 1 2ndmonth No Student Distalradius
fracture
IV 50 13 335 335 6 1 + 4 Yes 4 1 3rdmonth No Homemaker Distalradius
fracture
V 23 15 345 345 6 1 + 4 Yes 5 1 3rdmonth No Student No
VI 52 15 316 230 30 6 – 4 Yes 5 4 No SLAC Homemaker No
VII 60 14 335 335 6 2 + 4 Yes 5 1 6thmonth No Factoryworker Distalradius
fracture
VIII 58 15 295 270 18 1 + 4 Yes 5 2 6thmonth No Factoryworker No
IX 28 12 325 325 1 1 + 3 Yes 4 2 4thmonth No Factoryworker No
X 19 7 345 345 1 1 + 4 Yes 4 1 2ndmonth No Student Distalradius
fracture
XI 42 8 330 310 1 2 + 4 No 3 2 2ndmonth No TI No
XII 30 9 345 345 1 1 – 2 No 2 1 2ndmonth No Athlete No
XIII 52 6 315 315 1 1 + 2 No 3 1 3rdmonth No Homemaker No
XIV 23 3 340 335 2 1 + 3 Yes 4 2 3rdmonth No TI No
680
rev bras ortop.2017;52(6):676–684andeighthadsubjectivelossofstrengthandinstabilitywith apainfulclick.Inallpatients,physicalexaminationindicated painatpalpationattheSLgapsite.TheWatsontestwas pos-itivein12of14cases.
Allpatients were evaluatedbytheoccupationaltherapy sectoratregularpostoperativeintervalsandunderwentthe same rehabilitationsequence,followingthe same protocol, andwere evaluatedintwoand sixweeks,sixmonths,and oneyearpostoperatively(Table1).
Theassessedparameterswere:
- Range ofmotion(ROM),assessingthe goniometryofthe ROMwiththemeasurementindegrees.
- DisabilityArm,Shoulder,andHand(DASH)Questionnaire– qualityoflife.
- Visualanalogscale(VAS)–subjectivepainassessment. - Radiographicanalysis tovisualizepre-and postoperative
SLspace(Terry-Thomassign)andSLangle(normalvalues rangefrom30to60◦;DISIdeformitywasassessedwhenthe
anglewashigherthan70◦).
- Descriptionofthecomplicationsthataroseaftersurgical treatment.
- Returntowork.
Description
of
the
surgical
technique
Diagnosticarthroscopyis animportanttooltoidentifythe cause ofwristpainin caseswhereSLdissociationmay be associatedwithotherpathologies.
Thesurgerywasperformedundergeneralanesthesiaor locoregional blockade. The patient was placed in a dorsal recumbent position, withthe arm suspendedin a specific wristtractiontower,under10–13lboftraction.Atourniquet wasinflatedorpassed.Continuousirrigationwithsaline solu-tionwasachievedwithapumpandspecificequipmentunder theactionofgravity.
Aninventoryofthe radiocarpaljoint wasmadeinitially throughportals3–4,4–5,and6Uforthesalinesolutionexit; themidcarpaljointwasassessedthroughtheradial(MCR)and ulnar (MCU)portals. Small transverse incisions weremade alongtheskinfoldsforabetterscarappearance.Arthroscopes measuring1.9mmor2.7mmwereused.Thejointwas system-aticallyinspectedandthe resultsweredocumented. When necessary, radialsynovectomywas performed atthe same time,with2-mmand 2.9-mmshaverblades.Intra-articular fibrosiswasremovedtoimprovewristmobilityandto pro-motegapreductionand SLalignment,aswellastocorrect DISIdeformity.
Therebuildingstepwasinitiatedwitha2cmtransverse incisionalongtheproximaltransversefoldofthewrist(Fig.2) toidentifytheinsertionofthepalmarislongustendonandof theflexorcarpiradialistendon.Thepalmarislongusgraftwas extractedwithorwithouttheuseofatendonstripper.A2mm proximalincisionwasmadeinthefasciaoftheanterior fore-armtoidentifythemyotendinoustransitionofthepalmaris longus,inordertoexciseit.Bothdorsalandvolarjoint cap-suleswerepreserved,unaltered.Atthatmoment,the wrist wasreadyforthepreparationofthebonetunnels.
Fig.2–Preoperativeclinicalaspect:incisioninthe
transversepalmarfoldofthewristtolocatetheinsertionof thepalmarislongustendon.
Fluoroscopywasusedtoassessthewrist.IfaDISI defor-mity wasobserved, theextendedlunateposition wouldbe correctedbyflexionofthewristtorestorethenormal radioul-narangleandtheradioulnarjoint,withfixationornotwith a1.6-mmKirschnerwireinsertedpercutaneously.Thewrist wasthenpassivelyextendedtocorrecttheflexiondeformity ofthescaphoidandrestoreanormalSLangle.Ifthese cor-rectionswerenotachieved,additionalarthroscopicreleaseof thefibrosisaroundthescaphoidandlunatewasperformed.If itwasstillimpossibletoreducetheDISIdeformity,then lig-amentreconstructionwouldbeabandoned;fortunately,this didnotoccurinthisstudy.Throughthedorsalportals4–5or 6R,MCR,orMCU,a1.1-mmguidewirewasplacedinsidea soft-tissueprotector(drillguide)onthelunateandscaphoidunder fluoroscopicguidance.Whentheradiusandlunatewerewell alignedwiththeguidewire,thedirectionoftheradiusshould be perpendicular tothe long axisofthe lunate; i.e., paral-leltothelinejoiningthetipofvolaranddorsallipsofthe lunate(lateralview). Theguide wirewasadvanced2–3mm fromthebonemarginandthentowardthevolarcortex.With theflexortendonsandmediannerve,includingthepalmar cutaneousbranch,carefullymovedtotheulnarside,theexitof thiswirewasidentified.Anotherguidewirewastheninserted intothescaphoidthroughthe3–4dorsalportal.Itwasplaced paralleltothelunateguidewire,providedthattheSLangle hadbeencorrected.Otherwise,itsentranceshouldbeslightly moredistalthan thatofthelunateguidewire;it shouldbe movedtowardthepalmarandproximaldirectiontoprovide abettercorrectionofthescaphoidrotationandflexion.With theflexorcarpiradialistendonradiallymoved,thescaphoid wirewasadvancedthroughthevolarface.Bothtunnels(Fig.3) were sequentiallyenlargedwith2.0-,2.7-,or 3-mm cannu-lateddrills,dependingonthethicknessofthepalmarislongus graft.Thedrillofsmallestpossiblediametershouldbeused toensureasmoothpassageofthegraftandavoidiatrogenic fractureoravascularnecrosisofthesebones.
Fig.3–Intraoperativefluoroscopy:preparationofthe lunatebonetunnel.
Fig.4–Intraoperativeaspect–preparationofthepalmaris longustendongraft(Krackowsuture).
Fig.5–Intraoperativeclinicalaspect:preparationofthe scaphoidbonetunnel.
(grooved)needlesorwiresfromthepalmartothedorsalsideof thescaphoid(Figs.5and6)andfromthedorsaltothepalmar aspectofthelunate.Thetendongraftwaspassedoutsidethe
Fig.6–Intraoperativeclinicalaspect:thetendongraftis passedthroughthescaphoidbonetunnel(inapalmarto dorsaldirection),exitingtheskinthroughthedorsal arthroscopicportal3–4.
dorsalcapsule,sothatitwasreinsertedlinearlyundertheSL gap(linearcapsulodesis).
Thefixationofthegraft inthebonetunnelswitha bio-tenodesisscrew,measuring3mmindiameterand 8mmin length,alsocalled3/8mm(Bio-Tenodesisscrew,ArthrexInc., FL,USA)wasperformed.Thefinalpartofthegraftwassutured atthe same siteofthe graft entrypointinto the scaphoid (reconstructionofthepalmarportionoftheSLligament).The Kirschner wirewaspassedbetweenthe scaphoidand cap-itatebonesforstabilizationoftheligament reconstruction. Themidcarpaljoint wasonce againinspectedthrough the MCRorMCUportal.TheSLgapwasonceagaininspectedwith probetweezers,asdescribedbyGeissler(Fig.7).Thisinterval shouldbeclosed.AnytissueinterpositionintheSLgap pre-ventingacompletereduction,wasarthroscopicallyremoved. SLstabilitywasconfirmedbyarthroscopyandfluoroscopy.
Thelayerswere cleanedandsutured,and aplastercast wasplaced.Twoweekspostoperatively,theplastercastand the Kirschnerwiresthat maintainedtheSLreductionwere removedfromthecarpalbones;allpatientsstarted rehabili-tationinoccupationaltherapy.
Results
Thefollow-uptimewas12months(3–17).ThemeanROMwas 321.07◦(96.9%ofthenormalside).Themeansubjectivepain
assessment(VAS)was1.79/10 (1–6).ThemeanDASHscore, whichassessesqualityoflife,was6.50/100(1–30).
682
rev bras ortop.2017;52(6):676–684Lunate
Scaphoid
Fig.7–Intraoperativeaspectofwristarthroscopy:the probeisplacedintheSLgap,andtheclosureofthe scapholunategapisverified,asdescribedbyGeissler.
functionalwristROM,buthasnotyetreturnedtoprofessional activities.
Inthepreoperativeperiod,themeanSLgapwas4.29mm (2–7), vs.1.79mm(1–4) postoperatively.DISI deformitywas observed in ten patients, with an SL angle of more than 70◦,priortotheprocedure,and wascorrectedaftersurgery
inall patients. SLAC stageI was identified in onepatient.
Arthroscopywas performed inall cases. SLinstabilitywas classifiedas aGeisslergradeIII infourcasesand gradeIV
intencases.Otherarthroscopyfindingswereradial synovi-tisin11patients,degenerationoftheradialstyloidcartilage inone,chondrallesioninthescaphoidfossaoftheradiusin two,proximalscaphoidchondraldefectinone,and triangu-larfibrocartilagecomplexlesion(TFCC)intwo.Concomitant procedures were performed in six cases, including TFCC debridementinone,radiusosteosynthesisinfour,andTFCC repairinone.Nocasesofinfectionorneurovascular compli-cationswereobservedinthepresentseries.
Results
Forstatistical analyses,ap-valueof5%(0.050) was consid-eredassignificantfortheapplicationofthestatisticaltests (Table2).
MS-Excelspreadsheet,initsversionfromMS-Office2013, wasusedtoorganizethedata.Thestatisticalpackage Statisti-calPackageforSocialSciences(SPSS),version23.0,wasusedto applytheWilcoxonsignaledranktest,inordertoverify pos-sibledifferencesbetweenthetwomomentsstudied,forthe variablesofinterest.
Discussion
Theideaofreconstructingthisligamentisnotnew.In1975, Dobynsetal.24usedastripoftendonandpasseditthrough
anteroposterior bone tunnels at the proximal pole of the
scaphoidandlunatetorebuildtheSLligament.Stabilitywas achievedbyloopingthetendongraftthroughoutthescaphoid and lunate. However, the open creation of bone tunnels compromised theirvascularization andresulted in avascu-larnecrosisand fractures.Thisapproachwassubsequently abandoned.Thepresentarthroscopicseriesdidnotrequire dissectionofthejointcapsuleandthuspreservedthe vascu-larsupplyandproprioceptionofthecarpus.21Thisminimally
invasivetechniquehelpstominimizesoft tissuedissection anddecreasestheriskofavascularnecrosis,promoteshealing ofthereconstructedSLligament,andacceleratesthe postop-erativerehabilitation.
Theresultsofthepresentstudydemonstratedan improve-mentinwristmobility,witha96.9%recoveryofROMwhen comparedwiththenormalside.Thepresentresultsare sim-ilar to those by Ho et al.18 However, the present authors
disagree with those authors. Ho et al. stated that dorsal capsulodesis decreases flexionofthe wrist,which wasnot demonstrated in the present study. The present authors believethatthelinearcapsulodesisperformedinthepresent study,limitedtotheSLgap,didnotinterfereinthemobility ofthemidcarpaljoint.
Wahegaonkaretal.25statedthatthedorsalportionofthe
SLligament(DCSS)isparamountforSLstability,largelydueto itsattachmenttothedorsalcapsule.Theseauthorsconducted amulticenteranatomicalstudywithinternational collabora-tionanddemonstratedthecriticalimportanceofDCSS.The arthroscopiccapsule-ligamentrepairtechniqueprovided reli-able resultsand avoidedpostoperativestiffness.Theglobal resultsover amean follow-upperiodofovertwoyears are encouraging.Theauthorsbelievethatthecapsulodesis per-formedinthepresentstudyallowedcontinuityoftheligament withthedorsalcapsule,aswellasDCSSreconstruction.
Thechoiceofthepalmarislongustendongraft,usedinthis andotherpublishedstudies,offerssomeadvantages:
- the diameter of the bone tunnels can be minimal; it avoidscomplicationssuchasiatrogenicfracturesor vascu-larlesionsofcarpalbones;
- italsopreservestheflexorcarpiradialis,whichtheauthors believetobeanimportantsecondarystabilizerofthewrist, helpingtheuseofDTMintherehabilitationstages.23
The recurrence of the SL gap (Terry-Thomas sign) is commonly cited inthe literature,3 and the present results
demonstrated a maintenance of the SL gap reduction of 1.79mm(Fig.8).
Replacingaligamentwithatendonmaynotactually repro-ducetheoriginalanatomyoftheSLcomplex.However,the authorsbelieveinthe“ligamentization”ofthesegrafts,since theenvironmentinwhichtheyarefoundmayfavorthis mech-anism,similarlytowhatisobservedinpatientswhoundergo anteriorcruciateligament(ACL)reconstruction.26
Whenrebuildingboththevolaranddorsalportionsofthis ligament,greaterstabilityandefficacycanbeexpectedwhen comparedwiththemorecommondorsalreconstructions.
Many cadaveric studies support 360◦ reconstruction
around the carpal bones, with favorable biomechanical results.15–17 Other clinical studies have shown promising
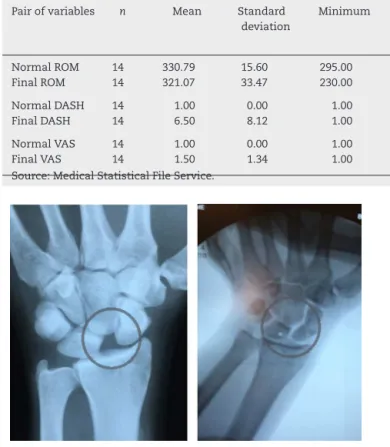
Table2–Statisticalresultsoftheanalyzedclinical-functionalvariables.
Pairofvariables n Mean Standard
deviation
Minimum Maximum 25th
percentile
50th percentile
(median)
75th percentile
Significance
(p)
NormalROM 14 330.79 15.60 295.00 345.00 315.75 335.00 345.00 [1,0]
0.068
FinalROM 14 321.07 33.47 230.00 345.00 313.75 335.00 345.00
NormalDASH 14 1.00 0.00 1.00 1.00 1.00 1.00 1.00 [1,0]
0.006
FinalDASH 14 6.50 8.12 1.00 30.00 1.00 6.00 6.00
NormalVAS 14 1.00 0.00 1.00 1.00 1.00 1.00 1.00 [1,0]
0.102
FinalVAS 14 1.50 1.34 1.00 6.00 1.00 1.00 1.25
Source:MedicalStatisticalFileService.
Fig.8–Pre-andpostoperativeradiographicviewsthat demonstratethemaintenanceofSLgapreduction.
dorsalandpalmarreconstructionandobtainedgoodclinical results,whichwerealsodemonstratedinthepresentstudy.27
TheidealtreatmentforSLdissociationhasnotyetbeen established.Theauthors believe thatthe reconstruction of bothportionsoftheSLligament,associatedwithlinear dor-salcapsulodesis,graftfixationwithspecificscrews,andthe useoftheDTMduringimmediatepostoperativerehabilitation decreasestheperiodofimmobilization(ofonlytwoweeksin thispresentstudy)andtheratesofcomplication,allowingan earlyreturntosocialandprofessionalactivities.
Conclusion
The new approach (dorsal capsulodesis associated with arthroscopic-assistedSLligamentreconstruction)presented inthisstudyissafeandeffectiveinthetreatmentofSL dis-sociation,sinceitpresentssatisfactoryradiographic,clinical, andfunctionalresults,aswellaslowratesofcomplications, allowingthereturntosocialandprofessionalactivitiesand increasingthequalityoflifeofthesepatients.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.DanielsJMII,ZookEG,LynchJM.Handandwristinjuries:Part I.Nonemergentevaluation.AmFamPhysician.
2004;69(8):1941–8.
2.MoranSL,FordKS,WulfCA,CooneyWP.Outcomesofdorsal capsulodesisandtenodesisfortreatmentofscapholunate instability.JHandSurgAm.2006;31(9):1438–46.
3.LinscheidRL,DobynsJH.Treatmentofscapholunate
dissociation.Rotatorysubluxationofthescaphoid.HandClin. 1992;8(4):645–52.
4.AlmquistEE,BachAW,SackJT,FuhsSE,NewmanDM. Four-boneligamentreconstructionfortreatmentofchronic completescapholunateseparation.JHandSurgAm. 1991;16(2):322–7.
5.BrunelliGA,BrunelliGR.Anewtechniquetocorrectcarpal instabilitywithscaphoidrotarysubluxation:apreliminary report.JHandSurgAm.1995;203Pt2:S82–5.
6.VanDenAbbeeleKL,LohYC,StanleyJK,TrailIA.Earlyresults ofamodifiedBrunelliprocedureforscapholunateinstability. JHandSurgBr.1998;23(2):258–61.
7.TalwalkarSC,EdwardsAT,HaytonMJ,StilwellJH,TrailIA, StanleyJK.Resultsoftri-ligamenttenodesis:amodified Brunelliprocedureinthemanagementofscapholunate instability.JHandSurgBr.2006;31(1):110–7.
8.ChabasJF,GayA,ValentiD,GuinardD,LegreR.Resultsofthe modifiedBrunellitenodesisfortreatmentofscapholunate instability:aretrospectivestudyof19patients.JHandSurg Am.2008;33(9):1469–77.
9.Garcia-EliasM,LluchAL,StanleyJK.Three-ligamenttenodesis forthetreatmentofscapholunatedissociation:indications andsurgicaltechnique.JHandSurgAm.2006;31(1): 125–34.
10.GlickelSZ,MillenderLH.Ligamentousreconstructionfor chronicintercarpalinstability.JHandSurgAm.
1984;9(4):514–27.
11.TaleisnikJ.Wristanatomyfunctionandinjury.Instructional courselectures.TheAmericanAcademyofOrthopaedic Surgeons,vol.27.StLouis:Mosby;1978.p.61–87. 12.MayfieldJK.Patternsofinjurytocarpalligaments.A
spectrum.ClinOrthopRelatRes.1984;(187):36–42.
13.MeadeTD,SchneiderLH,CherryK.Radiographicanalysisof selectiveligamentsectioningatthecarpalscaphoid:a cadaverstudy.JHandSurgAm.1990;15(6):855–62.
14.DunnMJ,JohnsonC.Staticscapholunatedissociation:anew reconstructiontechniqueusingavolaranddorsalapproach inacadavermodel.JHandSurgAm.2001;26(4):749–54. 15.ShortWH,WernerFW,SuttonLG.Dynamicbiomechanical
evaluationofthedorsalintercarpalligamentrepairfor scapholunateinstability.JHandSurgAm.2009;34(4):652–9. 16.YiIS,FiroozbakhshK,RaccaJ,UmedaY,MoneimM.
684
rev bras ortop.2017;52(6):676–684tendongraft:abiomechanicalstudy.UnivPaOrthopJ. 2000;13:53–9.
17.ZderoR,OlsenM,ElfatoriS,SkrinskasT,NourhosseiniH, WhyneC,etal.Linearandtorsionalmechanical characteristicsofintactandreconstructedscapholunate ligaments.JBiomechEng.2009;131(4):041009.
18.HoPC,WongCW,TseWL.Arthroscopic-assistedcombined dorsalandvolarscapholunateligamentreconstructionwith tendongraftforchronicSLinstability.JWristSurg.
2015;4(4):252–63.
19.HagertE,LjungBO,ForsgrenS.Generalinnervationpattern andsensorycorpusclesinthescapholunateinterosseous ligament.CellsTissuesOrgans.2004;177(1):47–54.
20.HagertE,ForsgrenS,LjungBO.Differencesinthepresenceof mechanoreceptorsandnervestructuresbetweenwrist ligamentsmayimplydifferentialrolesinwriststabilization.J OrthopRes.2005;23(4):757–63.
21.HagertE,Garcia-EliasM,ForsgrenS,LjungBO.
Immunohistochemicalanalysisofwristligamentinnervation inrelationtotheirstructuralcomposition.JHandSurgAm. 2007;32(1):30–6.
22.OverstraetenLV,CamusEJ,WahegaonkarA,MessinaJ, TandaraAA,BinderAC,etal.Anatomicaldescriptionofthe
dorsalcapsulo-scapholunateseptum(DCSS)–arthroscopic stagingofscapholunateinstabilityafterDCSSsectioning.J WristSurg.2013;2(2):149–54.
23.WolfeSW,CriscoJJ,OrrCM,MarzkeMW.Thedart-throwing motionofthewrist:isituniquetohumans?JHandSurgAm. 2006;31(9):1429–37.
24.DobynsJH,LinscheidRL,ChaoEY,WeberER,SwansonGE. Traumaticinstabilityofthewrist.Instructionalcourse lectures.TheAmericanAcademyofOrthopaedicSurgeons, vol.24.St.Louis:Mosby;1975.p.182–99.
25.WahegaonkarAL,MathoulinCL.Arthroscopicdorsal capsulo-ligamentousrepairinthetreatmentofchronic scapho-lunateligamenttears.JWristSurg.2013;2(2):141–8. 26.ClaesS,VerdonkP,ForsythR,BellemansJ.The
ligamentizationprocessinanteriorcruciateligament reconstruction:whathappenstothehumangraft?A systematicreviewoftheliterature.AmJSportsMed. 2011;39(11):2476–83.