SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
article
Spinopelvic
balance
evaluation
of
patients
with
degenerative
spondylolisthesis
L4L5
and
L4L5
herniated
disc
who
underwent
surgery
夽
Viviane
Regina
Hernandez
Nunes
a,
Charbel
Jacob
Junior
b,∗,
Igor
Machado
Cardoso
b,
José
Lucas
Batista
Junior
b,
Marcus
Alexandre
Novo
Brazolino
b,
Thiago
Cardoso
Maia
baUniversidadeVilaVelha,VilaVelha,ES,Brazil
bHospitalSantaCasadeMisericórdiadeVitória,GrupodeColuna,Vitória,ES,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received26September2015
Accepted8November2015
Availableonline22September2016
Keywords:
Intervertebraldiscdegeneration Spine
Spondylolisthesis Retrospectivestudies
a
b
s
t
r
a
c
t
Objective:Tocorrelatespinopelvicbalancewiththedevelopmentofdegenerative spondy-lolisthesisanddiskherniation.
Methods:Thiswasadescriptiveretrospectivestudythatevaluated60patientsinthis hospi-tal,30patientswithdegenerativespondylolisthesisattheL4–L5leveland30withherniated diskattheL4–L5level,allofwhomunderwentSurgicaltreatment.
Results:PatientswithlumbardiskherniationatL4–L5levelhadameantiltof8.06,mean slopeof36.93,andmeanPIof45.Inpatientswithdegenerativespondylolisthesisatthe L4–L5level,ameantiltof22.1,meanslopeof38.3,andmeanPIof61.4wereobserved.
Conclusion:ThisarticlereinforcesthefindingthatthehighmeantiltandPIarerelatedto theonsetofdegenerativespondylolisthesis,andalsoconcludedthatthesameangles,when low,increasetheriskfordiskherniation.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Avaliac¸ão
do
equilíbrio
espinopélvico
dos
pacientes
com
espondilolistese
degenerativa
L4L5
e
hérnia
de
disco
L4L5
submetidos
a
cirurgia
Palavras-chave:
Degenerac¸ãododiscointervertebral Colunavertebral
Espondilolistese Estudosretrospectivos
r
e
s
u
m
o
Objetivo:Correlacionaroequilíbrioespinopélvicocomodesenvolvimentode espondilolis-tesedegenerativaehérniadiscal.
Métodos:Estudoretrospectivodecaráterdescritivo,noqualforamavaliados60pacientes, 30portadoresdeespondilolistesedegenerativanonívelL4-L5e30portadoresdehérniade discononívelL4-L5,todossubmetidosatratamentocirúrgico.
夽
StudyconductedattheHospitalSantaCasadeMisericórdiadeVitória,Vitória,ES,Brazil. ∗ Correspondingauthor.
E-mail:[email protected](C.JacobJunior).
http://dx.doi.org/10.1016/j.rboe.2016.09.003
Resultados: OspacientesportadoresdehérniadediscolombarnonívelL4-L5apresentaram umamédiadainclinac¸ãopélvica(TILT)de8,06,dainclinac¸ãosacral(SLOP)de36,93eda incidênciapélvica(IP)de45.Nospacientesportadores espondilolistesedegenerativano nívelL4-L5foiobservadaumamédiadaTILTde22,1,daSLOPde38,3edaIPde61,4.
Conclusão: Opresenteartigoreforc¸aadescobertadequeaselevadasmédiasobtidasda TILTedaIPestãorelacionadascomosurgimentodaespondilolistesedegenerativaeainda concluiqueosmesmosângulos,quandobaixos,aumentamoriscoparahérniadedisco.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Lumbardischerniationisanintervertebraldisplacementof thenucleuspulposusthroughtheannulusfibrosus;itoccurs mainlybetweenthe4thand5thdecadeoflife,anditis esti-matedthat2%to3%ofthepopulationmaybeaffected,with ahigherprevalenceinmen.1,2Inturn,degenerative spondy-lolisthesisisdefinedasaslippageofalumbarvertebrawith anintactneuralarch,whichoccursmostlyinadultsover40 years,withapredilectionforfemales.3–5Bothdiseaseshavea multifactorialetiologythatmaybeassociatedwithsmoking, sedentarylifestyle,andobesity,aswellasgenetic predispo-sitionandanatomicalchanges.1,2,4,6Spinopelvicbalancehas beenincreasinglystudiedindegenerativediseasesofthe lum-barspineasanimportantfactorinthedevelopmentofthese diseases.Spinopelvicbalanceistheinteractionofthespine morphologywiththepelvis,anddirectlyimpactsthe mechan-icalbehaviorof thediscs, ligaments,and muscle strength.
These mechanisms allowthe individual to remain upright
andmove,minimizingenergyexpenditure.2,7–10Currently,the treatmentofthesepathologiesisconservative;incaseswith greatersymptomseverityandlackofresponsetoconservative treatment,surgicaltreatmentisindicated.2,11
Although diseases such as lumbar disc herniation and
degenerativespondylolisthesisarecommoninthepopulation, nostudiesthatassessedandcomparedspinopelvicbalancein thesepatientswereretrievedfromtheliterature.Therefore,
theauthors conductedthepresent studyinorder tobetter
understandspinopelvicbalance,therelationshipofits
biome-chanicswiththedevelopmentofspondylolisthesisanddisc
herniation,aswellastobeabletomakeanearlyidentification ofpatientsatriskofdevelopingthesediseases.By understand-ingspinopelvicbalance,preventivemeasuresorevenbetter treatmentforthesediseasescanbedeveloped.
Methods
Thiswasadescriptiveandretrospectivestudythatevaluated 60patients,30withdegenerativespondylolisthesisatL4–L5, and30withdischerniationattheL4–L5level,all ofwhom underwentsurgicaltreatment.Allpatientswereassessedby lumbopelvicradiographyinprofile;magneticresonance imag-ingwasalsousedforthediagnosisofdischerniation.
Inclusion criteria in group I were patients with lumbar
herniationatL4–L5andrefractorytoconservativetreatment
after 20 physiotherapy sessions without instability criteria
observedatlumbarradiography.GroupII includedpatients
withdegenerativespondylolisthesisattheL4–L5level,
classi-fiedaccordingtoWiltse,Newman,andMacnab,withfailure
ofconservativetreatmentwithphysicaltherapyand medica-tionforanalgesia.Bothgroupsofpatientsunderwentsurgical treatmentatHospitalSantaCasadeMisericórdiadeVitoria (ES).
Exclusioncriteriacomprisedpatientswithherniateddisc atotherlevels,thoselosttofollow-up,orthosewhodidnot undergo surgicaltreatment.IngroupII,patientswithother typesofspondylolisthesis,atlevelsotherthanL4–L5,orwho didnotundergosurgicaltreatmentwereexcluded.
Toassessspinopelvicbalance,X-rayimaginginorthostatic position(Fig.1)wasused,inwhichthefollowingcouldbe ana-lyzed: pelvicincidence(PI), throughthe intersection ofthe linesthatpassthroughthemidpointofbothcentersofthe
femoralheadsand themidpointofthesacralplateauwith
thelineperpendiculartothesacralplateau;sacralslope(SS), assessedthroughtheintersectionoflinesparalleltothesacral plateauandparalleltotheground;andpelvictilt(PT),which wasassessedbytheintersectionofthelinesthatcrossthe
midpointofbothcentersofthefemoralheadsandthe
mid-pointofthesacralplateauwiththelineperpendiculartothe ground.
Slope e
a
b PI c
d
Tilt
Results
Theassessmentoftheparametersinvolvedinspinopelvic bal-anceinpatientswithlumbardischerniationattheL4–L5level indicatedameanPTof8.06,meanSSof36.93,andmeanPIof 45(Table1).Inturn,ameanPTof2.1,meanSSof38.3,and
meanPIof61.4wasobservedinpatientswithdegenerative
spondylolisthesisattheL4–L5level(Table1).
After statistical analysis, the variables were compared
usingStudent’st-test,whichindicatedthatmeanSSresults didnotdifferbetweengroupsofherniateddiscand spondy-lolisthesis.Thiswasdemonstratedwithap-valueabove5% (p=0.483).Inturn,meanPIandPTvariables presented sta-tistically significant differences between groups, both with significancelevelslowerthan5%(p=0.000forboth).
Discussion
Properspinopelvic balance allowstheindividual toremain
uprightinastablemannerwithaminimumofmusculareffort; itsimbalancecausespainanddecreasedqualityoflife.
Spinopelvicbalance is determinedbythe association of
pelvicalignment withthe lumbar spine. Inthis geometric
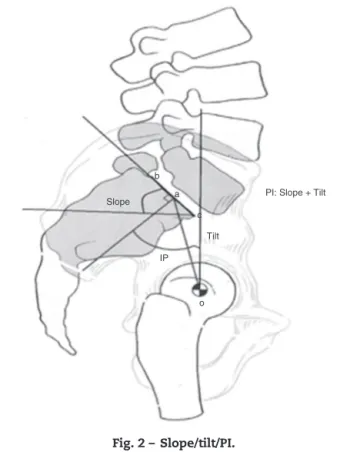
construction,thesuperiorangleoftheS1endplatewitha hor-izontalline(sacralslope)isequaltothelowerlumbarlordosis angle.Throughprofileradiograph,thepelvicreferencepoints canbeidentified,whichcontributetodeterminesagittal bal-ance,includingthesuperiorpointoftheS1endplateandthe centerofthefemoralhead.Throughthesepoints,threeangles canbedetermined:PI,PT,andSS.PIisthesumofPTandSS; therefore,PIisstrongdeterminantofthespatialorientation ofthepelvisinthestandingposition,i.e.,thehigherthePI, thehigherisPT,orSS,orboth(Fig.2).Itisimportantto under-standthatPIisameasureofastaticstructure,whilePTand SSvaryaccordingtowhetherthepatientisintheuprightor sittingposition,astheyassesstheangleofthesacrum/pelvis inrelationtothefemoralhead.10
Degenerativespondylolisthesisisdefinedastheslippage
of the lumbar vertebra with an intact neural arch,
occur-ring mainly between L4–L5. With this sliding, the entire
trunk moves along with the changed vertebra, resulting
in clinical consequences for the patient. The association
betweenexcess weightand a relative verticalslope ofthe
S1 endplate increases the chances of an anterior slip at
theL4–L5level. Other factorsalsopredisposemechanically
and non-pathogenically to degenerative spondylolisthesis.
These include sagittal orientation, osteoarthritis of the
Table1–Analysisofthemeansofspinopelvicbalance
parametersusingStudent’st-test.
Dischernia Spondylolisthesis
Tilt 8.06 22.1
Slope 36.93 38.3
PI 45.0 61.4
PI: Slope + Tilt
Tilt
IP Slope
b
a
c
o
Fig.2–Slope/tilt/PI.
joints,paraspinalmusculardystrophy,andlossofligament strength.4
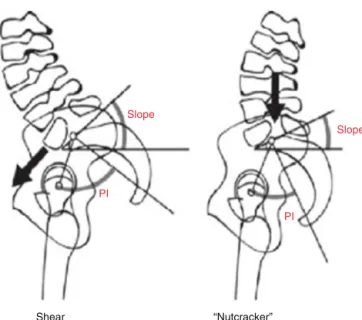
Notall patientswithspondylolisthesishavethesamePI angle.Spondylolisthesiscanbeclassifiedashigh-grade(group 0,1,or2,orsliphigherthan50%)andlowgrade(groups3and 4orsliplessthan50%).5,11AccordingtoLabelleetal.,11 low-gradespondylolisthesisisdivided intothreegroups: type1 (nutcrackertype)withPI<45◦;type2withnormalPI(between 45◦ and 60◦); andtype3,withPI>60◦ (sheartype). Accord-ingtotheseauthors,patientswithhighPIandhighSShave
increased shear forces in the lumbosacral junction, which
causesgreaterstrainonjointsandthesheartype.Moreover, patientswithlowPIandlowSSmaypresentanimpactonthe posteriorelementsbetweenofL5,L4,andS1duringextension, whichcausesanutcrackereffect(Fig.3).
High-grade spondylolisthesisisdivided into twogroups: balancedandunbalancedpelvicpositioning(Fig.4).The
bal-anced groupincludespatientswho present highslope and
lowtiltintheorthostaticposition.Patientsintheunbalanced grouppresent,inthestandingposition,pelvisinretroversion andaverticalsacrum,whichcorrespondstolowSSandhigh PT.5,10 Ithasbeendemonstratedthatalmostall individuals withhighvertebralslippagehaveameanPI>60◦.5
Forcesgeneratedbyanincreaseinlumbarlordosisleadto developmentandprogressionofspondylolisthesis.Increased PIisassociatedwithincreasedlumbarlordosis,which
predis-posestomechanicalchangesofthelumbarandlumbosacral
junction and increases the risk of spondylolisthesis.2,12
Slope
PI
Slope
PI
“Nutcracker” Shear
Fig.3–Shearandnutcrackertypes.
Aherniateddisc isrepresentedclinicallybypainknown assciatica,whichistriggeredbythemechanicalcompression
on the nerve root caused by disc herniation. Conservative
treatment with physical therapy and medication for pain
controlisusuallyeffective.Onlyasmallpercentageofthese patientsrequiresurgery.Thisisamultifactorialdisease;the
present article associated spinopelvic imbalance with the
emergenceofthisdisease.1,2
Anasymptomaticpopulationwithnohistoryoforthopedic diseasewasassessedinthestudybyRoussoulyetal.,2in2005, whichshowedameanPIangleof51.9◦.Intheirstudy,Schuller etal.4 concludedthathigherPImakestheindividual more susceptibletodevelopingdegenerativespondylolisthesis,and facilitatesitsprogression.
Retroverted pelvis Balanced pelvis
Fig.4–Balancedandretrovertedpelvicposture.
Source:TibetMA.Conceitosatuaissobreoequilíbriosagital
eclassificac¸ãodaespondilóliseeespondilolistese.2014;49 (1):3–12.
Inthepresentstudy,patientswithspondylolisthesishada meanPIof61.4◦;thosewithdischerniationhadameanPIof 45◦.ThisprovesthatpatientswithhigherPIhaveincreased riskofspondylolisthesisand those withlowerPIpresent a higherriskfordischerniation.
Conclusion
Thisarticlereinforcedthefindingthatthehighmeanvaluesof PIandPTarerelatedtotheonsetofdegenerative spondylolis-thesis;thestudyalsoconcludedthatthesameangles,when low,increasetheriskfordischerniation.Itwasalsopossible toconcludethat PTandSSare inverselyproportional vari-ables.However,bothvariablesaredirectlyproportionaltoPI; SSisavariableoflowsignificancebetweenthetwo patholo-gies.Therefore,onlyPIandPTcontributetotheidentification ofriskforspondylolisthesisandherniateddisc,whentheyare highorlow,respectively.
Itcanbeconcludedthatspinopelvicimbalanceisarisk fac-torfortheemergenceofherniateddiscandspondylolisthesis.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.VialleLR,VialleEN,HenaoJES,GiraldoG.Hérniadiscal lombar.RevBrasOrtop.2010;45(1):17–22.
2.RoussoulyP,GolloglyS,BerthonnaudE,DimnetJ. Classificationofthenormalvariationinthesagittal alignmentofthehumanlumbarspineandpelvisinthe standingposition.Spine(PhilaPa1976).2005;30(3):346–53.
3.LoveTW,FaganAB,FraserRD.Degenerative
spondylolisthesis.Developmentaloracquired?JBoneJoint SurgBr.1999;81(4):670–4.
4.SchullerS,CharlesYP,SteibJP.Sagittalspinopelvicalignment andbodymassindexinpatientswithdegenerative
spondylolisthesis.EurSpineJ.2011;20(5):713–9.
5.TebetMA.Conceitosatuaissobreequilíbriosagitale classificac¸ãodaespondilóliseeespondilolistese.RevBras Ortop.2014;49(1):3–12.
6.JacobsenS,Sonne-HolmS,RovsingH,MonradH,GebuhrP. Degenerativelumbarspondylolisthesis:anepidemiological perspective.TheCopenhagenOsteoarthritisStudy.Spine (PhilaPa1976).2007;32(1):120–5.
7.BarreyC,RoussoulyP,PerrinG,LeHuecJC.Sagittalbalance disordersinseveredegenerativespine.Canweidentifythe compensatorymechanisms?EurSpineJ.2011;20Suppl. 5:626–33.
8.GottfriedON,DaubsMD,PatelAA,DaileyAT,BrodkeDS. Spinopelvicparametersinpostfusionflatbackdeformity patients.SpineJ.2009;9(8):639–47.
9.RajnicsP,TemplierA,SkalliW,LavasteF,IllesT.The importanceofspinopelvicparametersinpatientswith lumbardisclesions.IntOrthop.2002;26(2):104–8.
10.BarreyC,JundJ,NosedaO,RoussoulyP.Sagittalbalanceofthe pelvis–spinecomplexandlumbardegenerativediseases.A comparativestudyabout85cases.EurSpineJ.
11.LabelleH,Mac-ThiongJM,RoussoulyP.Spino-pelvicsagittal balanceofspondylolisthesis:areviewandclassification.Eur SpineJ.2011;20Suppl.5:641–6.
12.VialleR,IlharrebordeB,DauzacC,GuiguiP.Intraand inter-observerreliabilityofdeterminingdegreeofpelvic
incidenceinhigh-gradespondylolisthesisusingacomputer assistedmethod.EurSpineJ.2006;15(10):