www.jped.com.br
ORIGINAL
ARTICLE
Quality
Assessment
of
Neonatal
Transport
performed
by
the
Mobile
Emergency
Medical
Services
(SAMU)
夽
Juliana
C.F.
Romanzeira,
Silvia
W.
Sarinho
∗UniversidadeFederaldePernambuco(UFPE),Recife,PE,Brazil
Received1September2014;accepted14October2014 Availableonline23April2015
KEYWORDS
Transportservices; Newborn;
EmergencyMedical Services
Abstract
Objective: Toassess thequality of neonataltransportperformed by theMobile Emergency MedicalServices(Servic¸odeAtendimentoMóveldeUrgência[SAMU]).
Methods: Thiswasacross-sectionalbefore-and-afterobservationalstudy.Thestudywascarried outfromMarchtoAugustof2013usingavalidatedinstrument,theTransportRiskIndexof Phys-iologicStability(TRIPS),toassessthecharacteristicsofthenewborn,medicalandmechanical complications(equipmentandambulance),andstabilityofnewbornsbeforeandafter trans-port.Testswereconductedwith95%confidencelevel.Numericalvariablesarerepresentedby measuresofcentraltendencyanddispersion.CategoricalvariableswerecomparedbyFisher’s exacttest.Inthecomparisonofvariablesbetweenthegroups,theStudent’st-testwasusedfor variableswithnormaldistribution,Fisherexacttest,whenappropriate,andtheMann-Whitney test,fornon-normaldistribution.
Results: 33newbornsweretransportedfromlow-riskunitstoneonatalintensivecareunits. Male gender (57.6%) and full-term gestational age (63.6%) were more prevalent. Birth weight<2,500g was found in 39.4% of newborns. Respiratory failure accounted for 42.4% of the requests. The mean transport time was 58minutes without medical or mechanical complications. The TRIPSscore worsened in 15%of neonates; inthisgroup of infants,the meaninitialtemperatureof36.46±0.19decreasedsignificantlyto36.08±0.22(p=0.041). Conclusion: ThetransportperformedbytheSAMUwasadequateformostnewborns.The oscil-lationinbody temperaturewas theonlysignificantvariable forthe alterationintheTRIPS score.
©2015SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Allrightsreserved.
夽
Pleasecitethisarticleas:RomanzeiraJC,SarinhoSW.QualityAssessmentofNeonatalTransportperformedbytheMobileEmergency MedicalServices(SAMU).JPediatr(RioJ).2015;91:380---5.
∗Correspondingauthor.
E-mail:[email protected](S.W.Sarinho).
http://dx.doi.org/10.1016/j.jped.2014.10.006
PALAVRAS-CHAVE
Servic¸osde Transporte; Recém-nascido; Servic¸osMédicosde Emergência
Avaliac¸ãodaqualidadedotransporteinter-hospitalarneonatalrealizadoporum Servic¸odeAtendimentoMóveldeUrgência
Resumo
Objetivo: Verificar aqualidadedotransporteneonatalrealizadoporservic¸odeatendimento móveldeurgência(SAMU).
Métodos: Estudoobservacional transversal de antes e depois, de marc¸o aagosto de 2013. Utilizou-seinstrumentovalidadodeavaliac¸ãodotransporte,oTransportRiskIndexof Phisi-ologicStabilit(TRIPS).Foramanalisadascaracterísticasdosrecém-nascidos,intercorrênciasde aspectomédicoemecânico(dasmáquinaseambulância)eaestabilidade,antesedepoisdo transporte.Ostestesforamaplicadoscom95%deconfianc¸a.Asvariáveisnuméricasestão rep-resentadaspelasmedidasdetendênciacentralededispersão.Asvariáveiscategóricasforam avaliadaspeloTesteExatodeFisher.Nacomparac¸ãodasvariáveisentreosgruposutilizou-se oTesteT-Studentparaasdistribuic¸õesnormais,testeexatodeFisher,quandoindicado,ede Mann-Whitneyparaasnão-normais.
Resultados: 33recém-nascidosforamtransportadosdeunidadesdebaixoriscoparaunidade deterapiaintensivaneonatal.Prevaleceramogêneromasculino(57,6%)eaidadegestacional atermo (63,6%).Pesodenascimentoabaixo de2500gfoiencontrado em 39,4%dos recém-nascidos.Insuficiênciarespiratóriafoiresponsávelpor42,4%dassolicitac¸ões.Adurac¸ãomédia dotransportefoi de58minutos,semintercorrênciasmédicas oumecânicas.Oescore Trips piorouem 15%dospacientesenessegrupodeRN,amédiadatemperaturainicialde36,46
±0,19diminuiudeformasignificativapara36,08±0,22(p=0,041).
Conclusão: OtransporterealizadopeloSAMUfoiadequadoparaamaioriadosrecém-nascidos. Aoscilac¸ãodatemperaturacorporalfoiaúnicavariávelimportanteparaalterac¸ãodoescore notransporte.
©2015SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Todososdireitos reservados.
Introduction
Sincethelate1990s,studieshavestatedthatanadequately performedneonataltransferreducesmorbidityand perina-talmortality.1,2
New technologies associated with the development of Medicine andlongerlife expectancyfor newborn preterm infantshaveincreasedthedemandforprogressively special-izedservices.The regionalizationofthelatest technology is challenging, and inter-hospital transport is part of the treatmentstrategyofthesepatients.3
Studies on the subject are scarce. Only in 2011 the BrazilianSocietyofPediatrics(SociedadeBrasileirade Pedi-atria [SBP]) created a manual and organized a training course for healthcare professionals in neonataltransport, in a partnership with the Brazilian Ministry of Health (MOH).4
The stabilityof vitalsignsin thesechildren beforethe transport is a prerequisite for safe transfer. The aim of the transport is that the newborns reach their destina-tionunitwithequalorbetterstatusthanthatpriortothe transport.1,5
Therearemanyfactorsleadingtoclinicaldeterioration in newborns submittedtointer-hospital transportthat do not depend ontransport conditions.There is a consensus thatthe severitystatusbeforetransport,gestationalage, weight,anduseofvasoactivedrugs influencethestability during transport.Arecent study showedthat birth in the
absenceofatrainedprofessionalinthedelivery roomhas adirectinfluenceonthechancethattheinfantwillsurvive withgoodqualityoflife.6
Conditions associated withtransport can contribute to patientinstability:vibration,excessnoise,temperature dif-ference,distance,durationoftransporttime,andhighway conditions.However,thetransportteamshouldbeprepared tolearntorecognizeandminimizethem.7
InBrazil,theMobileEmergencyMedicalServices(Servic¸o deAtendimentoMóvelde Urgência[SAMU]) is responsible forpediatric andneonatal inter-hospitaltransport,whose conducts must follow the guidelines established by the MOHEdict2048,whichregulatestheiractivities.8TheStork
Network established the Stork SAMU program, aimed at improvingthequalityandsafetyoftransportforpregnant womenandnewborns.9
Toassessthequalityoftransport,ensuringpatientsafety withoutworseninghis/herhealthstatus,itisnecessary to useatooltopredictitseffects.Forthispurpose,the Trans-portRiskIndexofPhysiologicStability(TRIPS)wasvalidated. TheMOHconsidersTRIPStobeagoodassessmenttooland recommendsitsuse.10
observationanddatacollectionfor12hours.TheNeonatal Status Score and the Alberta Neonatal Transport Stabi-lization Score (ANTSS) have not been validated for this population,andtheHermansen’stransportscoreonlytakes into account very-low birth weight newborns, in addi-tion to requiring laboratory exams, which also makes it unpractical.11
Theaimofthisstudywastoassessthequalityofnewborn transportconductedbytheMetropolitanSAMUofthecityof Recife,stateofPernambuco,Brazil.
Methods
Thiswasacross-sectionalobservationalstudy,performedat twodifferenttimes: immediatelybeforeandafter neona-talinter-hospitaltransportconductedbytheMetropolitan SAMUofthecityofRecife,whichprovidesfull-timeservices, fromMarchtoAugustof2013.
TheTRIPSscorewasappliedaccordingtotheguidelines oftheSBP.4
TheMetropolitanSAMUofRecife,atthetimeofresearch datacollection,wasresponsiblefor22municipalities,with 32basicambulancesandeightmobileintensive careunits (ICUs).
Events that met the following inclusion criteria were selectedforthestudy:a)neonatalinter-hospitaltransport request,b) mobileICU type,sent atthe discretionofthe physician, with a destination hospital pre-defined by the hospitalbed coordinator, and c) signed informed consent byaparentorguardian.
Thestudyexclusioncriteriaincludednewbornsthatwere hemodynamicallyunstable beforetransportandrefractory tostabilizationmeasures, orthosetransportedasa result ofpre-hospitalcare(rescueservice).
Maintenance of body temperature using a transport double-wall incubator; maintenance of patent airways by endotracheal intubation, when necessary; two patent venousaccesses;andhypoglycemiaandmetabolicacidosis correction,aswellashemodynamicstabilizationmeasures wereessentialforthebeginningofthetransport.
Neonataltransportwasperformed byateamconsisting of an interventional physician, nurse, nursing technician, andambulance driver,aswell as a neonatologist, as rec-ommendedbytheSBP.4
ThemobileICU,whenconfiguredforneonataltransport, includesadouble-wallheatedincubator,neonatal mechan-icalventilator,continuousinfusionpumps,andmonitors.
The studyvariableswere:datarelatedtothenewborn (gender,gestationalage,typeofdelivery,ageat transporta-tion, birth weight, weight during transportation, primary diagnosis,andreasonfortransfer),datarelatedtothe pre-andpost-transport(hemodynamicstabilityofthenewborn, ventilatorysupport, andTRIPSscore),anddatarelatedto the analysisof medical and mechanical complications (of theequipmentandambulance)duringtransport.
Data collectionwas performed by one of the authors, usingtheelectronicdatabaseofSAMU,thepatientreferral file,andtheformcompletedbytheteamduringtransport. The SAMU transport teamwas trained tostandardize the collection of the TRIPS score, which was incorporated into the service routine. The TRIPS score provides body
temperaturemeasurement(whichwasmeasuredwitha dig-italthermometerintherightaxilla),systolicbloodpressure measurement, breathing pattern, and neurological status beforeandafterthetransport,andwasappliedinallcases. Adatabasewascreated bythe researchersanddouble dataentrywasperformed,usingthesoftwareprogram Stat-aCorp2011(StataStatisticalSoftware:Release12.College Station,TX:StataCorpLP)fortheanalysis.
Good-qualitytransportwasconsidered when theTRIPS scoreat thesecondmeasurement wasequaltoor smaller thanthescoreatthefirstmeasurement.
TheresultoftheTRIPSscorewasgroupedaccordingto the beforeand afterscore variation, as‘‘increased’’ and ‘‘maintained/decreased’’,reflectingthetransportquality. AnincreaseintheTRIPSscorereflectsthetransport-related clinicalworseningofthenewborn.
Alltests were appliedwith 95% confidence. Numerical variableswererepresentedbymeasuresofcentraltendency anddispersion.Categoricalvariableswereassessedforthe presence of associations, using Fisher’s exact test. When comparing the variables between groups, Student’s t-test was used for normal distributions, in additionto Fisher’s exacttest,whenindicated,andMann-Whitneytestfor non-normaldistributions.
TheprojectwasapprovedbytheResearchEthics Com-mittee (REC), opinion No. 200,364. The TRIPS score was appliednoninvasively,withoutpainorharmtothepatient. The study was conducted according to existing protocols withnochangeinconduct,regardlessofthepatient partic-ipationinthestudy.Incasesofpatientinstabilityorsafety threat, the transport was contraindicated, in accordance withtheSAMUcriteria.
Results
NoequipmentorambulancesproblemsoftheMetropolitan SAMUofRecifewererecorded.Thedeviceswerestableand functioningadequatelyinalltransportedcases.
A total of 42 ambulance transports of newborns were requestedattheRecifeMetropolitanSAMU.Afterexclusion criteriawere applied,33 newborns remainedin the anal-ysis, of whom57% (19/33) were malesand 78.8% (26/33) werebornbyvaginaldelivery.
Therewere14services(maternities)oforigin,including emergency units(EUs); therewere fivedestination hospi-tals,allofwhichhadhigh-complexityneonatalICU.Allbut oneofthedestinationhospitals(transportofonenewborn) wereintheBrazilianUnifiedHealthSystem(SistemaÚnico deSaúde[SUS]).
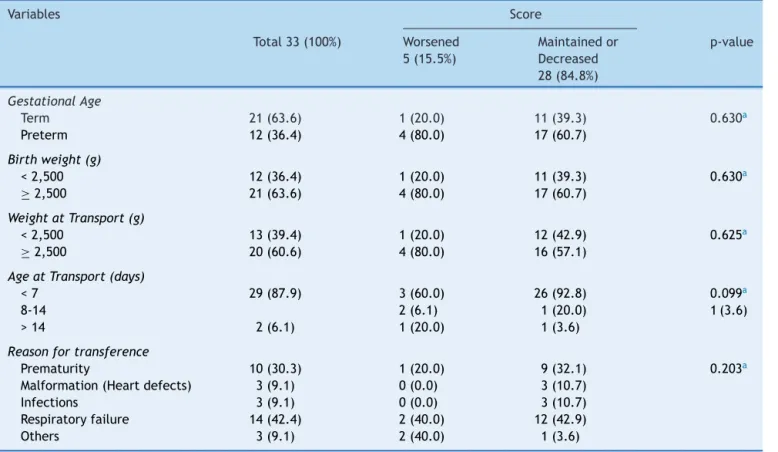
Table 1 shows that the TRIPS score was ‘‘maintained or decreased’’ in 84.80% (28/33) of cases. Most cases had gestational age between 37 and 42 weeks, age less than seven days old at the time of transport and weight during transport<2,500g (mean weight was 2,438±946.1g).Whencomparingthesedatabetween new-bornswhosescore‘‘increased’’andthosewhosescorewas ‘‘maintained/decreased’’aftertransport,variable distribu-tionwassimilarbetweenbothgroups.
Table1 Comparisonofthestudynewbornsregardingthepopulationcharacteristics.
Variables Score
Total33(100%) Worsened 5(15.5%)
Maintainedor Decreased 28(84.8%)
p-value
GestationalAge
Term 21(63.6) 1(20.0) 11(39.3) 0.630a
Preterm 12(36.4) 4(80.0) 17(60.7)
Birthweight(g)
<2,500 12(36.4) 1(20.0) 11(39.3) 0.630a
≥2,500 21(63.6) 4(80.0) 17(60.7)
WeightatTransport(g)
<2,500 13(39.4) 1(20.0) 12(42.9) 0.625a
≥2,500 20(60.6) 4(80.0) 16(57.1)
AgeatTransport(days)
<7 29(87.9) 3(60.0) 26(92.8) 0.099a
8-14 2(6.1) 1(20.0) 1(3.6)
>14 2(6.1) 1(20.0) 1(3.6)
Reasonfortransference
Prematurity 10(30.3) 1(20.0) 9(32.1) 0.203a
Malformation(Heartdefects) 3(9.1) 0(0.0) 3(10.7) Infections 3(9.1) 0(0.0) 3(10.7) Respiratoryfailure 14(42.4) 2(40.0) 12(42.9) Others 3(9.1) 2(40.0) 1(3.6)
a Fisher’sexacttest.
needforventilatorysupport,theinvasivetypewasthemost oftenused,anditwashigherthanthenumberofchildren whodidnotrequiresupport.
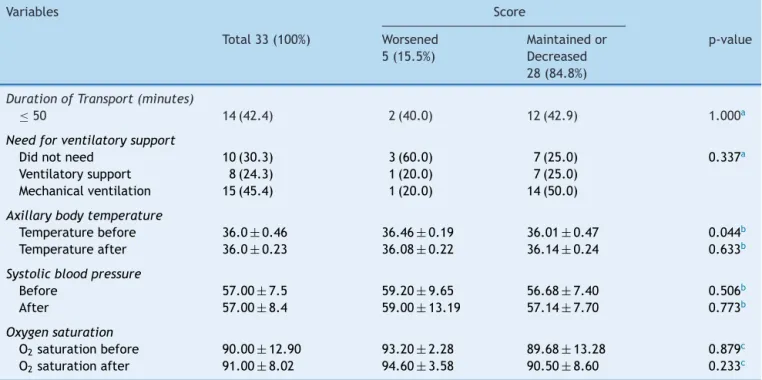
Vital signs (body temperature, oxygen saturation, and systolic blood pressure) are described in Table 2. These datawerealsocomparedbetweenthegroupsofnewborns whose score ‘‘increased’’ or ‘‘maintained/decreased’’. It wasobservedthat, inthegroup ofnewborns whose score ‘‘increased’’ after transport, the mean initial tempera-tureof36.46±0.19decreasedsignificantlyto36.08±0.22 (p=0.041),suggestingthisvariableisthemostaffectedby inter-hospital transport. This temperature alteration was observed in all five infants whoshowed worsening of the score.
Amongthenewborns,46.4%(13/28)ofthosewhosescore was‘‘maintained/decreased’’and80%(4/5)ofthosewhose score‘‘worsened’’hadscores<10beforetransport, indicat-inglowpre-transportseverity.Aftertransport,thescoresfor thegroups‘‘maintained/decreased’’and‘‘worsened’’were 50% (14/28) and 80% (4/5), respectively. However, when comparing thegroups regarding severityaccording to the TRIPSscorebefore(p=0.34)andafter(p=0.35)transport, therewasnostatisticallysignificantdifference.
Theothervariables(oxygensaturationandsystolicblood pressure)showed similarbehaviorbeforeand after trans-port, both in newborns whose score ‘‘increased’’, andin thosewhosescorewas‘‘maintained/decreased’’.
When comparing regarding the clinical deterioration variables, it was observed that only the initial tempera-ture wassignificantlydifferent;it waslowerin the group
of newborns whose score was ‘‘maintained/decreased’’ (p=0.044).
There were two deaths on the seven days imme-diately after transport among the study children: one newborn with increased TRIPS score due to congenital malformation,and anotherin the group whose score was ‘‘maintained/decreased’’, during surgery for tetralogy of Fallotcorrection.
Discussion
Onlyfiveofthetransportedinfantsshowedevidenceof clin-icaldeterioration,suggesting thatthe adequatetransport prevailed.Inspite of thesmallnumberof studysubjects, thepresent datadivergedfromsomestudiesinthe litera-turethatshowedtransportasthecauseofinstabilities.2,12---14
Inthisstudy,changeintemperaturewasthevariablethat wasalteredinthescore.
Amongthenewborns’ previousconditionsmentionedin the literature as likely to influence the quality of inter-hospital neonatal transport, the following are the most frequentlymentioned: prematurity, low birth weight,age atthe timeoftransportandhemodynamic instability.15---17
Table2 Comparisonofthestudynewbornsaccordingtothephysiologicalstatusresultduringtransport.
Variables Score
Total33(100%) Worsened 5(15.5%)
Maintainedor Decreased 28(84.8%)
p-value
DurationofTransport(minutes)
≤50 14(42.4) 2(40.0) 12(42.9) 1.000a
Needforventilatorysupport
Didnotneed 10(30.3) 3(60.0) 7(25.0) 0.337a
Ventilatorysupport 8(24.3) 1(20.0) 7(25.0) Mechanicalventilation 15(45.4) 1(20.0) 14(50.0)
Axillarybodytemperature
Temperaturebefore 36.0±0.46 36.46±0.19 36.01±0.47 0.044b
Temperatureafter 36.0±0.23 36.08±0.22 36.14±0.24 0.633b
Systolicbloodpressure
Before 57.00±7.5 59.20±9.65 56.68±7.40 0.506b
After 57.00±8.4 59.00±13.19 57.14±7.70 0.773b
Oxygensaturation
O2saturationbefore 90.00±12.90 93.20±2.28 89.68±13.28 0.879c
O2saturationafter 91.00±8.02 94.60±3.58 90.50±8.60 0.233c
Valuesexpressedasmean±standarddeviationormedian,quartilesforcontinuousvariables,andasabsolutenumbers(percentages)for categoricalvariables.
aFisher’sexacttest. b Student’st-test. c Mann-Whitneytest.
Regarding the main reasons for inter-hospital transfer, the results were similar to those reported in the litera-ture: respiratory failure as the main cause of transport request. In other words, situations requiring transfer to tertiaryunitsaretherespiratorydistresssyndromes (meco-niumaspiration,respiratorydistresssyndrome,pneumonia, andpneumothorax),pretermnewbornrequiringspecialcare (gestationalage<32weeks and/or birth weight<1,500g), severehypoxia,suspectedheart disease,seizures, perina-tal infections (sepsis), and surgical situations/congenital malformations.19
The transport occurred within distances of less than 50km, whichwas reflectedin the transporttime.It is of utmostimportancetounderstandthatpatientstabilization isanessentialrequirementforadequatetransport, regard-lessoftransporttimeordistance.20Thetransportteammust
confirm patient stabilitybefore starting the transport, so thatitsbenefitsoutweightheinherentrisks.1
Forthetransporttobesuccessful,withminimalrisks,the patientmustbewell-monitoredpatient,undergoingassisted mechanicalventilation,ifnecessary,afterreceiving medica-tionsatthelocalhospitalbeforetranspor.4Thetransportof
critically-illnewbornsisaprocesswithahighdegreeofrisk andcomplexity,asthesepatientstendtobeunstable.5The
internalenvironmentoftheambulancehindersinvasive pro-cedures:orotrachealintubationshouldbeperformedbefore thetransport,whenevernecessary.4
SBPhascreatedacoursetotrainhealthcareprofessionals inneonataltransport,aspartoftheNeonatalResuscitation Program,identifyingthetenstepsforsuccessfultransport; seven of them refer to the pre-transport. The sixth step
recommendsthecalculationoftheriskofpatientmortality, usingthe TRIPS score.Although thereareother scores to assessphysiologicalstability,whichtakeintoaccountother parametersofvitalsigns,suchasheartrate,meanarterial pressure,Apgarscoreatbirth,useofvasoactivedrugs, res-piratoryrate,bloodglucose,whitebloodcellcountbefore and after transport, among other factors,11,15,21 SBP uses
theTRIPSscoretosupporttheirrecommendations.Thiswas thebasisforthescoreselectionforthepresentstudy,used toassesstherealityofthetransportperformedbySAMU.
Themeasurementof vitalsignsbeforeandafter trans-port, regardless of the score calculation, is a routine practiceintransportservices,whichmeasures heartrate, oxygensaturation,axillarytemperature,andsystolicblood pressure.Thelattertwonotonlycontributetothe calcula-tionoftheTRIPSscore,butarealsoincludedinthetransport medicalfileandinformedatthedestinationhospital. Axil-lary temperature is one of the variables that change the mostduringtransport,asshowninstudiesthatuseditasa transportassessmentparameter.12,20,22
Iftheteamsweretrainedspecificallyinneonatal trans-port,theresultswouldprobablybeevenbetter.Theauthors suggest an integration between SAMU, MOH, and SBP in order tosystematically train healthcare staff in neonatal transport,reassessingneonataltransportserviceteamsand exchanging previous experience on patient transport and careofthetransportednewborn.
Conflicts
of
interest
Acknowledgments
To the Mobile Emergency Medical Services of the city of
Recife, and to Dr. José Henrique Moura and Dr. Sônia
Bechara,fortheirsupportandassistanceontheproject.
References
1.AbecasisF.Transporteneonatalepediátrico-organizac¸ãoe per-spectivasactuais.NascereCrescer.2008;173:162---5.
2.AlbuquerqueAM,LeiteAJ,AlmeidaNM,SilvaCF.Avaliac¸ãoda conformidadedotransporteneonatalparahospitalde referên-ciadoCeará.RevBrasSaudeMaternInfant.2012;12:55---64. 3.CusackJ,FieldD,ManktelowB.Impactofservicechangeson
neonataltransferpatternsover10years.ArchDisChildFetal Neonatal.2007;92:F181---4.
4.MarbaST,Guinsburg R,Almeida MFB,NaderPJH,VieiraALP, RamosJRM,etal.Transportederecém-nascidodealtorisco: diretrizes da Sociedade Brasileira de Pediatria. 1st ed. São
Paulo:SociedadeBrasileiradePediatria;2011.
5.RatnavelN.Safetyandgovernanceissuesforneonataltransport services.EarlyHumDev.2009;85:483---6.
6.Araújo BF, Zatti H, Oliveira Filho PF, Coelho MB, Olmi FB, GuaresiTB,etal.Effectofplaceofbirthandtransporton mor-bidityandmortalityofpretermnewborns. JPediatr (RioJ). 2011;87:257---62.
7.BouchutJC,VanLE,ChritinV,GueugniaudPY.Physicalstressors duringneonatal transport:helicopter compared withground ambulance.AirMedicalJournal.2010;30:134---9.
8.Brasil.Ministério da Saúde. Secretaria de Atenc¸ão à Saúde. Coordenac¸ãoGeraldeUrgênciaseEmergências.PortariaGM/MS n.o2048,de5denovembrode2002.Brasil;2002p.37---228. (SérieE.Legislac¸ãodeSaúde).
9.Brasil.Ministério da Saúde. Secretaria de Atenc¸ão à Saúde. Portaria 650-Rede Cegonha. Brasil 2011 p. 1---33. [Cited 2012 Jul 9]. Available from: http://onlinelibrary.wiley. com/doi/10.1002/cbdv.200490137/abstract
10.LeeSK,ZupancicJA,PendrayM,ThiessenP,SchmidtB,Whyte R,etal.Transport riskindexofphysiologicstability:a prac-tical system for assessing infant transport care. J Pediatr. 2001;139:220---6.
11.MargottoP.Escoredeavaliac¸ãodaseveridadededoenc¸a neona-tal.JPerinatol.2002;22:26---30.
12.daMotaSilveiraSM,Gonc¸alvesdeMello MJ,de ArrudaVidal S,deFriasPG,CattaneoA.Hypothermiaonadmission:arisk factorfordeathinnewbornsreferredtothePernambuco Insti-tute of Mother and Child Health. J Trop Pediatr. 2003;49: 115---20.
13.HarrisonC,McKechnieL. Howcomfortableisneonatal trans-port.ActaPaediatr.2011;101:1---5.
14.GoldsmitG,RabasaC,RodríguezS,AguirreY,ValdésM,Pretz D,etal.Riskfactorsassociatedtoclinicaldeterioration dur-ingthetransportofsicknewborninfants.ArchArgentPediatr. 2012;110:304---9.
15.BroughtonSJ,BerryA,JacobeS,CheesemanP,Tarnow-Mordi WO,GreenoughA.Themortalityindexforneonatal transporta-tion score: a new mortality prediction model for retrieved neonates.Pediatrics.2004;114:e424---8.
16.Spector JM, Villanueva HS, Brito ME, Sosa PG. Improving outcomes of transported newborn in Panama: Impact of a nationwideneonatalprovidereducationprogram.JPerinatol. 2009;29:512---6.
17.SoaresE,MenezesG.Fatoresassociadosàmortalidade neona-talprecoce:análisedesituac¸ãononívellocal.EpidemiolServ Saúde.2010;19:51---60.
18.Arora P,BajajM,Natarajan G, AroraNP, KalraVK,Zidan M, etal.Impactofinter-hospitaltransportonthephysiologic sta-tusofverylow-birth-weightinfants.AmJPerinatol.2014;31: 237---44.
19.Mendes C, Bettencourt A, Onofre J. Transporte do recém-nascido para UCIN terciária. Consensos em neonatologia. 2004; p. 25---8. [cited2012 Mar 21]. Available from: http:// www.lusoneonatologia.com/admin/ficheirosprojectos/ 201107201731-transporternparaucin.pdf
20.Kumar PP, Kumar CD, Shaik FR, Ghanta SB, Venkatalakshmi A. Prolonged neonatal interhospital transport on road: rele-vance for developing countries. Indian J Pediatr. 2010;77: 151---4.
21.Mathur NB, Arora D. Role of TOPS (a simplified assessment ofneonatalacutephysiology)inpredictingmortalityin trans-portedneonates.ActaPaediatr.2007;96:172---5.