REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
SCIENTIFIC
ARTICLE
Randomized,
controlled
trial
comparing
the
effects
of
anesthesia
with
propofol,
isoflurane,
desflurane
and
sevoflurane
on
pain
after
laparoscopic
cholecystectomy
Jaime
Ortiz
a,∗,
Lee
C.
Chang
a,
Daniel
A.
Tolpin
a,
Charles
G.
Minard
b,
Bradford
G.
Scott
c,
Jose
M.
Rivers
aaDepartmentofAnesthesiology,BaylorCollegeofMedicine,Houston,TX,UnitedStates
bDanL.DuncanInstituteforClinicalandTranslationalResearch,BaylorCollegeofMedicine,Houston,TX,UnitedStates cMichaelE.DeBakeyDepartmentofSurgery,BaylorCollegeofMedicine,Houston,TX,UnitedStates
Received11December2012;accepted20March2013
Availableonline11October2013
KEYWORDS
Laparoscopic cholecystectomy; Pain;
Propofol; Inhalational anesthetics
Abstract
Background: Painistheprimarycomplaintandthemainreasonforprolongedrecoveryafter laparoscopiccholecystectomy.Theauthorshypothesizedthatpatientsundergoinglaparoscopic cholecystectomy willhavelesspainfourhoursaftersurgerywhenreceivingmaintenance of anesthesiawithpropofolwhencomparedtoisoflurane,desflurane,orsevoflurane.
Methods:Inthisprospective,randomizedtrial,80patientsscheduledforlaparoscopic cholecys-tectomywereassignedtopropofol,isoflurane,desflurane,orsevofluraneforthemaintenance ofanesthesia.Ourprimaryoutcomewaspainmeasuredonthenumericanalogscalefourhours aftersurgery.Wealsorecordedintraoperativeuseofopioidsaswellasanalgesicconsumption duringthefirst24haftersurgery.
Results:Therewasnostatisticallysignificantdifferenceinpainscoresfourhoursaftersurgery (p=0.72).Therewerealsonostatisticallysignificantdifferencesinpainscoresbetween treat-mentgroupsduringthe24haftersurgery(p=0.45).Intraoperativeuseoffentanylandmorphine didnotvarysignificantlyamongthegroups(p=0.21and0.24,respectively).Therewereno dif-ferencesintotalmorphineandhydrocodone/APAPuseduringthefirst24h(p=0.61and0.53, respectively).
Conclusion: Patientsreceivingmaintenanceofgeneralanesthesiawithpropofoldonothave less pain after laparoscopic cholecystectomy when compared to isoflurane, desflurane, or sevoflurane.
© 2013SociedadeBrasileirade Anestesiologia.Publishedby ElsevierEditoraLtda.Allrights reserved.
∗Correspondingauthor.
E-mail:[email protected](J.Ortiz).
Introduction
Pain is the primary complaint and the main reason for
prolonged recovery after laparoscopic cholecystectomy.1
0104-0014/$–seefrontmatter©2013SociedadeBrasileiradeAnestesiologia.PublishedbyElsevierEditoraLtda.Allrightsreserved.
Previous studies investigating postoperative pain after
laparoscopic cholecystectomy reported large amounts of
inter-individual variation.2 Pain after laparoscopic
chole-cystectomyhasthreecomponents:incisionalpain,visceral
pain,andreferredshoulderpain.2Overthepast 20years,
severalstudieshaveexaminedthisissueusingamultimodal
approachtopostoperativepainmanagementafter
laparo-scopiccholecystectomy.3---8
The inhalational anesthetics isoflurane, desfluraneand
sevoflurane are commonly used to provide maintenance
of general anesthesia during surgery. Certain inhalational
agents reportedly increase sensitivity to pain at lower
concentrations as present during emergence, but relieve
painathigher concentrations.9 The differentialeffectsof
inhalationalagentsonnociceptivepathwaysmayinfluence
postoperativepaindevelopment.Specifically,investigators
haveshownthatisofluranehyperalgesiamaybemodulated
bythenicotinicreceptor.10
Clinical studies examining propofol versus inhalational
agents for the maintenance of general anesthesia reveal
potentialbenefitstopropofoladministrationwhichinclude:
improvementsinwell-being,decreasedpostoperativepain
scores, and decreased incidence of postoperative nausea
andvomiting(PONV).11---14However,notallofthesestudies
weredesignedorpoweredtolookspecificallyat
postopera-tivepain.AstudybyFassoulaki15didnotshowanydifference
inpostoperativepainscoresafterabdominalhysterectomy
ormyomectomywhencomparingpropofol,desflurane,and
sevofluraneformaintenanceofanesthesia.Theconflicting
findings withregard tothe potential analgesic benefit of
propofoluse for maintenanceof anesthesiahave resulted
ina numberof varyingopinions withintheanesthesiology
literature.16---18
Toourknowledge,nostudyinvestigatingdifferencesin
postoperativepainfollowinglaparoscopiccholecystectomy
has been reported in the literature comparing
mainte-nanceof anesthesiawithpropofol,isoflurane, desflurane,
or sevoflurane.The authors feltit would beimportant to
comparepropofoltoallthreeofthecommonlyused
inhala-tionalagents in this study,asdifferent results have been
found when comparing propofol to each of the separate
agents.11---15 Ourhypothesis wasthatmaintenanceof
anes-thesiawithpropofolwillresultinlesspainfourhoursafter
laparoscopiccholecystectomywhencomparedtoisoflurane,
desflurane,orsevoflurane.
Patients,
materials
and
methods
Patientrecruitment
Thestudy protocolwasapprovedbytheBaylorCollegeof
Medicine IRB in August2009 and registered at
ClinicalTri-als.gov(NCT00983918,September2009).Informed,written
consentwasobtainedfrom80inpatientsbetweentheages
of18and64classifiedasAmericanSocietyof
Anesthesiolo-gists(ASA)physicalstatusI,II,orIII,scheduledtoundergo
laparoscopic cholecystectomyat Ben TaubGeneral
Hospi-talinHouston,Texas.Patientswereexcludedifanyofthe
followingapplied:scheduledforoutpatientsurgery,
sched-uledforopencholecystectomy,renaldysfunction(Cr>1.2),
allergytoanyofthestudymedications,chronicopioiduseat
home,orinabilitytoproperlydescribepostoperativepainto
investigators (e.g.,languagebarrier, neuropsychiatric
dis-order). Patientswere enrolledbystudyinvestigatorsfrom
September 23, 2009 to June 10, 2010. Study recruitment
was placedon hold fromDecember 23, 2009 toMarch 9,
2010duetoalocalshortageofpropofol.
Randomization
Patients were assigned to one of four study groups using
acomputerrandomizationscheme generatedbya
depart-ment administrator usingthe website Randomization.com
(http://www.randomization.com). Patients had an equal
25%chanceofassignmenttoanyofthegroups.Group
assign-mentswere placed inside numberedopaque envelopesas
follows:GroupP---maintenanceofanesthesiawithpropofol
infusion; GroupI---maintenanceof anesthesiawith
isoflu-rane;GroupD---maintenanceofanesthesiawithdesflurane;
andGroupS---maintenanceofanesthesiawithsevoflurane.
Upon enrollment, all subjects were familiarized with the
numerical analog scale (NAS) and the postoperative pain
routine.Itwasexplainedthatascoreof‘‘0’’represented
no painand a score of ‘‘10’’ represented the worst pain
imaginable. Patients, surgeons and nurses assessing pain
scores were blindedwith regardtogroup assignment and
anestheticagent.Themembersoftheanesthesiateam
per-formingthegeneralanestheticwerenotblinded.
Anesthetictechnique
After placement of a peripheral venous catheter, a
lac-tated ringer’s infusion was started. A preoperative pain
score at rest was recorded at this time. Standard
moni-toringandBispectral index(BIS)(AspectMedicalSystems,
Norwood,MA)monitoringwereappliedforallgroups.
Mida-zolam1---2mgIVwasgivenfor anxiolysisasneeded.After
pre-oxygenationwith100%oxygen,anesthesiawasinduced
with fentanyl 2mcg/kg, lidocaine 1mg/kg, and propofol
2.5mg/kg. Tracheal intubationwasfacilitatedwitheither
succinylcholine1---2mg/kgorrocuronium0.6mg/kg.
Maintenance of anesthesia was provided as follows:
Group P--- propofolinfusion, Group I --- isoflurane, Group
D---desflurane,andGroupS ---sevoflurane.Theamount of
anestheticforallgroupswastitratedtomaintainaBISvalue
between30and50duringtheprocedure.Musclerelaxation
wasmaintainedwithrocuronium.Additionaladministration
of fentanyl50---100mcgwasgivenat thediscretionof the
anesthesiateamduringtheprocedure.Allpatientsreceived
ondansetron4mgIVandketorolac30mgIVafterremovalof
the gallbladder.Neuromuscular blockade wasantagonized
withneostigmineandglycopyrrolateattheendofsurgery.
The anesthesia team was instructed to give morphine as
needed at theend of theprocedure toassistwith
emer-gence.
Allpatientsreceived astandard laparoscopic
cholecys-tectomy withpneumoperitoneumpressures maintainedat
15mmHgthroughout.Atotalof10mLofbupivacaine0.25%
was injected subcutaneously at the trocar insertion sites
afterwound closureby thesurgical teamasfollows:3mL
foreachofthe10mmtrocarincisions,and2mLforeachof
Postoperativecareandpainassessment
Time of arrival to the post-anesthesia care unit (PACU)
became Time 0 for our pain assessments. Pain at rest
was recorded for each patient using the NAS (0---10) at
Time0, and at 1, 2, 4, 8, 12, and24h after the surgery
was completed. All patients were placed on a
postop-erative analgesic regimen which included hydrocodone
5mg/acetaminophen500mgtablets,2tabletsgivenformild
pain(NAS3---5)every6hwithamaximumof6tabletsina
24hperiod,andmorphine4mgIV,givenevery3hforsevere
pain(NAS6---10).PainscoreswererecordedbythePACUand
floornurses takingcare ofthe patientwithoutknowledge
ofpatientgroupassignment.Inaddition,analgesicuseand
PONVeventsduringthefirst24hwererecorded.
Statistics
Theprimaryoutcomewaspostoperativepainscoresonthe
NAS from0to10 four hoursaftersurgery. The secondary
outcomewaspainscoresduringthefirst24haftersurgery.
A study by Gupta19 reported that pain after laparoscopic
cholecystectomy had a standard deviation of ±2 on the
visualanalogscale.Assumingacommonstandarddeviation
of2.5unitssinceweusedanumericalanalogscale,atotalof
18patientspergroupwouldberequiredtodetecta3unit
differencebetween two groups with80% power assuming
alpha=0.01.Analpha=0.01levelwasassumedtomaintain
anoverallTypeIerrorrateof0.05formultiplecomparisons.
Toaccountforanypatientdropoutsormissingpatientdata,
weplannedtoenroll20patientsperstudygroupforatotal
of80patients.
Patientdemographics,surgerycharacteristics,analgesic
use, and pain scores were compared across treatment
groups. A one-way ANOVA model was used to compare
meanpostoperativepainscoresatfourhoursaftersurgery
acrosstreatmentgroups aswellascontinuouslymeasured
baselineandsurgicalcovariates.Categoricalvariableswere
comparedusing Fisher’s exact test. The overall effect of
treatment groups during the first 24h after surgery was
compared using a general linear mixed model assuming
an unstructured covariance matrix of correlated errors.
The model included fixed effects for treatment group,
Assessed for eligibility (n=97)
Randomized (n=80)
Sevoflurane (n=20) Isoflurane (n=20) Propofol (n=20) Desflurane (n=20)
Lost to follow-up (n=0) Lost to follow-up (n=0)
Lost to follow-up (n=0) Lost to follow-up (n=0)
Analysed (n=18)
®Excluded from analysis– open cholecystectomy (n=2)
Analysed (n=18)
®Excluded from analysis– open cholecystectomy (n=2)
Analysed (n=18)
®Excluded from analysis– open cholecystectomy (n=2)
Analysed (n=20)
®Excluded from analysis– open cholecystectomy (n=0) Excluded (n=17)
®Not meeting inclusion criteria (n=8) ®Declined to participate (n=9)
Table1 Patientdemographicsandsurgicalcharacteristics.
PROP ISO DES SEVO
(n=18) (n=18) (n=20) (n=18)
Age 29(7) 34(12) 33(12) 34(14)
Weight(kg) 76(22) 80(16) 77(27) 74(16)
Height(in.) 62(2) 63(3) 63(3) 63(4)
Female 18(100) 16(89) 14(70) 15(83)
ASAclass
1 10(55) 5(28) 5(25) 7(39)
2 7(39) 13(72) 14(70) 10(55)
3 1(6) 0(0) 1(5) 1(6)
Diagnosis
AC 11(61) 10(55) 12(60) 9(50)
BC 4(22) 5(28) 3(15) 8(44)
GP 3(17) 3(17) 5(25) 1(6)
Surgerytime(min) 93(16) 102(45) 88(23) 86(28)
Anesthesiatime(min) 148(19) 155(47) 142(24) 142(33)
Estimatedbloodloss(mL) 39(25) 47(54) 42(34) 37(28)
Nausea
No 15(83) 13(72) 16(80) 16(89)
Yes 3(17) 5(28) 4(20) 2(11)
Continuousvariablesarepresentedasmean(SD)andcategoricalvariablesarepresentedasn(%).
time,andgroup---timeinteractionterm.Treatmentandtime were modeled as categorical variables. The model was alsoadjusted forcovariatesincludingage,weight,height, sex,ASAclassification,diagnosis,intraoperativemorphine, intraoperativefentanyl,surgerytime,anesthesiatime,and estimated blood loss.Statistical significance wasassessed at˛=0.05.AllanalyseswereperformedusingSAS9.2(SAS
InstituteInc.,Cary,NC).
Results
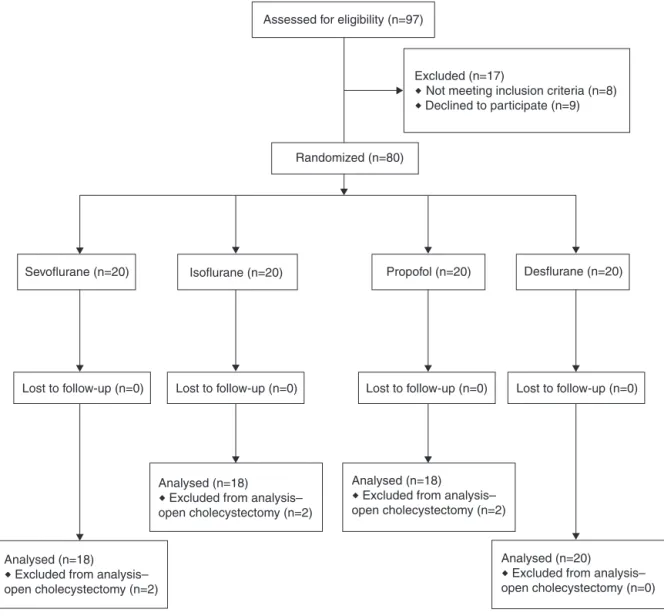
TheCONSORTpatientflowdiagramisshowninFig.1.Atotal
of80patientswereprospectivelyenrolledinthestudy.Six
patientsweresubsequentlyexcludedfromthefinalanalyses
because they met one of the exclusion criteria
(conver-sion of laparoscopic to open procedure). The remaining
74patientsincludedin thefinalanalysesweredistributed
as follows: 20 patients in the desflurane group, and 18
patientseach in the propofol,isoflurane, andsevoflurane
groups.
Ouroverallpatientpopulationwas85%female.The
pop-ulation was 85% Latin American, 6.25% Caucasian, 6.25%
AfricanAmerican, and 2.5%Asian.The preoperative
diag-nosesweredistributedasfollows:acutecholecystitisin56%,
biliarycolicin28%,andgallstonepancreatitisin16%ofthe
patients.
A summary of demographicand surgical data is shown
inTable1. Table2summarizes theanalgesic consumption
data. We did not find a statistically significant
differ-ence in the intraoperative use of fentanyl and morphine
betweenthegroups(p=0.21and0.24,respectively).
Addi-tionally,therewere nodifferences in total morphineand
hydrocodone/APAP use during the first 24h (p=0.61 and
0.53,respectively).
Fig.2showspainscoresforthefirst24hforallgroups.
There was no statistically significant difference in pain
scores four hours after surgery (p=0.72). Differences in
painscores between treatment groups did notdepend on
time(p=0.43),andtheinteractiontermwasremovedfrom
the model. There were no statistically significant
differ-ences inpainscores betweentreatment groups (p=0.45).
Timewassignificantlyassociatedwithpainscore(p<0.001).
Evenafteradjustingforpreoperativepainscores,treatment
groupswerenotstatisticallydifferent(p=0.42).Patientage
wassignificantlyassociatedwithpainscore(p<0.001).On
average,painscoresdecreasedby0.7unitsforevery10-year
increaseinage.Otherwise,noothercovariateswere
signifi-cantlyassociatedwithpostoperativepainscores(p>=0.16).
The largest differences between mean pain scores
occurredonehourafterarrivaltoPACU.Allpairwise
com-parisons were tested for significant differences using an
independent,two-samplet-test.Afteradjustingfor
multi-ple comparisonsusing theBonferroni correction, only the
differencebetweenpropofolanddesfluranewasstatistically
significant(p=0.04).Allothercomparisonswerenot
signif-icant (p>=0.07) assuming an overall Type1 error rate of
0.05.
Discussion
Theresultsofthisstudydonotsupportthehypothesisthat
patientsreceivingmaintenanceofanesthesiawithpropofol
havelesspainfourhoursafterlaparoscopiccholecystectomy
whencomparedtoisoflurane,desflurane,orsevoflurane.
Our findings differ from recent studies that reported
lowerpainscoresaftersurgeryinpatientsanesthetizedwith
propofolwhencomparedtoisofluraneorsevoflurane.11,12A
Table2 Analgesiccomparison.
PROP ISO DES SEVO p
(n=18) (n=18) (n=20) (n=18)
Preoppainscore(0---10) 1.3(2.4) 0.4(1.1) 1.7(2.1) 1.1(2.1) 0.28
Intraopfentanyl
>250mcg 6(33) 11(61) 8(40) 5(28)
<250mcg 12(67) 7(39) 12(60) 13(72) 0.21
Intraopmorphine(mg) 6.1(4.3) 5.1(4.1) 3.6(4.0) 6.1(4.8) 0.24
24hmorphine(mg) 16(8) 15(11) 12(7) 13(8) 0.61
Hydrocodone/APAP(#) 1.9(1.8) 1.9(2.1) 2.2(1.6) 1.3(1.8) 0.53
Continuousvariablesarepresentedasmean(SD)andcategoricalvariablesarepresentedasn(%).p-valuesobtainedbycomparingsummary measuresacrosstreatmentgroupsusingone-wayANOVAfor continuouslymeasuredvariablesandFisher’sexacttestfor categorical variables.
P 10
8
6
4
2
0
I D S P I D S P I D S P I D
Anesthetic type
hour = 0 hour = 1 hour = 2 hour = 4 hour = 8 hour = 12 hour = 24
P
ain score
S P I D S P I D S P I D S
Figure2 Meanpainscoresandstandarderrorsbytimeandanesthetictype.
whencomparedtoisoflurane,butonlytwopainscoreswere recordedafterthefirsthour,at2and24haftersurgery.The study by Tan12 showed patients hadless pain with
propo-folwhencomparedtosevoflurane,butonlylookedatpain
scoresduringthefirstfourhoursaftersurgery.Incontrast,
our study showed no significant difference in pain scores
forthesevofluraneandpropofolgroupsthroughoutthe24h
postoperativeperiod.
Advocatesofutilizingpropofolformaintenanceof
anes-thesia often refer to studies linking inhaled anesthetics
and pain on the biochemical level. For example, Zhang9
and Flood10 both reported on the hyperalgesic qualities
of isoflurane. Recently, isoflurane and desflurane were
found toactivatetransient receptorpotential(TRP)-A1in
aconcentration-dependentmanner.20 TRP-A1ispresent in
peripheralnociceptors.Thissameeffectwasnotobserved
withhalothaneorsevoflurane,suggestingthatactivationof
TRP-A1mayplayaroleinthedevelopmentofhyperalgesia
bythe irritant volatileanesthetics.20 Although patients in
ourstudythatwereanesthetizedwithdesfluranewerefound
tohavemorepainonehouraftersurgerywhencomparedto
propofol,thisdifferencewasnot found tobestatistically
significantatanyoftheothermeasuredtimepointsduring
thefirst24h.
Althoughwewereunabletoshowthatpropofolhas
anal-gesicbenefits when compared tothe inhalational agents,
ourstudyhaslimitations.Thisstudywaspoweredbasedon
analgesicconsumptionoverthefirst24h.Althoughwefound
no statistically significant differences in the use of
fen-tanyl,morphine,orhydrocodone/APAPinourstudygroups,
thismayneed furtherinvestigationusingastudypowered
forthatspecificoutcome.Someofthestatisticalmethods
usedtoanalyzethedatamakenormalityassumptions,but
the NAS is inherently non-normal. However,
nonparamet-ric analysis usingKruskal---Wallis and Kolmogorov---Smirnov
testsyieldednearlyidenticalresults.Theonlynotable
dif-ferencewasthattheBonferroniadjustedp-valuecomparing
propofolanddesfluraneonehouraftersurgerywasnolonger
significant(p=0.12).
Inaddition,wemodeledourprotocolbasedonthe
com-mon postoperative pain management of patients at our
institution,whichincludesamultimodalapproachwithlocal
anesthetics, NSAIDS and opioids. These analgesic agents
affect postoperativepain andcouldmask anydifferences
betweenpropofolandtheinhalationalagents.For
compari-sonpurposes,patientsreceivedpostoperativePCAmorphine
inthestudy byCheng11 whichshowedthat patients
anes-thetizedwithpropofolhadlesspaincomparedtoisoflurane
afteropen uterinesurgery.Patientsundergoingdiagnostic
laparoscopicgynecologicalsurgeryinthestudybyTan12had
lesspainafterpropofolwhencomparedtosevoflurane,but
received paracetamol, diclofenac, dexamethasone,
mor-phineandoxycodoneaspartoftheirmultimodalregimen.
Wechose tousepropofolastheIVinduction agentfor
all groups in this study since this is common practice at
ourinstitution.Althoughitcanbearguedthataninhalation
inductionwould bethe beststudydesign for thepatients
receivingmaintenance of anesthesiawithisoflurane,
des-flurane,orsevoflurane,theriskofaspirationinthispatient
population and difficulties with inhalation inductions in
adultpatientsmadethisimpractical.Therefore,wecannot
disregard any potential effects onpain that an induction
doseofpropofolcouldhaveonallgroups.
Anotherpotentialconfounderisthatsomeofourpatients
received succinylcholine at the anesthesiologist’s
discre-tion.Wefeltitwasimportanttoallowthischoiceasmany
patientsinourstudy populationhaveriskfactorsfor
aspi-rationor difficultventilation andintubation,and assuch,
theuse of succinylcholinemay be preferredover
rocuro-niumforinduction andintubation.Itispossiblethatsome
ofourpatientsmayhavehadpostfasciculationmusclepain
caused by succinylcholine which could have affected our
postoperativepainassessments.
Manypreviousclinicalstudiesonpainafterlaparoscopic
cholecystectomycommonlyhaveapatientpopulationwith
aprimarydiagnosisofbiliarycolicandsurgeryisusually
per-formedintheoutpatientsetting.Amajorityofpatientsin
ourstudy wereundergoingoperation foracute
cholecysti-tis.This subgroup of patients mayhave more painduring
theperioperativeperiodwhencomparedtopatientswitha
primarydiagnosis ofbiliarycolicor gallstonepancreatitis.
Thisincreasedperioperativepaininourpatientpopulation
couldmask anypotentialdifferencebetween the
mainte-nanceagents.However,thisheterogeneouspopulationisa
commonpatientmixatmanycommunityhospitals.
In conclusion, maintenance of general anesthesia with
propofol did not lead to decreased pain scores four
hours after laparoscopic cholecystectomy when
com-pared to isoflurane, desflurane, or sevoflurane. Further,
well-designed studies are needed to ascertain whether
propofol has any beneficial effect on postoperative pain
whencomparedtotheinhalationalagentsafterother
sur-gicalproceduresinthesettingofmultimodalanalgesia.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
WearegratefultoDr.RobertM.BryanJr.,Professorof
Anes-thesiologyatBaylorCollegeofMedicine,forassistinguswith
dataanalysis.Thisstudywassupported,inpart,bytheDan
L.DuncanInstituteforClinicalandTranslationalResearch.
References
1.BisgaardT,KlarskovB,RosenbergJ,etal.Factorsdetermining convalescenceafteruncomplicatedlaparoscopic cholecystec-tomy.ArchSurg.2001;136:917---21.
2.BisgaardT,KlarskovB,RosenbergJ,etal.Characteristicsand prediction ofearly pain afterlaparoscopic cholecystectomy. Pain.2001;90:261---9.
3.BisgaardT.Analgesictreatmentafterlaparoscopic cholecystec-tomy: acritical assessmentof theevidence. Anesthesiology. 2006;104:835---46.
4.JensenK,KehletH,KundCM.Post-operativerecoveryprofile after laparoscopic cholecystectomy: a prospective, obser-vational study of a multimodal anaesthetic regimen. Acta AnaesthesiolScand.2007;51:464---71.
5.MichaloliakouC,ChungF,SharmaS.Preoperativemultimodal analgesia facilitates recovery after ambulatory laparoscopic cholecystectomy.AnesthAnalg.1996;82:44---51.
6.MunozHR,GuerreroME,BrandesV,etal.Effectoftimingof morphineadministrationduringremifentanil-basedanaesthesia onearlyrecoveryfromanaesthesiaandpostoperativepain.Br JAnaesth.2002;88:814---8.
7.SinhaS,MunikrishnanV,MontgomeryJ, etal.Theimpactof patient-controlledanalgesiaonlaparoscopiccholecystectomy. AnnRCollSurgEngl.2007;89:374---8.
8.ZajaczkowskaR,WnekW,WordliczekJ,etal.Peripheral opi-oidanalgesiainlaparoscopiccholecystectomy.RegAnesthPain Med.2004;29:424---9.
9.Zhang Y, Eger 2nd EI, Dutton R, et al. Inhaled anesthetics havehyperalgesiceffectsat0.1minimumalveolaranesthetic concentration.AnesthAnalg.2000;91:462---6.
10.Flood P, Sonner JM, Gong D, et al. Isoflurane hyper-algesia is modulated by nicotinic inhibition. Anesthesiology. 2002;97:192---8.
11.ChengSS,YehJ, FloodP.Anesthesiamatters:patients anes-thetizedwithpropofolhavelesspostoperativepainthanthose anesthetizedwithisoflurane.AnesthAnalg.2008;106:264---9.
12.TanT, BhinderR, Carey M,etal. Day-surgerypatients anes-thetizedwithpropofolhavelesspostoperativepainthanthose anesthetizedwithsevoflurane.AnesthAnalg.2010;111:83---5.
13.HoferCK,ZollingerA,BüchiS,etal.Patientwell-beingafter general anaesthesia: a prospective, randomized, controlled multi-centretrialcomparingintravenousandinhalation anaes-thesia.BrJAnaesth.2003;91:631---7.
15.FassoulakiA,MelemeniA,ParaskevaA,etal.Postoperativepain andanalgesicrequirementsafteranesthesiawithsevoflurane, desfluraneorpropofol.AnesthAnalg.2008;107:1715---9.
16.ShaferSL,NekhendzyV.Anesthesiamatters:statisticalanomaly ornewparadigm?AnesthAnalg.2008;106:3---4.
17.FloodP.Pro:accumulatingevidenceforanoutrageousclaim. AnesthAnalg.2010;111:86---7.
18.WhitePF.Con:anesthesiaversusanalgesia:assessingthe anal-gesiceffectsofanestheticdrugs.AnesthAnalg.2010;111:88---9.
19.GuptaA,ThörnSE,AxelssonK,etal.Postoperativepainrelief using intermittent injections of 0.5% ropivacaine through a catheter after laparoscopic cholecystectomy. Anesth Analg. 2002;95:450---6.