REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
Official Publication of the Brazilian Society of Anesthesiologywww.sba.com.br
SCIENTIFIC
ARTICLE
Opioid-free
total
intravenous
anesthesia
with
propofol,
dexmedetomidine
and
lidocaine
infusions
for
laparoscopic
cholecystectomy:
a
prospective,
randomized,
double-blinded
study
夽
Mefkur
Bakan
a,∗,
Tarik
Umutoglu
a,
Ufuk
Topuz
a,
Harun
Uysal
a,
Mehmet
Bayram
b,
Huseyin
Kadioglu
c,
Ziya
Salihoglu
aaDepartmentofAnesthesiologyandReanimation,BezmialemVakifUniversityFacultyofMedicine,Istanbul,Turkey bDepartmentofPulmonaryMedicine,BezmialemVakifUniversityFacultyofMedicine,Istanbul,Turkey
cDepartmentofGeneralSurgery,BezmialemVakifUniversityFacultyofMedicine,Istanbul,Turkey
Received8February2014;accepted5May2014 Availableonline3June2014
KEYWORDS
Laparoscopic cholecystectomy; Totalintravenous anesthesia; Dexmedetomidine; Lidocaine;
Propofol; Remifentanil
Abstract
Backgroundandobjectives: Intraoperativeuseofopioidsmaybeassociatedwithpostoperative
hyperalgesia andincreasedanalgesic consumption.Sideeffectsduetoperioperativeuse of opioids, such as postoperative nausea andvomiting may delaydischarge. We hypothesized thattotal intravenousanesthesia consistingoflidocaineanddexmedetomidineasanopioid substitute maybe analternativetechniquefor laparoscopiccholecystectomy andwouldbe associatedwithlowerfentanylrequirementsinthepostoperativeperiodandlessincidenceof postoperativenauseaandvomiting.
Methods:80AnesthesiologistsI---IIadultswerescheduledforelectivelaparoscopic
cholecystec-tomy.Patientswererandomlyallocatedintotwogroupstohaveeitheropioid-freeanesthesia withdexmedetomidine,lidocaine,andpropofolinfusions(GroupDL)oropioid-basedanesthesia withremifentanil,andpropofolinfusions(GroupRF).Allpatientsreceivedastandard multi-modalanalgesiaregimen.ApatientcontrolledanalgesiadevicewassettodeliverIVfentanyl for6haftersurgery.Theprimaryoutcomevariablewaspostoperativefentanylconsumption.
Results:Fentanylconsumptionatpostoperative2ndhourwasstatisticallysignificantlylessin
GroupDL,comparedwithGroupRF,whichwere75±59gand120±94grespectively,while
itwascomparableatpostoperative6thhour.Duringanesthesia,thereweremorehypotensive eventsinGroupRF,whilethereweremorehypertensiveeventsinGroupDL,whichwereboth statisticallysignificant.Despitehigherrecoverytimes,GroupDLhadsignificantlylowerpain scores,rescueanalgesicandondansetronneed.
夽 Trialregistration:Clinicaltrials.gov(ID:NCT01833819). ∗Correspondingauthor.
E-mail:[email protected](M.Bakan).
http://dx.doi.org/10.1016/j.bjane.2014.05.001
Conclusion:Opioid-free anesthesiawith dexmedetomidine, lidocaineandpropofol infusions maybeanalternativetechniqueforlaparoscopiccholecystectomyespeciallyinpatientswith highriskforpostoperativenauseaandvomiting.
©2014SociedadeBrasileiradeAnestesiologia.PublishedbyElsevier EditoraLtda.Allrights reserved.
PALAVRAS-CHAVE
Colecistectomia laparoscópica; Anestesiavenosa total;
Dexmedetomidina; Lidocaína;
Propofol; Remifentanil
Anestesiavenosatotallivredeopioides,cominfusõesdepropofol,dexmedetomidina elidocaínaparacolecistectomialaparoscópica:estudoprospectivo,randomizadoe duplo-cego
Resumo
Justificativaeobjetivos: Ousode opioidesnoperíodo intraoperatóriopodeestarassociado
àhiperalgesiae ao aumentodo consumo deanalgésicos no períodopós-operatório. Efeitos colateraiscomo náuseaevômitonoperíodopós-operatório,porcausadousoperioperatório deopioides,podemprolongaraalta.Nossahipótesefoiqueaanestesiavenosatotal como usodelidocaínaedexmedetomidinaemsubstituic¸ãoaopioidespodeserumatécnicaopcional paraacolecistectomialaparoscópicaeestariaassociadaaumamenorsolicitac¸ãodefentanile incidênciadenáuseaevômitonoperíodopós-operatório.
Métodos: Foramprogramadosparacolecistectomialaparoscópicaeletiva80pacientesadultos,
estadofísicoASAI-II.Ospacientesforamrandomicamentealocadosemdoisgrupospara rece-beranestesialivredeopioidescominfusõesintravenosas(IV)dedexmedetomidina,lidocaínae propofol(GrupoDL)ouanestesiabaseadaemopioidescominfusõesderemifentanilepropofol (GrupoRF).Todosospacientesreceberamumregimepadrãodeanalgesiamultimodal.Um dis-positivodeanalgesiacontroladapelopacientefoiajustadoparaliberarfentanilIVporseishoras apósacirurgia.Odesfechoprimáriofoioconsumodefentanilnopós-operatório.
Resultados: Oconsumodefentanilnasegundahoradepós-operatóriofoisignificativamente
menornogrupoDLdoquenoGrupoRF,75±59ge120±94g,respectivamente,masfoi
com-parávelnasextahoradepós-operatório.Duranteaanestesia,houvemaiseventoshipotensivos noGrupoRFemaiseventoshipertensivosnogrupoDL,ambosestatisticamentesignificativos. Apesar de apresentar um tempo de recuperac¸ão mais prolongado, o Grupo DL apresentou escoresdedoreconsumodeanalgésicosderesgateedeondansetronasignificativamentemais baixos.
Conclusão:Aanestesialivredeopioidescominfusõesdedexmedetomidina,lidocaínae
propo-fol podeseruma técnicaopcionalpara acolecistectomialaparoscópica, especialmente em pacientescomaltoriscodenáuseaevômitonopós-operatório.
©2014SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
Opioidsarewidely usedfor perioperativeanalgesia. How-ever, the intraoperative use of large bolus doses or continuous infusions of potent opioidsmay be associated with postoperative hyperalgesia and increased analgesic consumption.1Whenitcomestoambulatorysurgery,opioid relatedsideeffects,suchaspostoperativenauseaand vomi-ting(PONV),prolongedsedation,ileusandurinaryretention maydelay recovery and discharge or cause unanticipated hospitalreadmission.
The postoperative painafter laparoscopic cholecystec-tomy (LC) is complex in nature and growing evidence suggeststhat itstreatment shouldbemultimodaland opi-oidsparingtoacceleraterecovery.2,3Inspiteofmultimodal analgesic strategies, which consist of opioids, dexameth-asone, non-steroidal anti-inflammatory drugs, and local anestheticsappliedintothesurgicalwound,postoperative
painandPONVarestillcommoncomplaintsreportedafter LC.Ithasbeen suggestedthatesmololinfusionmaybean acceptable alternative toremifentanil infusion for ambu-latory laparoscopic surgery4---6 and opioid-free anesthetic techniqueswithesmololinfusionisassociatedwithreduced postoperativeopioidconsumption.5,6
returnofbowelfunction anddecreasedlength ofhospital stay.14---20Therefore,wehypothesizethattotalintravenous anesthesia (TIVA) consisting of lidocaine combined with dexmedetomidineasanopioidsubstituteisafeasible tech-nique forLCandwould beassociatedwithlowerfentanyl requirementsintheearlypostoperativeperiodandless inci-denceofPONV.
The present prospective, randomized, double-blinded study was designed to compare the effect of opioid-free (using dexmedetomidine, lidocaine and propofol infusions)andopioid-based(usingremifentanilandpropofol infusions)TIVA techniques onpostoperative painintensity and the incidence of side effects in patients scheduled forLC.
Methods
After obtaining the Ethics Committee’s approval and the patients’ written informed consent, the study was conductedbetweenJune2012andApril2013atour univer-sity hospital.Patients scheduled for elective laparoscopic cholecystectomy,whohadtheAmericanSocietyof Anesthe-siologists(ASA)IorIIphysicalstatus,andwere20---60years of age were included in this study.The exclusion criteria were: a body mass index >35kgm−2, pregnant, breast-feedingor menstruatingwomen,hepatic,renalor cardiac insufficiency, diabetes, history of chronic pain,alcohol or drug abuse, psychiatric disease, allergy or contraindica-tion to any of the study drugs, inability to comprehend painassessment andtouse apatient-controlled analgesia
(PCA)device.Writteninformedconsentwasobtainedfrom patientsbeforerandomization.
Randomizationandblinding
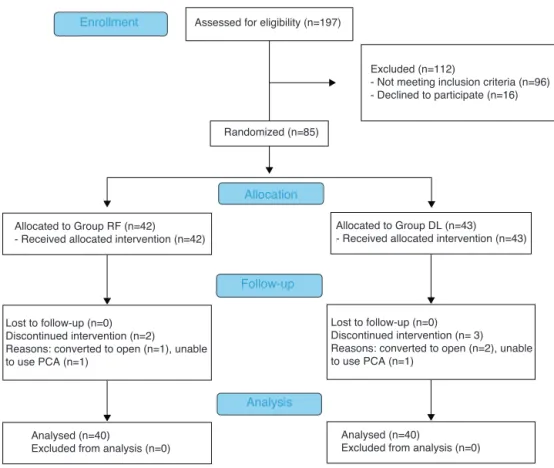
Patientswererandomly allocatedintotwogroups tohave eitheropioid-freeanesthesia(GroupDL)with dexmedetomi-dine(0.6gkg−1loading,0.3gkg−1h−1infusion),lidocaine (1.5mgkg−1 loading, 2mgkg−1h−1 infusion), and propofol infusionsor opioid-based anesthesia(Group RF)with fen-tanyl, and remifentanil(0.25gkg−1min−1),and propofol infusions(Fig.1).
Simplerandomizationwasdoneusing80opaquesealed envelopes,40for eachgroup,indicatinggroupassignment anddescribing the anestheticprotocol. Before anesthesia induction,ananesthesiologistopenedthenextenvelopein thesequencetorevealthetreatmentallocation.This anes-thesiologistonly prepared thestudy medications and was notinvolvedinpreoperativeandpostoperativedata collec-tionoranesthesiamanagementofthepatients.
TimechartofanestheticmanagementisshowninTable1. The drugs were delivered in 10mL and 50mL syringes labeledas‘‘loading’’or‘‘infusion’’respectively.Toensure properblinding,theloadingdosesofdrugs (dexmedetomi-dineandlidocaineinGroupDLorfentanylandnormalsaline in Group RF) were calculated according to the patient’s body weight and diluted to a 10mL volume labeled as ‘‘loading-1’’ and ‘‘loading-2’’ in order of administration. Theinfusiondrugs(dexmedetomidineandlidocaineinGroup DL or remifentanil and normal saline in Group RF) were
Assessed for eligibility (n=197)
Excluded (n=112)
- Not meeting inclusion criteria (n=96) - Declined to participate (n=16)
Analysed (n=40)
Excluded from analysis (n=0) Lost to follow-up (n=0)
Discontinued intervention (n=2) Reasons: converted to open (n=1), unable to use PCA (n=1)
Allocated to Group RF (n=42)
- Received allocated intervention (n=42)
Lost to follow-up (n=0) Discontinued intervention (n= 3) Reasons: converted to open (n=2), unable to use PCA (n=1)
Allocated to Group DL (n=43) - Received allocated intervention (n=43)
Analysed (n=40)
Excluded from analysis (n=0) Allocation
Analysis Follow-up Randomized (n=85) Enrollment
Table1 Timechartofanestheticmanagement.
Premedication Loading(10min) Induction Maintenance
A↓ B↓ C↓ D↓
GroupDL
Midazolam (0.03mgkg−1)
Loading1: Dexmedetomidine (0.6gkg−1)
Infusion1: Dexmedetomidine (0.3gkg−1h−1)
(0.3mLkg−1) Loading2: Lidocaine (1.5mgkg−1)
Infusion2:Lidocaine(2mgkg−1h−1)(0.1mLkg−1)
Propofol (1.5mgkg−1)
Propofol(3---12mgkg−1h−1)
GroupRF
Midazolam (0.03mgkg−1)
Loading1: Fentanyl (2gkg−1)
Infusion1:Remifentanil(0.25gkg−1min−1)(0.3mLkg−1) Loading2:0.9%
Saline
Infusion2:0.9%Salineinfusion(0.1mLkg−1)
Propofol (1.5mgkg−1)
Propofol(3---12mgkg−1h−1)
A,Baselinehemodynamicvaluesrecorded;B,Endotrachealintubation;C,‘Infusion2’wasstoppedaftergallbladderextraction;D,End ofsurgery,propofolinfusionand‘Infusion1’wasstopped.
preparedin50mLsyringesandlabeledas‘‘infusion-1’’and ‘‘infusion-2’’respectively.
Anesthetictechnique
Atthepreoperativeholdingarea,patientswereinstructed ontheuseofthenumericalratingscale(NRS)andpatient controlledanalgesia(PCA) pump. An anesthesiologist who is blinded to the study groups performed all procedures. On arrival at the operating room, standard monitoring was applied consisting of ECG, non-invasive blood pres-sure, pulse oximetry, temperature, and bispectral index (BIS). After premedication with intravenous midazolam 0.03mgkg−1, baselineheart rateand meanarterial blood
pressure (MAP) were determined which is the average of three consecutive measurements. Intravenous bal-anced crystalloid solution (Isolyte-S) was started and pre-oxygenation with 5Lmin−1 of pure oxygen was
per-formed during administration of loading doses. Before induction, patients in Group DL received 0.6gkg−1
dexmedetomidine (loading-1) diluted to a total volume of10mL andinfused in10min. To avoid bias,patients in GroupRFreceivedfentanyl2gkg−1inthesamefashion.At
theinduction, dexmedetomidine or remifentanilinfusions (in 1gmL−1 and 50gmL−1 concentrations respectively,
labeledasinfusion-1)at0.3mLkg−1h−1werestarted.
Lido-caineat1.5mgkg−1(loading-2)inGroupDLornormalsaline
inGroupRFandpropofolat1.5mgkg−1wasadministered.
Lidocaine(20mg/mL)ornormalsalineinfusions(infusion-2) at 0.1mLkg−1h−1 and propofol infusion at 10mgkg−1h−1
wasstarted immediately after loading doses. Vecuronium at0.1mgkg−1IVwasgiventofacilitatetrachealintubation.
Thedoseofdexmedetomidinewasbasedonaliterature21 that compared dexmedetomidine-based versus fentanyl-based TIVA and found no difference in extubation and
discharge times. The dose of remifentanil was based on studies,achievingsufficientanalgesiaforLC.22,23
DexmedetomidineandlidocaineinfusionsinGroupDLor remifentanilandnormalsalineinfusionsinGroup RFkeep constantduringsurgery.Propofolinfusionratewasadjusted to3---12mgkg−1h−1 tomaintainthemeanarterialpressure (MAP)within±20%ofthebaselinevalue,andtomaintaina BISreadingbelow50.Thelidocaineornormalsaline admin-istration was terminated after gallbladder extraction or aproximately10minbeforetheendofsurgery.Skinincisions wereinfiltratedwith15---20mLofbupivacaine0.5% includ-ing1/80.000 adrenalinebeforeclosure. Dexmedetomidine or remifentanil and propofol infusions were terminated during skin closure. Residualneuromuscular blockadewas antagonized with neostigmine 0.05mgkg−1 and atropine 0.02mgkg−1andtrachealextubationwasperformed when patientsachievedaregularspontaneousbreathingpattern. Thelungsweremechanicallyventilatedwithamixture of oxygen in air (FiO2: 50%, tidal volume 7---10mLkg−1, respiratory rate 10---14min−1) to obtain an end-tidal car-bon dioxide (EtCO2) value between 30 and 35mmHg. Supplemental neuromuscular blockade wasachieved with vecuronium after assessment of neuromuscular function withtrain-of-four.Intraoperative normothermiawas main-tainedwithforcedairwarmingblanketspositionedoverthe exposed partsof thebodyand IVcrystalloidwas adminis-tered at a rate of 6---12mLkg−1h−1 during anesthesia. All patients wore anti-embolicstockings and received enoxa-parin40mgsubcutaneouslybeforesurgery;dexamethasone 8mganddexketoprophentrometamol50mgIVafter anes-thesia induction; andparacetamol1g IVaftergallbladder extraction.
IV dose of 0.1mg nitroglycerine was administered when MAP>120mmHg.
Surgery
Surgeons whowere experiencedin laparoscopic cholecys-tectomyperformedtheoperationsusingstandard 4-trocar technique. After endotracheal intubation a nasogastric tube wasinserted and stomach content wasaspirated. A blunt-tipped 12-mm trocar was used toaccess the perit-onealcavity.Pneumoperitoneumwasachievedwithcarbon dioxide, and intra-abdominal pressure was maintained at 12---14mmHg throughout surgery. Three additional 5-mm portswere introducedand patientswere positionedin 30 degreesanti-Trendelenburgpositionandrotatedtowardthe leftsidetofacilitateexposureofthegallbladder.Attheend ofsurgery,patientswerereturnedtosupinepositionandthe inflatedcarbondioxidewascarefullyevacuatedbymanual compressionoftheabdomen.
Postoperativecare
A PCA pump wasready touse immediately after extuba-tionfor 6h. The PCA pump wassettodeliver fentanylIV withabolusdoseof20g,alockoutof5min,without con-tinuous infusion and dose limit. Transition from PACU to surgicalwardwasconsidered tobesafewhen thepatient had achieved a Modified Aldrete Score ≥9. Although LC is established as a day-case procedure, our protocol was designedtoadmitallpatientsfor24htoensureadequate follow-upofpatientsandforproperdatacollection.Patients wereallowedtodrinkwater4hafterextubation. Postopera-tivenauseaandvomitingwastreatedwithmetoclopramide 10mgIV(with 8h oftimeinterval)andifnoteffectivein 15min ondansetron 4mg IV was administered. After PCA wasstopped allpatients received oral doses of paraceta-mol500mg(4×1)anddexketoprophentrometamol25mg (3×1)andtramadol100mgasarescueanalgesic. Investi-gatorsblindedtotreatment allocationand withnoaccess totheintraoperativerecordsperformedalloutcome assess-mentsinthepost-anesthesiacareunit(PACU)andsurgical ward.Painscoreswereassessedusingthe11-pointNRS(0 corresponding tono painand 10 to the worst imaginable pain).
Thefollowingdatawerecollected:demographic charac-teristicsofthepatientsstudied,historyofsmoking,motion sickness and PONV, duration of surgery and anesthesia, amount of drugs used during surgery, amount of fentanyl usedinpostoperativeperiodfor6h,NRS,incidenceofPONV andotheradverseevents.
Statisticalanalysis
The primary outcome variable was fentanyl consumption used for pain relief in the first 6h after extubation. Secondary outcome measures were recovery times, the incidence of PONV, and maximal overall NRS pain score (max-NRS) at the surgical ward after PCA was discontin-ued.Thesamplesizerequirementwasbasedonpreliminary datafromapreviouspilotstudywithtenpatientsinwhich
fentanylrequirements were200±152gin Group RFand 120±88ginGroupDL.Thus,atanalphariskof0.05,39 patientspergroupwouldprovide 80%poweranddetect a 40%reductioninfentanylconsumptioninatreatmentgroup. Theresultsarepresentedasmediansandquartiles. Descrip-tivevariablesaregivenaspercentages.TheMann---Whitney
U test was used to compare the continuous parameters. Fisher’s exact test was used to compare non-parametric variables.Allstatisticalanalyseswereperformedusingthe commerciallyavailableSPSSv.16.0softwarepackage(SPSS Inc.,Chicago,IL,USA).Aprobabilityvalueoflessthan0.05 wasconsideredstatisticallysignificant.
Results
Ofthe197patientapproached,66didnotmeetthecriteria forinclusion,14refusedtoparticipateinthestudy,4turned toopensurgery,leaving80patientssuitabletobeenrolled inthisinvestigation(Fig.1).
Thepatients’characteristicsandperioperativedataare detailed in Table 2. Patient characteristics were not sig-nificantly different among groups. Propofol consumption, orientation and PACU discharge times were significantly higherinGroupDL.
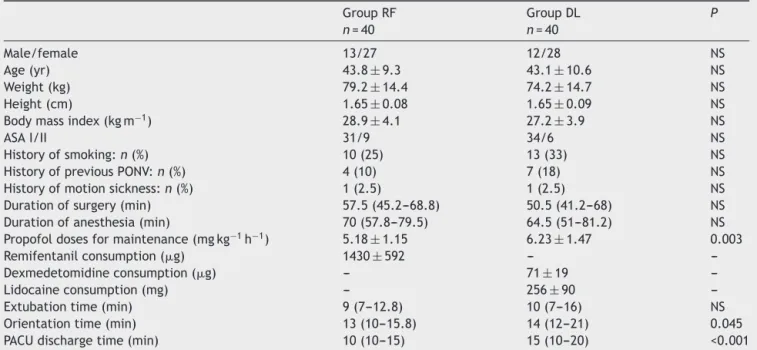
Baselinevaluesofheartrateandmeanarterialpressure werecomparablebetweenthegroups.Heartrateandmean arterialpressurevaluesafterinduction, at intubationand 1st,4th,7thand10thminofpneumoperitoneumwere signifi-cantlyhigherinGroupDL(Fig.2).Thereweremorepatients requiringephedrinetotreathypotensioninGroup RF,and more patients requiring nitroglycerine to treat hyperten-sioninGroupDL.NitroglycerineuseinGroupDL(n=11)was mostlyat thebeginningof thepneumoperitoneum(n=9). Othersideeffectswerecomparableamonggroups,except ondansetron use(Table 3).None ofthe patients in Group DLrequire ondansetron to treat PONV (p<0.05). None of thepatientsinbothgroupsreportedrecallofintraoperative eventsandcomplainedaboutanysideeffectsthatmaybe relatedtolidocaine(cardiacarrhythmia,perioralnumbness, metaltaste,tinnitusandvisualdisturbances).
Threepatients inGroup RFand6 patientsinGroup DL withminimalpainpreferrednottousePCA(0>0.05). Post-operative fentanyl consumption 2h after extubation and max-NRSandrescueanalgesicneedaftercessationof fen-tanyl PCA was significantly lower in Group DL (Table 4). Cumulativepostoperative fentanyl consumption 4 and 6h afterextubationwerecomparableamonggroups(Fig.3).
Discussion
Table2 DemographicCharacteristicsandPerioperativeData.
GroupRF
n=40
GroupDL
n=40
P
Male/female 13/27 12/28 NS
Age(yr) 43.8±9.3 43.1±10.6 NS
Weight(kg) 79.2±14.4 74.2±14.7 NS
Height(cm) 1.65±0.08 1.65±0.09 NS
Bodymassindex(kgm−1) 28.9±4.1 27.2±3.9 NS
ASAI/II 31/9 34/6 NS
Historyofsmoking:n(%) 10(25) 13(33) NS
HistoryofpreviousPONV:n(%) 4(10) 7(18) NS
Historyofmotionsickness:n(%) 1(2.5) 1(2.5) NS
Durationofsurgery(min) 57.5(45.2---68.8) 50.5(41.2---68) NS
Durationofanesthesia(min) 70(57.8---79.5) 64.5(51---81.2) NS
Propofoldosesformaintenance(mgkg−1h−1) 5.18±1.15 6.23±1.47 0.003
Remifentanilconsumption(g) 1430±592 ---
---Dexmedetomidineconsumption(g) --- 71±19
---Lidocaineconsumption(mg) --- 256±90
---Extubationtime(min) 9(7---12.8) 10(7---16) NS
Orientationtime(min) 13(10---15.8) 14(12---21) 0.045
PACUdischargetime(min) 10(10---15) 15(10---20) <0.001
Dataare presentedasrelative numberofpatients,mean±standarddeviation,median(25th---75th percentile),orabsolutenumber (percentage).
NS,notsignificant;ASA,AmericanSocietyofAnesthesiologists;PONV,postoperativenauseaandvomiting;PACU,post-anesthesiacare unit.
hyperalgesiaseemstobemorereasonableforthisfinding. Cumulativefentanyl consumption becomescomparable at 4thand6thhourspostoperatively.Thismightbeduetothe treatmentofpostoperativepainwithanotherpotentopioid (fentanyl)thatmightcausehyperalgesiaand/ortolerance. Ifwecouldmakethepostoperativepaintreatment opioid-free,theanalgesicconsumptioninGroupDLmightcontinue tobe significantlylowerat 4thand6thhpostoperatively. Thus,themax-NRSscoresandrescueanalgesic needafter cessationof fentanylPCA wassignificantly lowerinGroup DL.
Potent opioids are usually have to be used to con-trol the intraoperative cardiovascular instability due to pneumoperitoneum in LC.24 It has been reported that in patientsundergoingLC,intraoperativeinfusionoflidocaine,
80
77 76
67 76
73 72 71 72
66* 66* 65* 63* 64* 62*
Group RF Group DL
70
60
50
0 BI AI P1 P4 P7 P10
Heart rate (HR)
Figure2 Changesinheartratebetweengroupsduring intra-operative periods. 0: baseline values, BI: before intubation (afterinduction),AI:afterintubation,P1:1stminuteof pneu-moperitoneum,P4:4thminuteofpneumoperitoneum,P7:7th minuteofpneumoperitoneum,P10:10thminuteof pneumoperi-toneum.*:p<0.05betweengroups
in combination with low doses of opioids was associ-atedwithreducedintraoperativeandpostoperativeopioid requirements.18,19 Park et al.25 reported that pain scores after LC were reduced in the early postoperative period by the addition of dexmedetomidine in the multimodal analgesic regimen. Dexmedetomidine has mild analgesic properties than opioidshave; it hasbeen usedasan opi-oidsubstituteinvarioussurgicalinterventions21,26---28andis foundtobeassociatedwithlesspostoperativepain21,27and PONV21,27,28 but slowrecovery.26,27 Also,dexmedetomidine use(withsomefentanylsupport)asaremifentanilsubstitute in TIVA duringgynecologic video-laparoscopic surgerywas foundtobeeffective.29 But,laparoscopiccholecystectomy isuniquecomparedwithotherlaparoscopicproceduresand
120
96 94
67 72
80 81 81 83
Group RF Group DL
110
100
90
80
70
60 0 BI AI P1 P4 P7 P10
Mean arterial pressure (MAP)
94* 91* 100*
108* 98*
85*
Table3 Incidenceofeventsandsideeffects.
GroupRF
n=40
GroupDL
n=40
Pvalue
Ephedrineuse 8(20) 1(3) 0.029
Nitroglycerineuse 0 11(28) <0.001
Intraoperativebradycardia 4(10) 0 NS
Intraoperativetachycardia 0 1(3) NS
Sub-hepaticdrainuse 6(15) 5(13) NS
Shivering 10(25) 3(8) NS
Nausea 13(33) 5(13) NS
Vomiting 5(13) 1(3) NS
Ondansetronuse 6(15) 0 0.026
Valuesarepresentedasnumberofpatients(percentage). NS,notsignificant.
associated with higher sympathoadrenal response, so we wanttoincreasetheanalgesiceffectsofdexmedetomidine andlidocainebycombiningtheseagents.
It has been demonstrated that dexmedetomidine enhancesthelocalanesthetic actionof lidocaineinpigs30 and improves the quality of anesthesia and periopera-tive analgesia when added to lidocaine for IV regional anesthesia.31 Dexmedetomidine use, combined with lido-caine and propofol was defined for tracheal intubation without the use of muscle relaxants and intubation con-ditions were found to be statistically more satisfactory compared with fentanyl.32 But, the combined analgesic effect of dexmedetomidine and lidocaine in total intra-venous general anesthesia was not evaluated before our study.
Previousstudies inpatients undergoingLC showedthat intraoperativeesmololinfusioninsteadofopioidsis associ-atedwithreducedpostoperativeopioidrequirements.5,6In asimilarstudywithours,Collardetal.5comparedfentanyl, remifentanilandesmololadjunct todesfluraneanesthesia forLCandpatientsinesmololgroupused100g(median) fentanyl in the postoperative period (2h), which seems comparablewithouropioid-basedgroup.Inourstudy,we usedpropofol infusion insteadof desfluraneandthat was foundtobeassociatedwithlesspostoperativeanalgesic con-sumption during remifentanil-based anesthesia.22,33 Also, propofol has anti-emetic properties. Propofol use instead
of inhalational anesthetics in LC seems more suitable in this opioid-free concept. But, it has been suggested that dexmedetomidine may delay recovery, as an adjuvant to propofol during TIVA.34 This is consistent with our study, while the orientation and PACU discharge time was sig-nificantly higher in Group DL. This may be due to the higherinfusionrateofpropofoltocontrolthehemodynamic responsetopneumoperitoneum.
Thedouble-blindfashionofthestudymaybealimitation; astheinfusionratesofdexmedetomidineandremifentanil wereconstant,nitroglycerineor ephedrinehadtobeused tocontrolthehemodynamicfluctuationsinsomepatients. As 28% of patients in Group DL were hypertensive at the beginningof the pneumoperitoneumand regardinghigher nitroglycerineuse inGroup DL, theprotocol can be mod-ified with additionof small amount of opioid or a higher infusion rate for dexmedetomidine (1gkg−1 loading and 0.2---0.5gkg−1h−1maintenance)whichmightbemore appro-priate.Itmaybereasonabletopreferdelayedrecoveryto postoperativeincreasedpainintensity andPONVfor some patients.Also,desfluraneuseinsteadofpropofol(maximum dosewaslimitedto12mgkg−1h−1)inGroupDLmight alle-viate hypertensive events and beassociated with shorter recovery.
Postoperative pain after LC is highly variable among patients. There is need for individualized anesthesia technique and postoperative analgesic treatment. As
Table4 Postoperativepainintensityanalysis.
GroupRF
n=40
GroupDL
n=40
p
Postoperativefentanylconsumption
0---2h(g) 120±94(110) 75±59(60) 0.04
0---4h(g) 185±143(160) 123±100(120) NS
0---6h(g) 235±175(220) 162±142(150) NS
Max-NRS 4(2---6) 3(2---4) 0.028
Max-NRS-cough 5.5(3---7) 4(3---5) 0.015
Shoulderpain(n) 7(18%) 10(25%) NS
Rescueanalgesicneed(n) 19(48%) 9(23%) 0.034
dexmedetomidine and lidocaine decreases the anesthetic andopioidconsumption,itisreasonabletoaddtheseagents inananesthesiaregimenforLC.Formeropioidaddictionor high-risk for PONV maybe reasons for preference of this opioid-freetechnique.
In conclusion: when compared with opioid-based TIVA withremifentaniland propofolinfusions, opioid-freeTIVA withdexmedetomidine,lidocaineandpropofolinfusionsis associated withlower fentanyl requirements in the early postoperativeperiod(0---2h).Also, max-NRS,rescue anal-gesic need and ondansetron use was significantly lower in the opioid-free group in the first postoperative day. Despite prolonged recovery times, opioid-free anesthesia withdexmedetomidine, lidocaineandpropofol maybean alternativetechniqueforLCinselectedpatientsespecially withhighriskofPONV.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.AngstMS,ClarkJD.Opioidinducedhyperalgesia:aqualitative systematicreview.Anesthesiology.2006;104:570---87.
2.BisgaardT,KlarskovB,RosenbergJ,etal.Characteristicsand prediction of earlypain after laparoscopic cholecystectomy. Pain.2001;90:261---9.
3.BisgaardT.Analgesictreatmentafterlaparoscopic cholecystec-tomy: a criticalassessment oftheevidence. Anesthesiology. 2006;104:835---46.
4.ColomaM,ChiuJW,WhitePF,etal.Theuseofesmololasan alternative toremifentanil duringdesflurane anaesthesiafor fast-trackoutpatientgynecologiclaparoscopicsurgery.Anesth Analg.2001;92:352---7.
5.CollardV,MistralettiG, TaqiA,etal. Intraoperativeesmolol infusionintheabsenceofopioidssparespostoperativefentanyl in patientsundergoing ambulatorylaparoscopic cholecystec-tomy.AnesthAnalg.2007;105:1255---62.
6.Lopez-AlvarezS,Mayo-MoldesM,ZaballosM,etal.Esmolol ver-susketamine-remifentanilcombinationforearlypostoperative analgesia after laparoscopic cholecystectomy: a randomized controlledtrial.CanJAnaesth.2012;59:442---8.
7.Arain SR, Ruehlow RM, Uhrich TD, et al. The efficacy of dexmedetomidineversusmorphineforpostoperativeanalgesia aftermajorinpatientsurgery.AnesthAnalg.2004;98:153---8. 8.Gurbet A, Basagan-Mogol E, Turker G, et al. Intraoperative
infusionofdexmedetomidinereducesperioperativeanalgesic requirements.CanJAnaesth.2006;53:646---52.
9.TufanogullariB,WhitePF,PeixotoMP,etal.Dexmedetomidine infusion during laparoscopic bariatric surgery: the effecton recoveryoutcomevariables.AnesthAnalg.2008;106:1741---8. 10.Unlugenc H, Gunduz M, Guler T, et al. The effect of
pre-anestheticadministrationofintravenousdexmedetomidineon postoperativepaininpatientsreceivingpatientcontrolled mor-phine.EurJAnaesthesiol.2005;22:386---91.
11.OhtaniN, YasuiY, WatanabeD,et al. Perioperativeinfusion of dexmedetomidine at a high dose reduces postoperative analgesicrequirements:arandomizedcontroltrial.JAnesth. 2011;25:872---8.
12.Blaudsun G, Lysakowski C, Elia N, et al. Effect of periop-erative systemic alfa-2 agonists on postoperative morphine consumption and pain intensity: systematic review and meta-analysisofrandomizedcontrolledtrials.Anesthesiology. 2012;116:1312---22.
13.CortinezLI,HsuYW,Sum-PingST,etal.Dexmedetomidine phar-macodynamics:PartII:Crossovercomparisonoftheanalgesic effectofdexmedetomidineandremifentanilinhealthy volun-teers.Anesthesiology.2004;101:1077---83.
14.Groudine SB, Fisher HA, Kaufman Jr RP, et al. Intravenous lidocaine speeds the return of bowel function, decreases postoperative pain, and shortens hospital stay in patients undergoing radical retropubic prostatectomy. Anesth Analg. 1998;86:235---9.
15.KoppertW,WeigandM,NeumannF,etal.Perioperative intra-venouslidocainehaspreventiveeffectsonpostoperativepain and morphine consumption after major abdominal surgery. AnesthAnalg.2004;98:1050---5.
16.Wu CT, Borel CO, Lee MS, et al. The interaction effect of perioperativecotreatmentwithdextromethorphanand intra-venouslidocaineonpainreliefandrecoveryofbowelfunction afterlaparoscopic cholecystectomy.Anesth Analg.2005;100: 448---53.
17.Kaba A, Laurent SR, Detroz BJ, et al. Intravenous lido-caineinfusionfacilitatesacuterehabilitationafterlaparoscopic colectomy.Anesthesiology.2007;106:11---8.
18.LauwickS,KimdoJ,MichelagnoliG,etal.Intraoperative infu-sionoflidocainereducespostoperativefentanylrequirements in patients undergoing laparoscopic cholecystectomy. Can J Anaesth.2008;55:754---60.
19.Saadawy IM, Kaki AM, Abd El Latif AA, et al. Lidocaine vs. magnesium:effectonanalgesiaafteralaparoscopic cholecys-tectomy.ActaAnaesthesiolScand.2010;54:549---56.
20.Vigneault L, Turgeon AF, CotéD, et al. Perioperative intra-venous lidocaine infusion for postoperative pain control: a meta-analysisofrandomizedcontrolledtrials.CanJAnaesth. 2011;58:22---37.
21.TurgutN,TurkmenA,GokkayaS,etal.Dexmedetomidine-based versusfentanyl-basedtotalintravenousanaesthesiaforlumbar laminectomy.MinervaAnesthesiol.2008;74:469---74.
22.GrundmannU,SilomonM,BachF,etal.Recoveryprofileand sideeffectsofremifentanil-basedanaesthesiawithdesflurane orpropofolforlaparoscopiccholecystectomy.ActaAnaesthesiol Scand.2001;45:320---6.
23.VanDeldenPG,HouwelingPL,BenciniAF,etal. Remifentanil-sevoflurane anaesthesia for laparoscopic cholecystectomy: comparison of three dose regimens. Anesthesia. 2002;57: 212---7.
24.Mann C, Boccara G, Pouzeratte Y, et al. The relation-ship among carbondioxide pneumoperitoneum, vasopressin release and hemodynamic changes. Anesth Analg. 1999;89: 278---83.
25.Park JK, Cheong SH, Lee KM, et al. Does dexmedetomidine reduce postoperative pain after laparoscopic cholecystec-tomy with multimodal analgesia? Korean J Anesthesiol. 2012;63:436---40.
26.Turgut N, TurkmenA, Ali A, et al. Remifentanil-propofol vs dexmedetomidine-propofol.Anesthesiaforsupratentorial cran-iotomy.MJEAnesth.2009;20:63---70.
27.SalmanN,UzunS,CoskunF,etal.Dexmedetomidineasa sub-stituteforremifentanilinambulatorygynecologiclaparoscopic surgery.SaudiMedJ.2009;30:77---81.
28.Ali AR, Ghoneimy MN. Dexmedetomidine versus fentanyl as adjuvanttopropofol:comparativestudyinchildren undergo-ing extracorporeal shock wave lithotripsy. Eur Anaesthesiol. 2010;27:1058---64.
29.BulowNM,BarbosaNV,RochaJB.Opioidconsumptionintotal intravenousanaesthesiaisreducedwithdexmedetomidine:a comparativestudy with remifentanil in gynecologic videola-paroscopicsurgery.JClinAnesth.2007;19:280---5.
31.MemisD,TuranA,KaramanliogluB,etal.Adding dexmedetomi-dinetolidocaineforintravenousregionalanaesthesia.Anesth Analg.2004;98:835---40.
32.Hancı V, Erdogan G, Okyay RD, et al. Effects of fentanil-lidocaine-propofolanddexmedetomidine-lidocaine-propofolon trachealintubationwithoutuseofmusclerelaxants.Kaohsiung JMedSci.2010;26:244---50.
33.LiM,MeiW,WangP,etal.Propofolreducesearlypost-operative painaftergynecologicallaparoscopy.ActaAnaesthesiolScand. 2012;56:368---75.