REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
SCIENTIFIC
ARTICLE
Sympathetic
activity
of
S-(+)-ketamine
low
doses
in
the
epidural
space
Slobodan
Mihaljevic
∗,
Ljiljana
Mihaljevic,
Marko
Cacic
ClinicHospitalZagreb,UniversityofZagrebSchoolofMedicine,KliniˇckiBolniˇckiCentar,Zagreb,Croatia
Received23January2013;accepted22March2013 Availableonline23October2013
KEYWORDS
S-(+)-ketamine; Epiduralspace; Lowdoses;
Sympatheticactivity
Abstract
Backgroundandobjectives: S-(+)-ketamine is an intravenous anaesthetic and sympath-omimetic with properties of local anaesthetic. It has an effect of an analgetic and local anaestheticwhenadministeredepidurally,buttherearenodatawhetherlowdosesof S-(+)-ketaminehavesympathomimeticeffects.Theaimofthisstudywastodeterminewhetherlow dosesofS-(+)-ketamine,givenepidurallytogetherwithlocalanaesthetic,haveanyeffecton sympatheticnervoussystem,bothsystemicandbelowthelevelofanaestheticblock.
Methods:Thestudy wasconductedontwogroupsofpatients towhomepiduralanaesthesia was administered to.Localanaesthesia(0.5% bupivacaine)was giventoone group(control group) whilelocal anaesthesiaand S-(+)-ketamine were givento othergroup. Age, height, weight,systolic,diastolicandmeanarterialbloodpressureweremeasured.Non-competitive enzymeimmunochemistrymethod(CatCombiELISA)wasusedtodeterminetheconcentrations ofcatecholamines(adrenalineandnoradrenaline).Immunoenzymometricdeterminationwith luminescentsubstrateonamachinecalledVitrosEciwasusedtodeterminethe concentra-tionofcortisol.Pulsetransittimewasmeasuredusingphotoplethysmography.Mann---Whitney
U-test,WilcoxontestandFriedmanANOVAwerethestatisticaltests.Bloodpressure,pulse, adrenaline, noradrenaline andcortisol concentrations were measured in order toestimate systemicsympatheticeffects.
Results:40patientsinthecontrolgroupweregiven0.5%bupivacaineand40patientsinthe testgroupweregiven0.5%bupivacainewithS-(+)-ketamine.Valuep<0.05hasbeentakenas alimitofstatisticalsignificance.
Conclusions: Low dose of S-(+)-ketamine administered epidurally had no sympathomimetic effects;itdidnotchangebloodpressure,pulse,serumhormonesorpulsetransittime.Lowdose ofS-(+)-ketamineadministeredepidurallydidnotdeepensympatheticblock.Adding25mgof S-(+)-ketamineto0.5%bupivacainedoesnotdeprivesympathetictonusbelowthelevelof epidu-ralblockatthemomentofmostexpressedsympatheticblockandhasnoeffectonsympathetic tonusabovetheblocklevel.
© 2013SociedadeBrasileirade Anestesiologia.Publishedby ElsevierEditoraLtda.Allrights reserved.
∗Correspondingauthor.
E-mail:[email protected](S.Mihaljevic).
0104-0014/$–seefrontmatter©2013SociedadeBrasileiradeAnestesiologia.PublishedbyElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE
CetaminaS-(+); Espac¸oepidural; Dosesbaixas; Atividadesimpática
AtividadesimpáticadecetaminaS-(+)emdosesbaixasnoespac¸oepidural
Resumo
Justificativaeobjetivos: cetaminaS-(+)éumanestésicointravenosoesimpaticomiméticocom propriedadesdeanestésicolocal.Temefeitoanalgésicoedeanestésicolocalquando admin-istrada porviaepidural,mas nãohá dadosquerelatemse cetaminaS-(+)em dosesbaixas temefeitossimpaticomiméticos.OobjetivodesteestudofoideterminarsecetaminaS-(+)em dosesbaixas,administradaporviaepiduralemcombinac¸ãocomanestésicolocal,temalgum efeitosobreosistemanervososimpático,tantosistêmicoquantoabaixodoníveldobloqueio anestésico.
Métodos: oestudofoiconduzidocomdoisgruposdepacientessubmetidosàanestesiaepidural. Anestesialocal(bupivacaínaa0,5)foiadministradaaumgrupo(controle),enquanto aneste-sialocalem combinac¸ãocomcetaminaS-(+)foiadministradaaooutrogrupo(teste).Idade, altura,peso,pressãoarterialsistólicaediastólicaepressãoarterialmédiaforammedidos.O métodoimunoquímicodeinibic¸ãoenzimáticanãocompetitiva(CatCombiElisa)foiusadopara determinarasconcentrac¸õesdecatecolaminas(adrenalinaenoradrenalina).Oensaio imunoen-zimométricocomsubstratoluminescenteemumamáquinachamadaVitrosEcifoiusadopara determinaraconcentrac¸ãodecortisol.Otempodetransic¸ãodopulsofoimedidocom foto-pletismografia.Paraanáliseestatística,ostestesdeWilcoxon,UdeMann---WhitneyeAnovade Friedmanforamusados.Pressãoarterial,pulsoeconcentrac¸õesdeadrenalina,noradrenalina ecortisolforammedidosparaestimarosefeitossimpáticossistêmicos.
Resultados: receberambupivacaínaa5%40pacientesdogrupocontrolee40dogrupoteste receberambupivacaínaa0,5%comcetaminaS-(+).Umvalordep<0,05foiaceitocomoolimite designificânciaestatística.
Conclusões:dosebaixadecetaminaS-(+)administradaporviaepiduralnãoteveefeitos sim-paticomiméticos;não alterou a pressãoarterial, opulso, os hormôniosséricos ouo tempo detransic¸ãodepulso.DosebaixadecetaminaS-(+)administradaporviaepiduralnão apro-fundouobloqueiosimpático.Aadic¸ãode25mgdecetaminaS-(+)àbupivacaínaa0,5%não deprimiu otônus simpáticoabaixo do nível do bloqueio peridural nomomento máximode bloqueiosimpáticoenãotemefeitosobreotônussimpáticoacimadoníveldobloqueio. ©2013SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
Sympatheticactivityregulatesthebloodvessels’tonusand isconnectedwithhaemodynamicchanges.1
Epiduralsympatheticblocklessens bloodvessels’ vaso-constrictionoflowerextremitiesleadingto:
(a) lessened resistance in arterioles and increased blood flowthroughthem
(b) increasedamount of bloodflow due toreducedblood vessels’tonus
(c) increasedblood vesselscompliance--- changeof blood vessels’ volume perchange of pressureunit --- due to combineddecreaseofvasculartonus.1,2
Various drugs that have effect on paravertebral spinal nerves,spinal ganglia,ventralanddorsal spinal rootsand spinalcordaregivenintoepiduralspace.Theyblocksensor andmotorfibresbelowthepointatwhichanaestheticwas applied.2
S-(+)-ketamine, given intravenously, causes prominent cardiovascular stimulation --- increasing minute volume of the heart, myocardial oxygen consumption, heart rate, meanarterial andpulmonary pressureand centralvenous presure.3---5
LowdosesofS-(+)-ketamine,givenintravenously,cause haemodynamicchangeswithin5min.Arterialpressuregets increased10minafterinjectionandisaveragelyincreased by 23% maximum. Heart rate is averagely maximally increased15minafterinjection.Normalisationoccursafter 45min.
Photoplethysmography is a method that investigates blood volume pulsations by detection andreal-time anal-ysis of optic radiation, presenting periodical changes of lighttransmissionthroughskinwhichoccurduetochanges in tissue and arterial volume that are induced by the heart. Indirect methodfor estimating arterial compliance dependent onsympatheticactivity is measuringthepulse transmission time (Nitzan).6 Pulse transit time reflects
changes insympatheticactivity below thelevel of anaes-theticblock.6,7
Lumbar epidural anaesthesia, administered for opera-tionsoflowerabdomenandlowerextremities,isfollowed bylessenedsympatheticactivityinlowerabdomen,lower extremitiesandtoes,sothatpulsetransittimeisextended afterapplyingepiduralanaesthesia.8---10
Endocrinestressresponseinanaesthesiologyandsurgery ismediatedthrough:
• Neuropituitaryglandwithanti-diuretichormone(ADH) • Adenopituitarygland---suprarenalglandaxlewith
adreno-corticotropichormone(ACTH)andcortisol.11
BolusapplicationofS-(+)-ketamineleadsbyitself, with-out surgical stress, to general stimulation of endocrine stress response. Adrenaline and noradrenaline rise, while ACTH rises unsignificantly and ADH does not rise at all. ‘‘Dissociative anaesthesia’’, caused by ketamine, represents endogen psychical stress and contributes to stressresponse.4,11,12
Ketamine inhibits catecholamine re-uptake on sympa-theticend-plate, which can explainthe increased effects of endo- and egogenic catecholamines (adrenaline and noradrenalineconcentrationrises).Adrenaline,-mimetic, affects heart and metabolism, while noradrenaline, ␣ -mimetic,affectsbloodvesselsandbloodstream.12Epidural
anaesthesiapreventscatecholaminesecretionfromadrenal glandthathappensbecauseof stimulationfromoperation field. Epidural anaesthesia has no effect on secretion of cortisol, probably because afferent vagus paths are not blocked.
Materials
and
methods
Thisstudywasconductedwithapprovalofethical commit-teeof ClinicalhospitalZagreb andafter allpatients gave theirwritteninformedconsent.
Choosingpatients
Research of the sympathetic activity was made on 80 patients aged 18---45 years ASA II who underwent surgi-calinterventionunderepiduralanaesthesia.Patientswere introducedtocourse andaimsofthestudyanddrugs that aregoingtobeusedthroughthestudy thedaybeforethe operation.
Patientsweredividedintotwogroups:group1consisted of40patientswhoreceivedaninjectionof0.5%bupivacaine intoepiduralspaceandgroup2whoreceivedaninjection of0.5%bupivacaineandlowdose(25mg)ofS-(+)-ketamine intoepiduralspace.
Excludingcriteriawere:
1. ContraindicationsforEDAanaesthesia
2. Accompanyingcardiovasculardiseases(arteriosclerosis, hypertension, Raynaud syndrome), neuromuscular dis-eases,diabetes
3. Patients whose prescription therapy were vasoactive drugs
4. Patientsyoungerthan18yearsandolderthan45years. • 40 patients underwent surgical intervention under epiduralanaesthesiawithepiduralcatheterthatwas setonthelevelofL3---L4inlaterallyingposition • 0.5% isobaric bupivacaine, 1mL per segment, plus
0.1mLpersegmentforevery5cmforpatientshigher than150cmwasgivenintoepiduralspace
• Control group, consisting of 40 patients, underwent surgicalinterventionunderepiduralanaesthesiawith cathetersetonthelevelofL3---L4
• 0.3to0.75mlof0.5%isobaricbupivacainewasgiven intoepiduralspacepersecond.1mlpersegment,plus 0.1mlpersegmentforevery5cmforpatientshigher than150cm.
Anaesthesiaandmonitoring
Thenightbeforetheoperation,patientsweregiven5mgof diazepamorally,aswellas1hbeforetheoperation.
Everypatienttookeventuallyprescribeddrugsuptothe morningbeforetheoperation.
Veinpathway(cannula16G)wassetonaforearmbefore theanaesthesia.
500mL of 0.9% NaCl wasgiven several minutes before theoperationinordertocompensateexpecteddecreaseof arterialpressure.
Monitoring
Indirectmeasuring of the blood pressureusing automatic manometerbeforeandevery5minafterepidural anaesthe-sia,ECGIIlead,pulseoximetryonfingersandtemperature.
Haemodynamicparameters
- heartrate
- systolicbloodpressure - diastolicbloodpressure - meanarterialpressure
Epiduralanaesthesia
Epidural space was punctured and fitted with epidural catheteronthelevelofL3---L4usinghangingdroptechnique. Afterepiduralspacewasidentified,2mLof0.9%NaClwere injectedandafter that,thecatheterwasset 2---3cminto theepiduralspace.Catheterwasfixatedandthefilterwas set.
Correctpositionof catheterischeckedusingaspiration test---neitherbloodnorliquorisbeingaspirated---andtest dose---3mLof0.5%bupivacaine---inordertoexcludethe subarachnoidalcatheterposition.
Vasoactivehormones
Bloodwastakentodetermineconcentrationsofadrenaline, noradrenalineandcortisol30minbeforesettingvein path-way and again between 17 and 25min after epidural injection.
Non-competitiveenzymeimmunochemistrymethod(Cat Combi ELISA) was used to determine the concentrations ofcatecholamines(adrenalineandnoradrenaline).Sample shouldcontain1.1mLofplasmaorblood,takenbyEDTA.
Referentvalueofadrenalineinplasmais<0.69nmol/L, whilefornoradrenalineitis<3.55nmol/L.
Biopac system configuration for measuring PPG signal
AC/DC
Signal
Filter
AC
Signal
Analogue amplifier
AC
Signal
Digitalization
AC
Signal
Screen Software Record
Figure1 BiopacsystemconfigurationformeasuringPPG sig-nal.
Photoplethysmographicmeasurementtechnique (PPG)
PPG measurements were done on the second toe using Biopac system --- SS4LA pulse Plethysmograph Transducer whichusesinfraredlightsourceandphotodetector (Emit-ter/detector wavelength 860±900nm). Infrared light is modulated to a frequency of 3kHz. Detector’s output is filtered through a narrow tube on to 3kHz, in order to avoiddetectingthelightfromthebackground.Demodulated detector’soutputenablesPPGsignal,thatisfilteredthrough low-passing filter (Cut-off filter, wavelength 800nm), to reducehighfrequencynoise(Fig.1).
Recordingtechnique
Patient’slegwaslaiddowntosurfaceandfixated.PPGprobe wasfixatedontosecondtoein suchwaythatfixationdid notalterreceivedsignal.
PPG signal wasmeasured 3min, monitored inorder to correctdislocationsofasensororartefactsandsavedasa digitalrecordforfurtheranalysis.
First standard ECG lead was gathered and monitored simultaneouslywithrecordingPPGsignal.
Aftereveryexamination,PPGcurveswereshownonthe screenand thepart thatincludes 50 PPGpulses with rel-ativelylowfluctuations.ThefirststandardECGleadcurve simultaneouslywasshown.
Recorded data were marked in separate sequences of 180s and saved in separated files. Software enables repeateddisplayofunprocessed datasequence as contin-uoussignal.Thereisapossibilityofselectingunprocessed datawhichwereusedinfurtheranalysis.Screenwasused todisplaydata.Itshowscutofmeasurementintime.Yaxis showssignalpower.Cursorcanbeusedtomovesignalcuts intimeinbothdirections.Itispossibletogetareviewofthe wholerecordedsignal andanytimepointcanbeanalysed intodetails.
TimesofmeasuringPPGsignal
1. T1---5---10minbeforeepiduralinjection
2. T2---justbeforeadministering500mLofinfusion 3. T3---17---25minafterepiduralinjection
Patient’s position: 30% supination towards horizontal, patientliesstillonanoperationdesk.
Statisticalmethods
DataareshowninTable1withmedianandbelongingrange. Differencesbetweenthetwopatientgroups(group1vs. group2)weretestedwithnonparametrictestfor indepen-dentsamples(Mann---WhitneyU-test).
Differences between two single parameters measure-mentsofthesamepatientsweretestedwithnonparametric testfordependentsamples(Wilcoxontest).
Differences between three or more single parameters measurementsofthesamepatientsweretestedwith non-parametric analysis of variance for dependent samples (FriedmanANOVA).
Differences in changes of single parameters values in moremeasurementsbetweenbothgroupsofpatientswere testedwithvarianceanalysiswithrepeatedmeasurement.
Valuep<0.05hasbeentakenasalimitofstatistical sig-nificance.
Statisticalprocessinghasbeen madeonaPCusing pro-grammecalledStatistica6.
Results
Itisobviousthatbothgroupsofpatientswerehomogeneous inrelationtoage,weightandheightwhichenabledbetter comparisonandmoreaccurateresults.
Groups contained young people with well developed compensatorymechanisms.Therewerenostatistically sig-nificant differencesbetween patientsregarding age,body massandheight.Mann---WhitneyU-test(p=0.7234).
The dose of S(+)-ketamine given into epidural space was0.326mg/kg;altogethergivenvolumeofS(+)-ketamine given into epidural space respective to homogeneity of groups was 14.5mL of 0.5% bupivacaine(1.14mg/kg) and 1mL(25mg)ofS(+)-ketamine,asregards,0.326mg/kgbm (Fig.2).
TheresultsshowthataddingS(+)-ketamineto0.5% bupi-vacaine into epidural space before the skin incision was performeddidnotcauseanystatisticallysignificantchanges ofsystolicbloodpressure(Fig.3).
The results show that adding S(+)-ketamine to 0.5% bupivacaineintoepiduralspacebeforetheskin incisionis performeddidnotcauseanystatisticallysignificantchanges ofdiastolicbloodpressure(Fig.4).
Table1 Age,weightandheight.
Group1
N=40
Median(range)
Group2
N=40
Median(range)
Mann---WhitneyU-test
Age 41(23---45) 42(19---45) p=0.7234
Weight(kg) 84(60---102) 81.5(50---102) p=0.2910
Height(cm) 179(158---191) 176(152---188) p=0.1545
Pulsetransittime
PulsetransittimepresentsthetimeintervalbetweenRwave onECGandfirstvalueonPPGsignalcurve(Tables2and3). Pulse transit time in both groups did not change sig-nificantly after administering crystalloid infusion before anaesthesia(p=0.9031,Mann---WhitneyU-test)(Fig.11).
Pulse transit timeto toe changed significantly in both groups of patients after administering epidural
anaes-115
0 5 10
Minutes
Mm Hg
15 20
Group 1 Group 2
120 125 130 135 140 145 150
Figure2 Systolicpressure. Therewere nostatistically sig-nificantdifferences(p=0.22696)ofsystolicpressurebetween group1andgroup2inspecifiedmeasuremarks(repeated meas-uresANOVA).
84
82
80
78
76
74
72
70
68
66
0 5 10 15 20
Group 1 Group 2
Minutes
Mm Hg
Figure3 Diastolicpressure.Therewerenostatistically sig-nificant differences (p=0.40124) of diastolic blood pressure between the groups of patients in specified measure marks (repeatedmeasuresANOVA).
thesia, compared to state before administering epidural anaesthesia(Mann---Whitneytest).Group1:p=0.007,group 2:p=0.0079.However,therewasnosignificant difference inspecifiedmeasurementpointsbetweengroup1andgroup 2 (repeated ANOVA test). There were no significant dif-ferencesof pulsetransit time between groups that were
96
94
92
90
88
86
84
82
80
74 76 78
0 5 10 15 20
Group 1 Group 2
Minutes
Puls / min
ute
Figure4 Pulse.Therewerenostatisticallysignificant differ-ences(p=0.39709)inheartratebetweenthegroupsatthesame timeintervals(repeatedmeasuresANOVA).
0,00
M PDA
Min-Max
Nmol/L
25%-75% Median 0,01
0,02 0,03 0,04 0,05 0,06
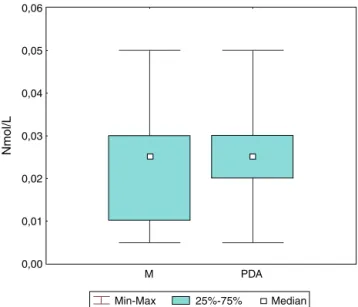
Figure 5 Adrenaline group 1. There were not statistically
Table2 Group1.Pulsetransittime.
Beforeanaesthesia
N=40
Median(range)
Anaesthesia
N=40
Median(range)
Wilcoxon’spairtest
T 0.3000
(0.2350---0.3458)
0.3050
(0.2667---0.3600)
p=0.0070
Table3 Group2.Pulsetransittime.
Beforeanaesthesia
N=40
Median(range)
Anaesthesia
N=40
Median(range)
Wilcoxon’spairtest
T 0.3000
(0.2350---0.3458)
0.3043
(0.2436---0.3795)
p=0.0071
administered epidural anaesthesia, despite the fact that group2wasadministeredlowdosesofS-(+)-ketamine epidu-rally(p=0.7043,Mann---WhitneyU-test).
Discussion
Spontaneous changes of heart rate, blood pressure and othercardiovascularsystemparametersarewellknown.13---15
Thesechangesareclassifieddependingontheirfrequency andeachfrequencyofchangescomesfromdifferent activ-ityoftwoautonomicnervoussystembranches---sympathetic andparasympathic.16
Ketamine causes prominent cardiovascular stimulation increasingminute volumeoftheheart,myocardialoxygen consumption,heartrate,meanarterialandpulmonary pres-sureandcentralvenouspresure.13,14,16,17
0,06
0,05
0,04
0,03
0,02
0,01
0,00
M PDA
Nmol/L
Min - max 25% - 75% Median
Figure6 Adrenaline group 2. Concentrationsofadrenaline
remained within referent values (p=0.0199, Wilcoxon test). M=beforeanaesthesia;PDA=afteranaesthesia.
AddingS-(+)-ketamine tobupivacaine intrathecally did notcausesignificantchangesofarterialpressurecompared togroupwhichwasgivenonlybupivacaine.12
Arterialcomplianceonfingerswasincreasedafter sym-patheticblock.6---9
Togal18 reports that S-(+)-ketamine administered
intrathecally to elder patients does not cause negative haemodynamiceffects.
Higher sympathetic activity above the place of block resultsinincreasedtonusanddecreasedcomplianceof cuta-neousarterias.6---9
Blood accumulation in lower body parts after apply-ingepiduralsympatheticblockdidnotsignificantlychange systolic,diastolicormeanarterialpressureneitheringroup 1(epiduralspace---0.5%bupivacaine)noringroup2 (epidu-ralspace---0.5%bupivacaineandS-(+)-ketamine).Therewas
0,14
0,12
0,10
0,08
0,06
0,04
0,02
0,00
M PDA
Nmol/L
Min - max 25% - 75% Median
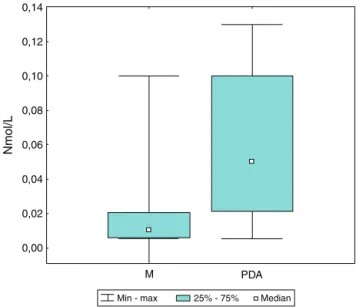
Figure7 Noradrenalinegroup1.Noradrenalineshowed
0,14
0,12
0,10
0,08
0,06
0,04
0,02
0,00
M PDA
Nmol/L
Min - max 25% - 75% Median
Figure 8 Noradrenaline group 2. Noradrenaline showed no
statisticallysignificantdifferences(p=0.7989)ingroup2when measuredduringepiduralanaesthesia.Itremainedwithin refer-entvalues(Wilcoxontest).M=beforeanaesthesia;PDA=after anaesthesia.
nostatisticallysignificantdifferencebetweengroup1and2 inspecifiedmeasuremarks(repeatedANOVAtest).
DespiteaddingS-(+)-ketamineintoepiduralspace,there were no blood pressure and heart rate changes during anaesthesia.Results obtained at patients whowere given S-(+)-ketamineepidurallyaresimilartoonesTogalobtained whenbupivacaineandS-(+)-ketamineweregiven intrathe-cally.Negativehaemodynamiceffectsofepidurallyinjected S-(+)-ketamineingroup2werenotcausedeitherbycentral orneuroaxialactivity.
Preoperational fluid compensation is important for patient’s intraoperational haemodynamic stability. Suffi-cient intravasal volume is inevitable for blood pressure
1000
800
600
400
200
0
M PDA
Nmol/L
Min - max 25% - 75% Median
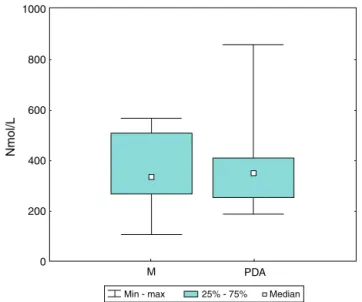
Figure 9 Cortisol group 1. There were no statistically sig-nificant changes (p=0.2297) of cortisol in group 1. Cortisol remained within referent values (Wilcoxon test). M=before anaesthesia;PDA=afteranaesthesia.
1000
800
600
400
200
0
M PDA
Nmol/L
Min - max 25% - 75% Median
Figure10 Cortisolgroup2.Therewere nostatistically sig-nificantchanges(p=0.2184)ofcortisol ingroup2,whichwas given0.5%bupivacaineintoepiduralspace.Cortisolremained withinreferentvalues(Wilcoxontest).M=beforeanaesthesia; PDA=afteranaesthesia.
stability and adequate tissue perfusion. Only because of not taking food and water from 10pm the day before the operation, there is a preoperative fluid deficit of averagely1400mL inadults.Crystal isotonicsolutions are distributed into extracellular space --- out of 1000mL of infused crystal solutions, after 1h only 200---300mL is stillplacedintravasally.19 Intravasalvolumeisdecisivefor
haemodynamicstability.
Bothgroupsofpatientsweregiven500mLofcrystalloids preoperativelyin ordertocompensate the bloodpressure drop caused by blocking sympathicus below the level of sympatheticblock.
Becausecrystalloidinfusionhadbeenadministeredinto epiduralspacebeforelocal anaesthetic,the infused crys-talloid remained within intravascular space and did not
M I PDA
Sec
0,34
0,33
0,32
0,31
0,30
0,29
0,28
0,27
0,26
Group 1 Group 2
redistributeintoextracellularspace.Thatcausedlessdrop ofbloodpressuredespitesympatheticblock.
Sincethepatients wereyoung andhadwell developed compensatory mechanisms, combination of preoperative volumecompensationandgoodcompensatorymechanisms contributed to haemodynamic stability in both groups of patient.
Anaesthetic primarily takes effect on nervous system, butisundoubtedlyrelatedwitheffectonendocrinesystem. Catecholaminesadrenaline andnoradrenalineandcortisol are important stress hormones which are being excreted as an outcome of different stress stimuli. Organism’s perioperative stress response is caused by more factors. Manypatientshaveanincreasedsympathetictonuscaused byfearanduncertaintyofthesurgicalinterventionalready preoperatively.Thiscanbeavoidedbytalkingtothepatient andexplaininghim theplannedcourseof anaesthesiaand operationasanadequatepremedication.11
In our study, an interview was done with the patients and anaesthesia protocol was explained. Patients were introducedtomedicamentsthatwillbeusedduring anaes-thesiaand weregivenpremedication. Inadditiontothat, theygavetheirwritteninformedconsent.
Informerstudiesdifferentlocalanaestheticswere com-paredandresultshaveshownthattherearedifferencesin theireffectonconcentrationsofcatecholaminesinplasma. When S-(+)-ketamine is intrathecally added to bupi-vacaine, there are no significant changes of arterial pressurecomparedtowhenonlybupivacaineisadministered intrathecally.18
Togal’s18 reportindicates that combinationsof
bupiva-caineandS-(+)-ketamine, administeredintrathecally, give resultsthatmatchourresults.Bupivacaineandlowdoseof S-(+)-ketamine,administered epidurally,donotcause sig-nificantchangesofheartrate,systolic,diastolicandmean arterialpressure,whicharethe reflectionof cardiovascu-lar sympathomimetic activity and concentration of stress hormonesinplasma.
Dahletal.20 provedthatsettingepiduralnervousblock
beforetheskinincision,usingonlylocalanaesthetic,does notsignificantlychangeconcentrationofstresshormonesin plasma.
Ourstudyshows thatconcentrationsof catecholamines and cortisol in plasma remain within referent values beforeandafteradministeringlumbarepiduralanaesthesia usingonly bupivacaine and administeringlumbar epidural anaesthesia using bupivacaine and S-(+)-ketamine. Stress responsewasabsentandconcentrationsofstresshormones werewithinreferentvaluesinbothgroupsofourpatients before and after administering epidural anaesthesia. We havetoemphasisethatmeasurementsweredonebeforethe skinincision,sothatsurgicalstressisexcluded.
Pulsetransittime
Babchenko2 comes to a cognition that lumbar epidural
anaesthesia,administeredforoperationsoflowerabdomen andlowerextremities,isfollowedbylessenedsympathetic activityinlowerabdomen,lowerextremitiesandtoes, so thatpulsetransittimeisextendedafterapplyingepidural anaesthesia.
Elyad21pointsoutthatpulsetransittimechanges(pulse
delay time)were significantlylongerat higher concentra-tionsoflocalanaesthetic.Thisparameterdependsondose andcanreflecthaemodynamicchangesinducedby sympa-thetic block withhigher reliabilitythan changes of blood pressureandtemperature.
LowdoseofS-(+)-ketamine,administeredepidurally,did notchangethepulsetransittime.
Sighampointsoutthatpulsetransittimechangesreflect autonomicresponsetonoxiousstimuliandchangesof anaes-thesia depth independently of heart rate. Pulse transit time at our patients reflects only the effect of lumbar sympatheticblockcausedbyadministering0.5%bupivacaine togroup 1 and 0.5%bupivacaine and low dose (25mg) of S-(+)-ketaminetogroup2(p>0.90138).
Inourstudy,therewerenonoxiousstimuliduringpulse transittimemeasuring,sotherewasnoautonomicnervous system responseto them. Therefore, thereis no statisti-cally significant difference of pulse transit time between patientsanaesthetisedwith0.5%bupivacaineandpatients anaesthetisedwith0.5%bupivacaineandlowdose (25mg) ofS-(+)-ketamine(p>0.903108).
Nitzan6citesthatlesseningofpulsetransittimerelative
topatient’sageisattributedtodirectstructurallesseningof arterialcompliance,notthefunctionaleffectsofincreased blood pressure combined with ageing, while parameters of pulsetransittimedonotdepend ondiastolicpressure, despitemeasurementaredoneattheendofdiastole.
Inourstudy,structurallesseningofarterialcompliancein respectofpatient’sagecouldnotaffectpulsetransittime. Averageageofgroup1was41(23---45).Averageage of group2was42(19---45).Therefore,thereisnostatistically significant difference (Mann---Whitney U-test, p=0.7234,
Table1)whichwouldaffectpulsetransittimedecrease. Babchenko2,6pointsoutthatarterialcompliancelessens
because of higher sympathetic activity which stretches arterial wall and increases pulse pressure velocity. Our patients were epidurally injected 0.5% bupivacaine which caused lessening arterial compliance, which was visible fromprolongedpulsetransittimeinspecifiedmeasurement pointsinbothgroupsofpatients(Wilcoxontest, ANOVAin specifiedmeasurementpoints,graph15).Lowdoseof S-(+)-ketamine(25mg)combinedwith0.5%bupivacainedidnot leadtoadditionalarterialcompliancelessening,whichcan be seen from changesof pulse transittime. Pulsetransit timeis an indirectscale for arterialcompliance. When S-(+)-ketamineisadministeredintravenously,bloodpressure andstrikingblood volumeget increased.However,we did notfindthosechangesonPPG curvewhenS-(+)-ketamine was administered epidurally in addition to bupivacaine, becausepulsetransittimewasnotstatisticallysignificantly changed.
OurresultshaveshownthatS-(+)-ketaminedidnottake effectonsympatheticblock,sowecanconcludethatitdid notdeepensympatheticblock.
Conclusion
sympatheticblockandsympathetictonusabovethelevelof sympatheticblock.Inotherwords,addinglowdoseof S-(+)-ketamineepidurally incombination with0.5% bupivacaine doesnotdeprivehaemodynamics.Therearenochangesof pulse,systolic, diastolic andmean arterialpressure when low dose(25mg)ofS-(+)-ketamine is administered epidu-rallyincombinationwith0.5%bupivacaine.Settingcentral nervousblockbeforeskinincision,usinglocalanaesthetic, and S-(+)-ketamine, leaves concentrations of stress hor-monesin plasma within referent values.Adding low dose ofS-(+)-ketamine intoepiduralspace incombination with 0.5%bupivacainedoesnothaveeffectonconcentrationof stresshormonesinplasma.
There is no change of sympathetic activity under the levelofblock,neitherarea,norpulsetransittimeonPPG curveiflowdose(25mg)ofS-(+)-ketamineisaddedto0.5% bupivacaine.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.GuytonAC,HallJE. Textbook ofmedicalphysiology.9thed. Philadelphia:W.B.SaundersCo.;1996[chapter18].
2.BabchenkoA, DavidsonE, AdlerS, Ginosar Y,Kurz V,Nitzan M. Increased pulse transit time to the foot following lum-bar epidural anesthesia. Med Biol Eng Comput. 2000;38: 674---9.
3.ZielmannN,KazmaierS,SchnullS,WeylandA.S(+)Ketamin undKreislauf.DerAnaesthesist.1997;46:43---6.
4.AdamsHA.EndokrineReaktionennachS(+)Ketamin.Der Anaes-thesist.1997;46:30---7.
5.AdamsHA,WernerC.VonRacematzumEutomer(S)Ketamin. Anaesthesist.1997;46:1026---42.
6.NitzanM,BabchenkoA,KhanokhB,LandauD.Thevariability ofthephotoplethysmographicsignal---apotentialmethodfor theevaluationoftheautonomicnervoussystem.PhysiolMeas. 1998;19:93---102.
7.Millasseau SC, Kelly RP, Ritter JM, Chowienzyk PJ. Deter-mination of age-related increases in large artery stiffness bydigital pulse contour analysis. Clin Sci (Lond). 2002;103: 371---7.
8.NitzanM,KhanokhB,SlovikY.Thedifferenceinpulsetransit timetothetoeandfingermeasuredbyphotoplethysmography. PhysiolMeas.2002;23:85---93.
9.Beene TK, Eggers Jr GW. Use of the pulse monitor for determining sympathetic block in the arm. Anesthesiology. 1974;40:412---4.
10.SubramaniamK,SubramaniamB,PawarDK,KumarL. Evalua-tionofthesafetyandefficacyofepiduralketaminecombined withmorphinefor postoperativeanalgesiaaftermajorupper abdominalsurgery.JClinAnesth.2001;13:339---44.
11.Dick A. Kombinationsanästhesie verindert die Stressantwort auf chirurgischen Reiz-Untersuchungen von hämodynamis-chen und hormonellen Regulationsvorgängen im vergleich zur balancierten Allgemeinenanästhesie. Dissertation Medi-zinischen Fakultät der Charite- Universitätsmedizin Berlin; 2005.
12.AdamsHA,BauerR,GebhardB,MenkeW,Baltes-Götz.TIVAmit S-(+)KetmaininderorthopädischenAlterschirurgieEndokrine Strereaktion,Kreislauf-undAufwachverhalten.Anaesthesist. 1994;43:92---100.
13.AkselrodS,GordonD,Madwed JB,SnidmanNC,ShannonDC, CohenRJ.Hemodynamicregulation:investigationbyspectral analysis.AmJPhysiol.1985;249:867---75.
14.Magnusdottir H, Kirno K, Rickstein SE, Elam M. High tho-racicepiduralanaesthesiadoesnotinhibitsympatheticnerve activity in the lower extremities. Anaesthesiology. 1999;91: 1299---304.
15.Pinna GD, Maesteri R, Mortara A. Estimation of arterial blood pressure variability by spectral analysis: comparison between Finapres and invasivemeasurements. Physiol Meas. 1996;17:147---69.
16.MartindaleSJ,DixP,StoddartPA.Double-blindrandomized con-trolled trial of caudal versus intravenous S-(+)-ketmaine for supplementationofcaudalanalgesiainchildren.BrJAnaesth. 2004;92:344---7.
17.Himmelseher S, Ziegler-Pithamitisis D, Argiriaridou H, Mar-tinJ, Jelen-EsselbornS,Kochs E.Small-dose S(+)ketamine reducespostoperativepainwhen appliedwithropivacainein epiduralanesthesiafortotalkneearthroplasty.AnesthAnalg. 2001;92:1290---5.
18.Togal T, Demirbilek S, Koroglu A, Yapici E, Ersoy O. Effects ofS(+) ketamineaddedto bupivacainefor spinal anaesthe-siaforprostatesurgeryinelderlypatients.EurJAnaesthesiol. 2004;21:193---7.
19.ScholzM.Mechanismsof(local)anaestheticsonvoltage-gated sodiumandotherionchannels.BrJAnaesth.2002;89:52---61. 20.Dahl JB, RosenbergJ, Kehlet H. Effect of thoracic epidural
etidocaine1.5%onsomatosensoryevokedpotentials,cortisol andglucoseduringcholecystectomy.ActaAnaesthesiolScand. 1992;36:378---82.
21.ElyadM, DavidsonMD, Yehuda G, NitzanM. Erhöhte
Impuls-durchfahrzeitzumFußlumbarerEpiduralAnästhesiefolgend.