www.jped.com.br
ORIGINAL
ARTICLE
Influence
of
maternity
leave
on
exclusive
breastfeeding
夽
Fernanda
R.
Monteiro
a,∗,
Gabriela
dos
S.
Buccini
b,
Sônia
I.
Venâncio
c,
Teresa
H.M.
da
Costa
daUniversidadedeBrasília(UnB),FaculdadedeCiênciasdaSaúde,ProgramadePós-graduac¸ãoemCiênciasdaSaúde,Brasília,DF,
Brazil
bUniversidadedeSãoPaulo(USP),FaculdadedeSaúdePública,DepartamentodeNutric¸ão,SãoPaulo,SP,Brazil cSecretariadeEstadodaSaúdedeSãoPaulo,InstitutodeSaúde,SãoPaulo,SP,Brazil
dUniversidadedeBrasília(UnB),FaculdadedeCiênciasdaSaúde,DepartamentodeNutric¸ão,Brasília,DF,Brazil
Received25July2016;accepted10November2016 Availableonline21July2017
KEYWORDS
Exclusive breastfeeding; Maternityleave; Womenandwork
Abstract
Objectives: To describe the profile ofwomen with children aged under 4 months living in theBrazilianstatecapitalsandintheFederalDistrictaccordingtotheirworkingstatusand toanalyzetheinfluenceofmaternityleaveonexclusivebreastfeeding(EBF)amongworking women.
Methods: Thiswasacross-sectionalstudy withdata extractedfromtheIINationalMaternal BreastfeedingPrevalenceSurveycarriedoutin2008.Initially,adescriptiveanalysisoftheprofile of12,794womenwasperformed,accordingtotheirworkingstatusandmaternityleaveandthe frequencyofmaternityleaveintheBrazilianregionsandcapitals.Thestudyusedamultiple modeltoidentifytheinfluenceofmaternityleaveonEBFinterruption,including3766women whodeclaredtheywereworkingandwereonmaternityleaveatthetimeoftheinterview.The outcomeassessedinthestudywastheinterruptionoftheEBF,classifiedbytheWHO. Results: Regarding theworkingstatus ofthe mothers, 63.4% didnot workoutside oftheir homesandamongthosewhoworked,69.8%wereonmaternityleave.Thelargestprevalence amongworkerswasofwomenolderthan35yearsofage,withmorethan12yearsofschooling, primiparousandfromtheSoutheastandSouthregions.Thelackofmaternityleaveincreased by23%thechanceofEBFinterruption.
夽
Pleasecitethisarticleas:MonteiroFR,BucciniGS,VenâncioSI,CostaTH.Influenceofmaternityleaveonexclusivebreastfeeding.J Pediatr(RioJ).2017;93:475---81.
∗Correspondingauthor.
E-mail:[email protected](F.R.Monteiro).
http://dx.doi.org/10.1016/j.jped.2016.11.016
0021-7557/©2017SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-ND
Conclusion: Maternity leave contributedto increase the prevalenceofEBF inthe Brazilian statescapitals,supportingtheimportanceofincreasingthematernityleaveperiodfromfour tosixmonths.
©2017SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/ 4.0/).
PALAVRAS-CHAVE
Aleitamentomaterno exclusivo;
Licenc¸a-maternidade; Mulheretrabalho
Influênciadalicenc¸a-maternidadesobreaamamentac¸ãoexclusiva
Resumo
Objetivos: Descreverperfildasmulherescomfilhosmenoresde4mesesresidentesnascapitais brasileirasenoDistritoFederalsegundosituac¸ãodetrabalhoeanalisarainfluênciadalicenc ¸a-maternidadesobreoaleitamentomaternoexclusivoentreasmulherestrabalhadoras. Métodos: Trata-sede umestudotransversal comdadosextraídosdaIIPesquisaNacionalde PrevalênciadoAleitamentoMaternorealizadaem2008.Inicialmentefoirealizadaanálise des-critivadoperfildas10.995mulheresparticipantesdoestudosegundosituac¸ãodetrabalhoede licenc¸a-maternidade,bemcomo afrequênciadelicenc¸a-maternidadenasregiõesbrasileiras ecapitais.Emseguida,paraidentificarainfluênciadalicenc¸a-maternidadenainterrupc¸ãodo aleitamentomaternoexclusivo,realizou-semodelomúltiplo,ondeforamincluídas3.766 mul-heresquedeclararamtrabalhareestaremlicenc¸a-maternidadenomomentodaentrevista.O desfechoadotadonoestudofoiainterrupc¸ãodoaleitamentomaternoexclusivo,classificado deacordocomadefinic¸ãodaOrganizac¸ãoMundialdaSaúde.
Resultados: Em relac¸ãoàsituac¸ão detrabalho,63,4%das mãesentrevistadas noBrasil não trabalhavam fora do lar e dentre as que trabalhavam fora, 69,8% usufruíam da licenc ¸a-maternidade.Verificou-semaiorconcentrac¸ãodemulheresquetrabalhavamforaentreaquelas commaisde35anos,maisde12anosdeescolaridade,primíparas,dasregiõesSudesteeSul. Paraas mulheres quenão estavam em licenc¸a-maternidade, apósajuste para todas as co-variáveis,houveumaumentodaprevalênciadeinterrupc¸ãodoaleitamentomaternoexclusivo (RP[IC95%]ajustada1,23[1,11---1,37]).
Conclusão: Verificou-sequeasmulheresquenãoestavamemlicenc¸a-maternidadede120dias apresentarammaiorprevalênciadeinterrupc¸ãodoaleitamentomaternoexclusivonascapitais brasileiraseDistritoFederal,noanode2008,reforc¸andoaimportânciadaampliac¸ãodalicenc ¸a-maternidadepara6meses.
©2017SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Este ´eumartigo OpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4. 0/).
Introduction
Exclusivebreastfeeding(EBF)offersmanybenefits forthe health of infants and their mothers.1 However, it is
esti-matedthatonly37%ofchildrenunder6monthsofageare exclusivelybreastfedworldwide,areality thatisfar from thatrecommendedbytheWorldHealthOrganization(WHO), which has established an EBF prevalence goal of 50% by 2025.2 In Brazil, the II Maternal Breastfeeding Prevalence
Survey (Pesquisa Nacional de Prevalência de Aleitamento Materno[PPAM]),carriedoutin2008,foundthat41%of chil-dren under 6 months of age were exclusively breastfed.3
Consideringthisscenario,identifyingfactorsandstrategies thatmay contribute toincrease EBF is a worldwide chal-lenge.Amongthefactorsassociatedwithearlyinterruption ofEBF,maternalworkoutsideofthehomehasbeen identi-fiedasanobstacle.4---8
TheInternationalLaborOrganization(ILO),inthe begin-ning of the 20th century, held in Washington their third conventiononwomen’semploymentbeforeandafter child-birth.In1935,Brazilratified therecommendationsofthis
convention,whichguaranteedreturntoworkatsixweeks ofpostpartumandtwohalf-hourbreakstobreastfeed dur-ing the working day.9 In 1988, the Brazilian Constitution
establishedthewomen’sright toamaternityleavelasting 16 weeks (120 days),10 longer than the 14-week
interna-tionalmaternityleaverecommendation(ILOn.183/2000).11
I In 2008, Law n. 11,770 was passed, giving women the option to extend the maternity leave to 180 days (24weeks).12
Concernsabout maternal work and breastfeedinghave increasedduetothegrowingparticipationofwomeninthe labor market,13,14 makingitimpossible for womentostop
workingforanunpaidperiodtodedicatethemselvestothe care of their children, which can lead to changes in the childcareandfeedingpatterns.
toanalyzetheinfluence ofmaternityleave onEBFamong womenworkingoutsideofthehome.
Methods
This is a cross-sectional study,whose data were obtained fromtheIIPPAMcarriedoutin2008.Thissurveycollected information fromchildren under 1 year of age who were brought for the second phase of the 2008 multi-vaccine campaign in all Brazilian capitals and in the Federal Dis-trict(DistritoFederal[DF]).ThePPAMwascarriedoutusing conglomeratesamples, by drawinglots in two stages and probabilityproportionaltothesizeoftheconglomerates.
In the first stage, the vaccination units were selected bydrawinglots,andinthesecond,thechildrenwere sys-tematicallyselectedineachunit,alsobydrawinglots.The sample size considered information onthe distributionof vaccinatedchildrenineachvaccinationunitin2007andthe prevalenceofEBFobtainedattheIPPAM,carriedoutin1999 inthe26capitalsandintheDF.15Detailsonthesampling
pro-cedureshavebeendescribedinpreviouspublications.3,16To
reachtheaimsofthisstudy,childrenunder4monthsofage wasanalyzed,theagerangeinwhichitwouldbepossible formotherstobeonmaternityleavein2008.
The data collection tool wasapplied to the children’s caregiversduringthevaccinationcampaign.The question-nairecontainedclosedquestionsaboutthecharacteristics of the children and their mothers, about infant feeding in the last 24h, and about the healthcare services they attended.Themothersalsostated,atthetimeofthe inter-view, whether theywere working outside of thehome or not,andwhethertheywereonmaternityleave.The data wereentered intoawebapplication byteammembersin eachmunicipality.
Initially, a descriptive analysis was performed on the profile of the 10.995 women participating in the study, according totheir workingstatus andmaternity leave, as wellasthefrequencyofmaternityleaveinBrazilianregions and capitals. Subsequently, to identify the influence of thematernityleaveonEBFinterruption,amultiplemodel wasdeveloped,whichincluded onlythe3766 womenwho reportedworkingoutsideofthehomeorbeingonmaternity leaveatthetimeoftheinterview.Theoutcomeadoptedin thepresentstudywasEBFinterruption,classifiedaccording totheWHOdefinition.17
Themainindependentvariablewaswhethertheworking motherwasor not onmaternity leave at the timeof the interview. The following variables were analyzed: mater-nal age(<20,20---35, >35years),maternal schooling(0---8, 9---12, >12 years of schooling), primiparity (yes/no), type ofdelivery(vaginal/forceps,cesareansection),thechild’s gender (female/male), low birth weight (yes/no), health care(PublicNetwork---SistemaÚnicodeSaúde[SUS]; Pri-vateService/HealthInsurance),pacifieruseinthelast24h (yes/no),andthechild’sage(0---60daysand61---120days). Poisson regressionwasusedtoestimatetheprevalence ratio(PR)and95%confidenceintervals(95%CI),withrobust varianceforbivariateandmultipleanalyses.Variablesthat showed p<0.20 in the bivariate analysiswere introduced in the multiple model. In the multiple model, variables thatshowedp<0.05wereconsideredtobeassociatedwith
the outcome. A linear trend test was performed for the variablesinwhichtherewasatheoreticalassumptionofa dose---responseassociation. Althoughthechild’sagewasa controlvariable,amultiplemodelwastestedwiththeage variablecategorizedfrommonthtomonth.Inthisanalysis, therewasnorelevantadjustment inthe prevalenceratio oftheresponse variable,and thus,this approachwasnot explored(datanotshown).
TheIIPPAMdatabasewasexportedtotheStatasoftware (Stata Statistical Software: Release 9. StataCorp., 2005, College Station, TX, USA) for data analysis. The sample complexity was considered at all analytical stages of the analysis.15
TheresearchprotocolwasapprovedbytheEthics Com-mittee of Instituto de Saúde de São Paulo (Protocol n. 001/2008, of 05/06/2008), after consulting the National CommissionforResearchEthics(ComissãoNacionaldeÉtica emPesquisa[CONEP]).
Results
The study involved 12,794 women with children under 4 monthsofage,fromwhich10.995motherrepliedregarding theworkvariable.Halfofthesample consistedofwomen withmalechildrenandtheinfants’meanagewas59.5days. Itwasverifiedthat37.4%ofthechildrenwerebornina hos-pitalaccredited asa ‘‘Child-Friendly Hospital’’;low birth weightoccurred in8.7% ofthecasesand pacifieruse was reportedfor 36.4% of the children. In the analyzed sam-ple,51% of the children were exclusively breastfed.Half of the mothers were primiparous, 18.4% were under 20 years of age, and 47.6% of the mothers had 9---12 years ofschooling.Regardingtheworking statusatthe moment ofthe interview,it wasverifiedthat63.4% of thewomen interviewedinBrazildidnotworkoutsideofthehome.Of thoseworkingoutsideofthehome,69.8%wereonmaternity leave.
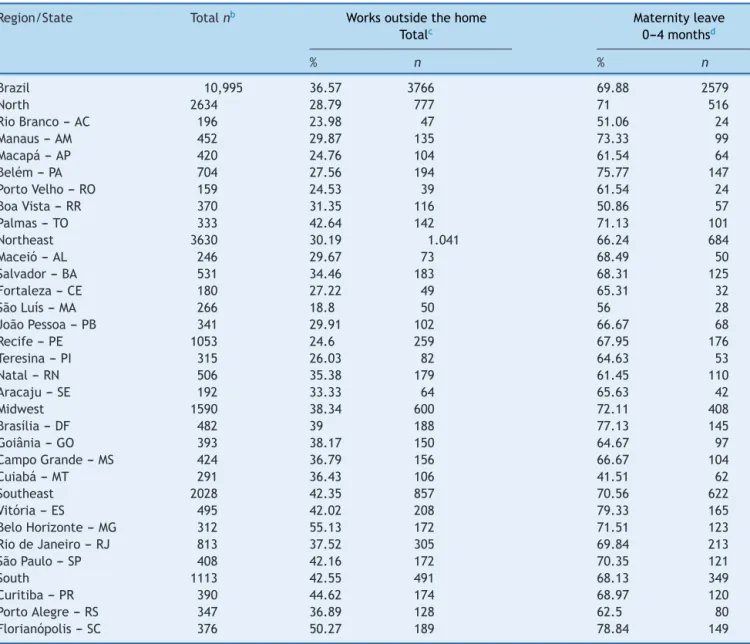
Table 1 shows the distribution of women in Brazilian capitalsand in the DF regarding their working statusand maternityleave.Itwasimportanttocharacterize the pro-fileofwomenaccordingtotheworkingstatustounderstand thecharacteristicsofthosewhodidnotworkoutsideofthe home.Therewasa greatvariabilityamongthecapitalsin relationtotheworkingstatusatthetimeoftheinterview, anditwasverifiedthatlessthan25%ofthewomenreported workingoutsideofthehomeinsomeofthecapitalslocated intheNorthandNortheastregions.Thesamevariabilitywas observedinrelationtotheprevalenceofwomenon mater-nityleave, with theSoutheast and Southregions showing thehighest percentagesof women workingoutside ofthe home.
Table1 Frequencyofmaternityleaveaandmaternalworkingstatus,stratifiedby Brazilianregionsandbycapitalofeach
state.IIMaternalBreastfeedingPrevalenceSurveyintheBrazilianCapitalsandFederalDistrict,2008.
Region/State Totalnb Worksoutsidethehome Maternityleave
Totalc 0---4monthsd
% n % n
Brazil 10,995 36.57 3766 69.88 2579
North 2634 28.79 777 71 516
RioBranco---AC 196 23.98 47 51.06 24
Manaus---AM 452 29.87 135 73.33 99
Macapá--- AP 420 24.76 104 61.54 64
Belém--- PA 704 27.56 194 75.77 147
PortoVelho--- RO 159 24.53 39 61.54 24
BoaVista---RR 370 31.35 116 50.86 57
Palmas---TO 333 42.64 142 71.13 101
Northeast 3630 30.19 1.041 66.24 684
Maceió---AL 246 29.67 73 68.49 50
Salvador---BA 531 34.46 183 68.31 125
Fortaleza---CE 180 27.22 49 65.31 32
SãoLuís---MA 266 18.8 50 56 28
JoãoPessoa---PB 341 29.91 102 66.67 68
Recife---PE 1053 24.6 259 67.95 176
Teresina---PI 315 26.03 82 64.63 53
Natal---RN 506 35.38 179 61.45 110
Aracaju---SE 192 33.33 64 65.63 42
Midwest 1590 38.34 600 72.11 408
Brasília---DF 482 39 188 77.13 145
Goiânia---GO 393 38.17 150 64.67 97
CampoGrande---MS 424 36.79 156 66.67 104
Cuiabá---MT 291 36.43 106 41.51 62
Southeast 2028 42.35 857 70.56 622
Vitória---ES 495 42.02 208 79.33 165
BeloHorizonte---MG 312 55.13 172 71.51 123
RiodeJaneiro---RJ 813 37.52 305 69.84 213
SãoPaulo---SP 408 42.16 172 70.35 121
South 1113 42.55 491 68.13 349
Curitiba--- PR 390 44.62 174 68.97 120
PortoAlegre--- RS 347 36.89 128 62.5 80
Florianópolis--- SC 376 50.27 189 78.84 149
aMaternityleavereportedbythemother.
b Thisanalysisincludedalltheparticipatingwomenwhoansweredthequestionrelatedtothematernalworkingstatus(totaln=10,995). c %inrelationtothetotalofwomenparticipantswhoansweredthequestionrelatedtothematernalworkingstatus(totaln=10,995). d %inrelationtothetotalnumberofwomenwhoreportedworkingoutsideofthehome(n=3766).
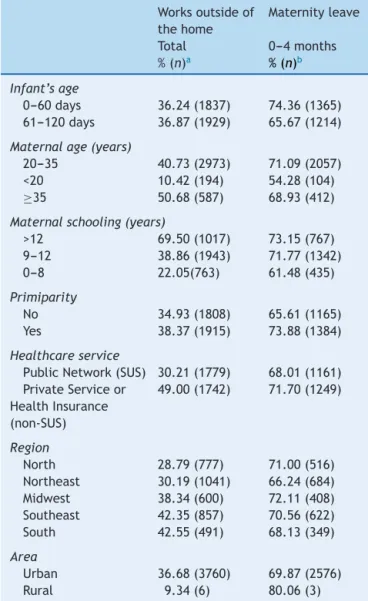
primiparous, thosewho had health insuranceor usedthe privatehealthcarenetwork,andthoselivingintheMidwest andNorthregions.
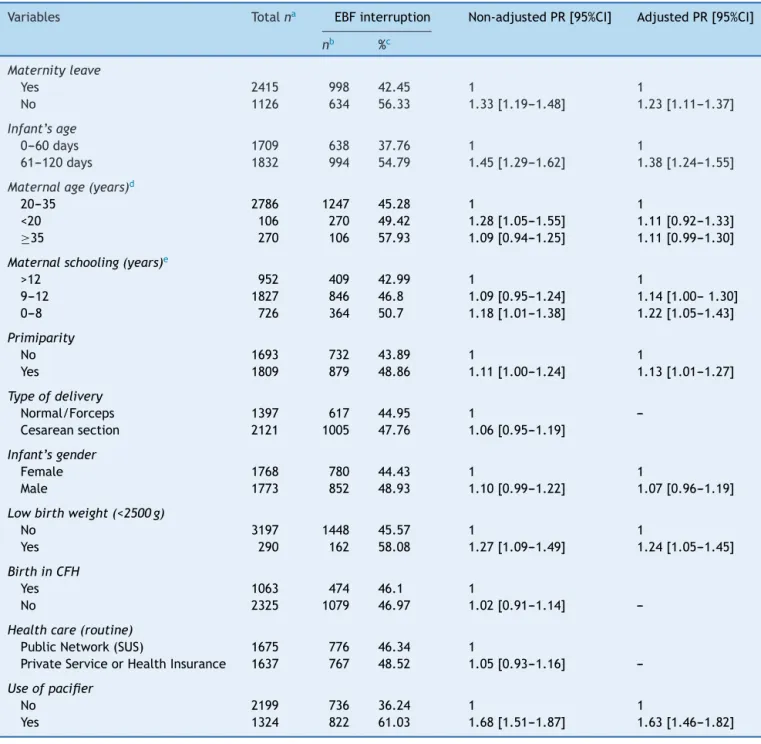
Table3showstheresultsofthegrossandadjusted anal-ysis of the association between maternity leave and EBF interruptionfor theworking mothers’ population.Forthe women not in the LMAT, after adjust in all co-variables, therewasanincreaseintheprevalenceoftheinterruption oftheAME(RP[IC95%]adjusted 1,23[1,11---1,37]). Chil-drenwithlowbirthweightwhousedpacifiersandchildren of primiparous mothers alsohad a greater chance of EBF interruption. Moreover, a dose---response component was observedbetweenmaternalschoolingandEBFinterruption,
i.e.,thelowerthewoman’seducationallevel,thegreater theriskofEBFinterruption(p=0.01).
Discussion
This is the firststudy of national scope that assesses the association between maternity leave and EBF prevalence andpresentstheresultsaccordingtoBrazilianregionsand capitals,basedonthedataobtainedintheIIPPAM,inthe BrazilianCapitalsandFederalDistrict,heldin2008bythe MinistryofHealth.
Table2 Profile ofthe women according tothe working statusandmaternityleavesituation.IIMaternal Breastfeed-ingPrevalenceSurveyintheBrazilianCapitalsandFederal District,2008.
Worksoutsideof thehome
Maternityleave
Total 0---4months %(n)a %(n)b
Infant’sage
0---60days 36.24(1837) 74.36(1365) 61---120days 36.87(1929) 65.67(1214)
Maternalage(years)
20---35 40.73(2973) 71.09(2057) <20 10.42(194) 54.28(104)
≥35 50.68(587) 68.93(412)
Maternalschooling(years)
>12 69.50(1017) 73.15(767) 9---12 38.86(1943) 71.77(1342)
0---8 22.05(763) 61.48(435)
Primiparity
No 34.93(1808) 65.61(1165)
Yes 38.37(1915) 73.88(1384)
Healthcareservice
PublicNetwork(SUS) 30.21(1779) 68.01(1161) PrivateServiceor
HealthInsurance (non-SUS)
49.00(1742) 71.70(1249)
Region
North 28.79(777) 71.00(516)
Northeast 30.19(1041) 66.24(684) Midwest 38.34(600) 72.11(408) Southeast 42.35(857) 70.56(622)
South 42.55(491) 68.13(349)
Area
Urban 36.68(3760) 69.87(2576)
Rural 9.34(6) 80.06(3)
a %inrelationtothetotalnumberofwomenwhoanswered
the question related to the maternal working status (total
n=10,995).
b %inrelationtothetotalnumberofwomenwhoreported
workingoutsideofthehome(n=3766). SUS,BrazilianUnifiedHealthSystem.
2009,therewasanincreaseinthisparticipation,from32% to46%intheUnitedStates,from25%to47%inCanada,and from21%to41%inLatinAmericaandtheCaribbean.13,14In
Brazil,in1996, approximately21% ofBrazilianhouseholds hadafemaleheadofthefamily,andin2012,37.4%ofthe familieshadawomaninchargeofthehousehold.18
Among workingmothers,itwasobservedthatthoseon maternityleavehadalowerchanceofEBFdiscontinuation inthefirstfourmonthsoftheinfant’slife,afteradjusting forotherfactorsindicatedinotherstudiesasdeterminants or associated toEBF, suchasmaternal level of schooling, parity,lowbirthweight,andpacifieruse.4---8,19
Corroborating the present findings,a studycarried out by Venâncio et al.20 in 77 municipalities in the state of
SãoPaulo alsoshowed ahigher percentageof EBF among motherswhowereonmaternityleave(54.6%)andalower percentage(25.6%)amongthosewhowereworkingwithout maternityleave. Similarly, Viannaetal.,21 ina study
car-riedoutin70municipalitiesinthestateofParaíba,verified thatmaternity leave positivelyinfluenced the prevalence of EBF. A North-American study carried out by Mirkovic etal.,22whoanalyzedtheinfluenceofmaternityleave
dura-tion and working hours on breastfeeding duration, found thatreturningtowork before3 monthsof postpartum on afull-timebasisreducedthechanceofwomenreachingthe periodtheyhaddeclaredasbeingtheirintentionto breast-feed.Itisworthmentioningthatstudieshavedemonstrated theinfluence of maternity leave onthe total duration of breastfeeding,23inadditiontobenefitsrelatedtothe
reduc-tionininfantmortalityrates.24,25
The adoption of strategies and legislations to protect workingwomenwhobreastfeedhasbeenemphasizedin sev-eraldocumentsbyinternationalorganizations,suchasthe InnocentiDeclarationonProtection,Promotion,andSupport ofBreastfeeding(1990)andthe GlobalStrategy forInfant andYoung ChildFeeding in Early Childhood.26 The
Brazil-ianMinistryofHealthhasdevelopedsomestrategies,such astheBreastfeedingProgramSupportforWorkingWomen, whichaimstostimulatemanagersofpublicandprivate com-paniestoadheretothesix-monthmaternityleave,havinga daycareattheworkplaceandabreastfeedingsupportroom. AlthoughBrazilhasstoodoutintheinternationalscenario asone of the countries that offers the longest maternity leavein weeks andthe highest percentageof wagespaid tothewomen,27 theseventhinarankingof202countries
surveyed by the United Nations, further actions are still required.
Breastfeedingamongworkingwomenisacomplex sub-jectandpermeatedbymanychoices,oftenrequiringmore thanemployeebenefitsforthecontinuationofEBF.28
Sev-eralauthors point outthat EBF rates varyworldwideand thatpostpartumsupporttechnologies,suchas breastfeed-ingsupportatworkplaces,breaksduringworkinghoursfor breastfeeding,maternity leave, andprofessional counsel-ingandlactationmanagementduringthistransitionperiod ofreturningtoworkarepositivefactorsforbreastfeeding stimulation.29
Somestudy limitationsarenoteworthy. Secondarydata were used, and the set of variables available was used toconstruct the model. Nonetheless,important variables pointed out in the literature related to the mother and childwereincluded.30Duetothecross-sectionaldesign,the
resultsshown heremaybeusefultoformulatehypotheses andnottoestablishacausalassociation.Inthissense,the authorsverifiedthatmaternityleavecaninfluencethe dura-tionof the EBF, but longitudinal studies arenecessary to confirmthishypothesis.The dataanalyzedherewere col-lectedin2008and,thus,thereisatemporaldistancefrom thepresent,buttherearenodataofnationalscopeonthe subject,emphasizingtheimportanceofthisresearch.
Table3 CrudeandadjustedanalysisbyPoissonregressionofexclusivebreastfeedinginterruptionamongworkingwomenand covariables.IIMaternalBreastfeedingPrevalenceSurveyintheBrazilianCapitalsandFederalDistrict,2008.
Variables Totalna EBFinterruption Non-adjustedPR[95%CI] AdjustedPR[95%CI]
nb %c
Maternityleave
Yes 2415 998 42.45 1 1
No 1126 634 56.33 1.33[1.19---1.48] 1.23[1.11---1.37]
Infant’sage
0---60days 1709 638 37.76 1 1
61---120days 1832 994 54.79 1.45[1.29---1.62] 1.38[1.24---1.55]
Maternalage(years)d
20---35 2786 1247 45.28 1 1
<20 106 270 49.42 1.28[1.05---1.55] 1.11[0.92---1.33]
≥35 270 106 57.93 1.09[0.94---1.25] 1.11[0.99---1.30]
Maternalschooling(years)e
>12 952 409 42.99 1 1
9---12 1827 846 46.8 1.09[0.95---1.24] 1.14[1.00---1.30] 0---8 726 364 50.7 1.18[1.01---1.38] 1.22[1.05---1.43]
Primiparity
No 1693 732 43.89 1 1
Yes 1809 879 48.86 1.11[1.00---1.24] 1.13[1.01---1.27]
Typeofdelivery
Normal/Forceps 1397 617 44.95 1
---Cesareansection 2121 1005 47.76 1.06[0.95---1.19]
Infant’sgender
Female 1768 780 44.43 1 1
Male 1773 852 48.93 1.10[0.99---1.22] 1.07[0.96---1.19]
Lowbirthweight(<2500g)
No 3197 1448 45.57 1 1
Yes 290 162 58.08 1.27[1.09---1.49] 1.24[1.05---1.45]
BirthinCFH
Yes 1063 474 46.1 1
No 2325 1079 46.97 1.02[0.91---1.14]
---Healthcare(routine)
PublicNetwork(SUS) 1675 776 46.34 1
PrivateServiceorHealthInsurance 1637 767 48.52 1.05[0.93---1.16]
---Useofpacifier
No 2199 736 36.24 1 1
Yes 1324 822 61.03 1.68[1.51---1.87] 1.63[1.46---1.82]
PR,prevalenceratio;CFH,Child-FriendlyHospital;SUS,BrazilianUnifiedHealthSystem.
aTotalnumberofinfantsunder4monthsofagewhosemothersdeclaredworkingoutsidethehomeoronmaternityleaveatthetime
oftheinterview.
b Infantsunder4monthsofagewhodiscontinuedexclusivebreastfeeding.
c %ofinfantsunder4monthsofagewhointerruptedexclusivebreastfeedingconsideringthesampleweightofeachcapital. d poflineartendency>0.05.
e poflineartendency<0.05.
decisions that will benefit thousands of Brazilian women withtheincreaseofmaternityleave.
Funding
Thedata analyzedin thearticle wereextracted fromthe II PPAM, carried out in 2008 and funded by the Brazilian MinistryofHealth.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
2.World Health Organization [WHO]. Sixty-fifth World Health Assembly.Resolutionsanddecisions.Geneva:21---26may;2012.
3.VenancioSI,EscuderMM,SaldivaSR,GiuglianiER.Apráticado aleitamentomaternonascapitaisbrasileiraseDistritoFederal: situac¸ãoatualeavanc¸os.JPediatr(RioJ).2010;86:317---24.
4.Vieira TO,Vieira GO, OliveiraNF, Mendes CM, Giugliani ER. Duration of exclusive breastfeeding in Brazilian population: newdeterminantsincohortstudy.BMCPregnancyChildbirth. 2014;14:175.
5.SanchesMT,Buccini GS, GimenoSG, RosaTE,BonamigoAW. Factorsassociatedwithinterruptionofexclusivebreastfeeding inlowbirthweightinfantsreceivingprimarycare.CadSaúde Públ.2011;27:953---65.
6.ParizotoGM, ParadaCM, VenâncioSI,Carvalhaes MA.Trends andpatternsofexclusivebreastfeedingforunder-6-month-old children.JPediatr(RioJ).2009;85:201---8.
7.Damião JJ. Influence of mothers’ schooling and work on thepracticeof exclusivebreastfeeding. RevBrasEpidemiol. 2008;11:442---52.
8.LindauJF,MastroeniS,GaddiniA,LalloDD,NastroPF,PatanèM, etal.Determinantsofexclusivebreastfeedingcessation: identi-fyingan‘‘atriskpopulation’’forspecialsupport.EurJPediatr. 2014;174:533---40.
9.Brasil. Poder Executivo. Decreto n◦. 423 (Nov 12, 1935).
Convenc¸ãorelativa aoempregodasmulheresantesedepois do parto. Available from: http://www.ilo.org/brasilia/ convencoes/WCMS 234869/lang–pt/index.htm [cited 12.06.16].
10.Brasil.Constituic¸ãodaRepúblicaFederativadoBrasil.Brasília (DF):SenadoFederal;1998.
11.Trabalhoefamília:rumoanovasformasdeconciliac¸ãocom cor-responsabilidadesocial/Organizac¸ãoInternacionaldoTrabalho. Brasília:OIT;2009.
12.Brasil. Lei n◦ 11.770, Lei da Licenc¸a Maternidade, de 9 de
setembrode2008.CriaoProgramaEmpresaCidadã,destinado
àprorrogac¸ãodalicenc¸amaternidademedianteconcessãode
incentivofiscal,ealteraaLein.8.212dejulhode1991.Brasília,
9September2008.
13.WorldBank.Worlddevelopmentindicators2002.Washington,
DC:Int.BankReconstr.Dev./WorldBank;2002.Availablefrom:
http://www-ds.worldbank.org/external/default/WDSContent Server/IW3P/IB/2002/10/12/0000949460210120412542/ Rendered/PDF/multi0page.pdf[cited10.12.15].
14.WorldBank.Worlddevelopmentindicatorsonline.Washington,
DC:WorldBank;2012.Availablefrom:http://data.worldbank.
org/data-catalog/world-development-indicators [cited 12.06.15].
15.Brasil.Ministério da Saúde. Secretaria de Atenc¸ão à Saúde. DepartamentodeAc¸õesProgramáticasEstratégicas.IIPesquisa dePrevalênciadoAleitamentoMaternonascapitaisbrasileirase DistritoFederal.Brasília:EditoradoMinistériodaSaúde;2009.
16.Venancio SI, Saldiva SR, Escuder MM, Giugliani ER. The Baby-Friendly Hospital Initiative shows positive effects on breastfeedingindicatorsinBrazil.JEpidemiolCommunHealth. 2012;66:914---8.
17.WorldHealthOrganization.Indicatorsforassessinginfantand youngchildfeedingpractices.Part1:definitions.Conclusions ofaconsensusmeetingheld6---8November2007inWashington, DC,USA.Geneva:WorldHealthOrganization;2007.
18.IBGE.Pesquisanacionalporamostradedomicílios:PNAD,vol. 1.RiodeJaneiro:IBGE;2011.
19.Buccini GS, Perez-Escamilla R, Venancio SI. Pacifier use and exclusive breastfeeding in Brazil. J Hum Lact. 2016;32:NP52---60.
20.VenâncioSI,ReaMF,SaldivaSR.Alicenc¸a-maternidadeesua influênciasobreaamamentac¸ãoexclusiva.BIS,BolInstSaúde. 2010;12:287---92.
21.Vianna RP, Rea MF, Venancio SI, Escuder MM. A prática de amamentar entre mulheres que exercem trabalho remuner-adonaParaíba,Brasil:umestudotransversal.CadSaúdePúbl. 2007;23:2403---9.
22.MirkovicKR,PerrineCG,ScanlonKelleyS,Grummer-StrawnLM. Maternityleavedurationand full-time/part-timeworkstatus areassociatedwithusmothers’abilitytomeetbreastfeeding intentions.JHumLact.2014;30:416---9.
23.Martins EJ, Giugliani ER.Fatores associadosà amamentac¸ão prolongada.JPediatr(RioJ).2012;88:67---73.
24.TanakaS.ParentalleaveandchildhealthacrossOECDcountries. EconJ.2005;115:F7---28.
25.Heymann J,Earle A,McNeill K.Theimpact oflaborpolicies on thehealth ofyoung childrenin thecontext ofeconomic globalization.AnnuRevPublicHealth.2013;34:355---72.
26.World Health Organization. Infant and young child feeding:
modelchapter for textbooksfor medical studentsand allied
health professionals; 2009. Available from: http://apps.
who.int/iris/bitstream/10665/44117/1/9789241597494eng. pdf?ua=1
27.UnitedNations.Theworld’swomen:trendsandstatistics,New York;2010. Available from:unstats.un.org/unsd/publication/ SeriesK/SeriesK19e.pdf[cited10.12.15].
28.Rea MF, Venâncio SI, Batista LE, Santos RG, Greiner T. Possibilidades e limitac¸o˜es da amamentac¸a˜o entre mul-heres trabalhadoras formais. Rev Saúde Públ. 1997;31: 149---56.
29.Brasileiro AA, Ambrosano GM, Marba ST, Possobon RF. A amamentac¸ão entre filhos de mulheres trabalhadoras. São Paulo.RevSaúdePúbl.2012;46:642---8.