rev bras hematol hemoter. 2017;39(1):73–76
w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Case
report
Mantle
cell
lymphoma
presenting
as
multiple
lymphomatous
polyposis
of
the
gastrointestinal
tract
Cláudio
Martins
∗,
Cristina
Teixeira,
Élia
Gamito,
Ana
Paula
Oliveira
CentroHospitalardeSetúbal,Setúbal,Portugal
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received4October2016 Accepted7November2016 Availableonline31December2016
Introduction
Thegastrointestinal(GI)tractisthemostcommonextranodal siteaffectedbylymphoma,accountingfor5–20%ofallcases.1
Theincidenceandlocation ofprimaryGIlymphomavaries aroundtheworld.Overall,themostcommonlyinvolvedsites arethe stomachfollowedbythe smallbowel andileocecal region.2Concerninghistologicalsubtypes,mucosa-associated
lymphoidtissuelymphomaismorecommoninthestomach, mantlecelllymphoma(MCL)intheterminalileum,jejunum and colon, enteropathy-associated T-celllymphoma in the jejunum,andfollicular lymphomaintheduodenumwitha geographicvariationinitsdistribution.3MCLisarareand
dis-tinctsubtypeofB-cellneoplasm,comprisingapproximately 6–9%ofallmalignantlymphomainWesternEurope,withan incidenceof1–2cases/105people/year.4
EndoscopicfeaturesofGIlymphomasareheterogeneous, encompassingulcers,erosions,polypsandsoon.GIpolyposis
∗ Correspondingauthorat:DepartmentofGastroenterology,SetúbalHospitalCenter–SãoBernardoHospital,2910-446,Setúbal,Portugal.
Tel.:+351265549000.
E-mailaddress:[email protected](C.Martins).
occursinupto10%ofcases,includingconditionssuchas mul-tiplelymphomatouspolyposis(MLP)andimmunoproliferative small-intestinaldisease.MLPisarareentitycharacterizedby thepresenceofnumerousGIpolypoidlesionsinvolving sev-eraldigestive tractsegments.Typicallymphomapresenting withMLPisMCLalthoughothertumorscanhavethisfeature.5
MCLasMLPoccursmorecommonlyinolderadultsand hasamalepredominance.6Theetiopathogenesisisunknown
butasusceptiblegeneticbackground,aprevious chemothera-peuticregimenor ionizedradiationcould contributetothe developmentofMCL. Theclinical courseisheterogeneous. Themajorityofpatients(>90%)presentwithadvanceddisease (AnnArborstageIII–IV)whichcompriseslymphadenopathy, hepatosplenomegalyandbonemarrowinvolvement.
Diagnosiscanusuallybemadebasedonendoscopic find-ingsandhistopathologicalanalysisoftheirbiopsyspecimens. ImmunohistochemistrytodetectcyclinD1overexpressionis mandatory.IntherarecyclinD1-negativecases,detectionof Sox-11mayhelptoestablishthediagnosis.7
http://dx.doi.org/10.1016/j.bjhh.2016.11.005
74
revbrashematolhemoter.2017;39(1):73–76Figure1–Endoscopicfindings.(A)Smallpseudopolypoidlesionsontheduodenalbulb;(B–F)Multiplesessilepolypoid lesionsofdifferentsizesthroughoutthecolon;(F)Polypoidlesionwithulceratedsurface.
Systemicimmunochemotherapyisthetreatmentofchoice. ThemanagementofMCLischallengingbecause ithasthe worstfeaturesofbothhighandlowgradenon-Hodgkin lym-phoma(NHL)–anaggressiveclinicalcoursebutwithapattern ofresistantandrelapsingdiseaserenderingitincurablewith standardtherapy.
Herein, we report an uncommon case of MCL pre-sented with diffuse GI tract involvement, mesenteric lymphadenopathies,hepatosplenomegalyandbonemarrow infiltration,emphasizingitsendoscopicfeatures.
Case
report
A62-year-oldCaucasianfemale wasreferredtoour depart-mentdue toanemiaand apositivefecaloccultblood test. The patient presented with a two-month clinical picture of mild diffuse abdominal pain, change in bowel habits
including loose stools, significant involuntary weight loss, anorexiaandasthenia.Theremainingpatient’shistorywas uneventful. Shereportedno history ofsmoking, alcoholor drug consumptionand deniedany history ofsystemic dis-eases.Therewasanimportantfamilyhistoryofgastriccancer infirst-degreerelatives, namelythreebrothers withgastric adenocarcinoma diagnosedat30,50and 60 yearsold.The physicalexaminationshowedpallor,painless splenomegaly andapalpablemassintherightiliacfossa.Superficial lym-phadenopathieswereabsent.
Laboratorytestsshowedmicrocyticandhypochromic ane-mia(hemoglobin7.6g/dL,MCV78fL),normaltotalwhiteblood cell count(7.3×109/L), mildthrombocytopenia (125×109/L)
and high lactate dehydrogenase (399 U/L; normal range: 125–200).Theerythrocytesedimentationrate,C-reactive pro-tein,totalprotein,albumin,andliverandkidneytestswere normal. Laboratory study ofanemia revealed a multifacto-rialetiologywithferropenic(lowserumironlevel,ferritinand
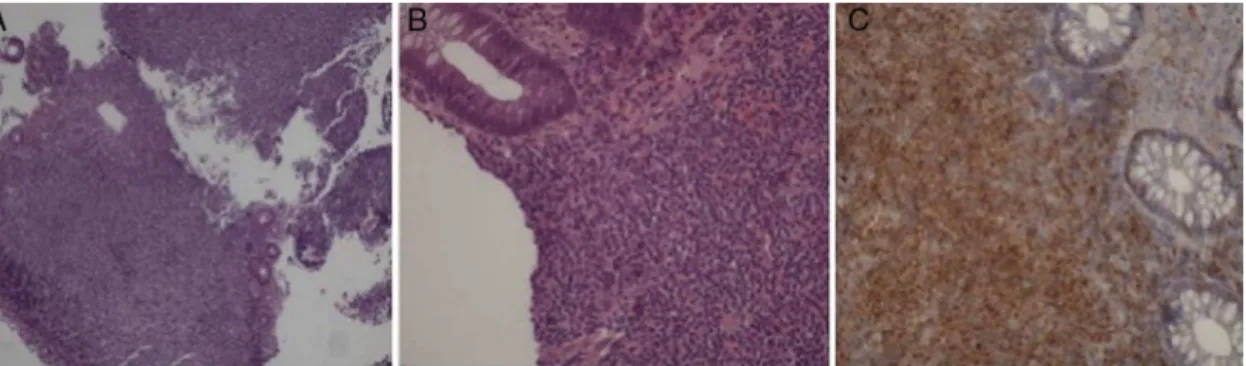
Figure2–Histopathologicalfeaturesofthelymphoma.(A,B)Diffuseintestinalmuralinfiltrationoftumorcells(A–
hematoxylin&eosinstain:magnification×40;B–hematoxylin&eosinstain:magnification×100);(C)Neoplasticcellswere
revbrashematolhemoter.2017;39(1):73–76
75
transferrinsaturation)andnon-autoimmunehemolytic com-ponents(reticulocytosis,polychromatophilia,elevatedlactate dehydrogenaseandunconjugatedbilirrubinandverylow hap-toglobin).
Upper endoscopyshowed small pseudopolypoidlesions ontheduodenalbulb(Figure1A).Totalcolonoscopyrevealed multiplesessilepolypoidlesions,rangingfrom4to25mmin thelargest dimension,somewithsubepithelialappearance andothers withsurfaceulceration, alongthe entirelength (Figure1B–F).
Endoscopicbiopsysamplesofduodenalandcoloniclesions showed diffuse infiltration of the intestinal wall by atypi-calsmall-to-medium sized lymphocytes (Figure 2A and B). Immunohistochemicalanalysisdemonstratedpositive stain-ingforCD20,CD5,Bcl-2andcyclinD1(Figure2C)andnegative forCD3andCD10;75%oftumorcellswerepositiveforKi-67. Therefore,thesefindingssupportedadiagnosisofmantlecell lymphomapresentingasmultiplelymphomatouspolyposis. Thesubsequentworkupincludedathoraco-abdominopelvic computed tomography (CT) scan that revealed thickening ofseveralsegments ofthe smallandlargeintestinalwalls, mostprominentintheterminalileum,multiplemesenteric adenopathiesandhomogeneoushepatosplenomegaly;there were no superficial and intrathoracic lymphadenopathies. Bonemarrowbiopsyshowedlymphomatousinvolvement.
ThebiologicMCLInternationalPrognosticIndex(IPI)score was7.8andthediseasewasclassifiedasstageIVBaccording totheAnnArborstagingsystem.
The patient underwent immunochemotherapy with rit-uximab, cyclophosphamide, doxorubicin, vincristine and prednisone(R-CHOP).Sofar,shecompletedeightcycleswith good tolerance. Mild oral mucositis was the main compli-cation reported during treatment. There was a significant improvementinherclinical statuswithprogressiveweight recovery.Follow-upupperandlowerendoscopicexaminations aftereightcyclesrevealedcompleteremissionwithabsence of all polypoid lesions in the GI tract. Likewise, thoraco-abdominopelvic CT scan showed no hepatosplenomegaly, remarkableregressionofherbowelwallthickening,and dis-appearanceofmostenlargedmesentericlymphnodes.
Discussion
MLP,firstdescribedbyCornesetal.8in1961,ischaracterizedby
thepresenceofdiffuseproliferationofatypicallymphocytes presentingasmultiplepolypoidlesionsindifferentGIsites.
B-cell GI lymphomas are more frequent than T-cell GI lymphomaswith this being due to the fact that, histolog-ically, these polypsoriginate from the mantlezone ofthe lymphoidfollicleofthe mucosa-associatedlymphoid tissue (MALT).Therefore,typicallymphomapresentingwithMLPis MCL,whichhasbeenreportedwithafrequencyofupto9%of allGIB-celllymphomas.However,othertumorscanhavethis featureand,additionally,multiplehistologicaltypesof lym-phomascanbesimultaneouslypresentinacontextofMLP. Therefore,thebiopsyofmorethanonepolypandofdifferent typesoflesionsisalwaysadvisable.
MajorsitesofGIMCLinvolvementaretheileocecalregion (35.7%),ileum(20.3%),rectum (9.1%)and duodenum(7.7%).
Regionallymphnodeinvolvementisnotuncommon.Other possible extra-digestive tract sites include bone marrow, peripherallymphnodes,Waldeyer’sring,spleenandliver.
MCLusuallyoccursinthemalepopulation(65%)witha meanageof63years.Arecentlypublishedpopulation-based study revealed that 91% of MCL cases found were ethni-callywhite,4%wereblackandalmost4%wereAsian/Pacific Islander.9Theseethnicdifferencesmaybearesultofgenetic
orotherenvironmentalandlifestylefactors.
TheclinicalpictureofGIMCLisheterogeneous.Basedon thelargeststudyseriesbyRuskone-Fourmestrauxetal.10,the
mainpresentingsymptoms ofGIMCL areabdominalpain, diarrhea and hematochezia.Weight loss,night sweats and fatigue are commonly found. The differential diagnosis of GI MCL include adenomatous polyps, hereditary polyposis syndromes, colorectal carcinoma,GIlipomatosis, lymphoid nodular hyperplasia with hypogammaglobulinemia,among others.
Diagnosiscanbemadebasedonendoscopicfindingsand histopathological analysis. The typicalendoscopic features aresmallnodularorpolypoidlesionsrangingfromtwo mil-limeterstoseveralcentimetersindiameter,alongtheentire GItract,withorwithoutnormalinterveningmucosa.
StagingiscarriedoutaccordingtotheAnnArbor classi-ficationsystem.Forprognosticpurposes,aMCLIPIhasbeen established.11TheevaluationoftheKi-67proliferativeantigen
isthemostapplicablemethodtoevaluatecellproliferation, andisconsideredthemostestablishedbiologicalriskfactor inMCL.
Thecurrenttherapeuticapproachisbasedonclinicalrisk factors,symptoms,patientcharacteristics andstageof dis-ease.Inadvanceddisease,themajorclinicaltrialsofthelast decadefocusedonimprovementofthefront-linetreatmentof MCL,leadingtothedefinitionofa‘goldstandard’therapyfor youngandfitpatients(<66yearsandtransplanteligible) con-sistingofadose-intensifiedimmunochemotherapy,followed byautologousstem-celltransplantation(ASCT).12,13Basedon
severalstudies,particularlytherecentEuropeanMCLNetwork YoungerPhaseIIItrial,aR-CHOPinductionregimenandhigh doseofcytarabinefollowedbyhighdoseconsolidationand ASCTisrecommended.14Forthegroupofelderlypatientsnot
eligibleforASCT,conventionalimmunochemotherapy(e.g. R-CHOP)followedbymaintenancewithrituximab,appearstobe the‘goldstandard’.
Inthisreport,wedescribeanuncommoncaseofMCL pre-sentingasMLPinvolvingtheentireintestinewithremarkable endoscopicfindings.Inourcase,thepatientpresentedwith disseminateddiseasewithinvolvementofmesentericlymph nodes,bonemarrow,liverandspleen.Duetothisfact,itis dif-ficulttospeculatewheretheprimarylocationofthedisease was.TheMCLIPIscorewas7.8(highrisk)andthediseasewas classifiedasstageIVBaccordingtotheAnnArborstaging sys-tem.TheprognosisofMCLpatientsatthisstageisverypoor withanoverallsurvivalof37months,andfewerthan8%of patientsarealiveat10years.
76
revbrashematolhemoter.2017;39(1):73–76furtherstudiesintegratingnovelagentsare stillrequiredto determinetheoptimaltreatmentwithlesstoxicity.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. FreemanC,BergJW,CutlerSJ.Occurrenceandprognosisof extranodallymphomas.Cancer.1972;29(1):252–60.
2. HerrmannR,PanahonAM,BarcosMP,WalshD,StutzmanL. Gastrointestinalinvolvementinnon-Hodgkin’slymphoma. Cancer.1980;46(1):215–22.
3. RizviMA,EvensAM,TallmanMS,NelsonBP,RosenST.T-cell non-Hodgkinlymphoma.Blood.2006;107(4):1255–64.
4. DreylingM,GeislerC,HermineO,Kluin-NelemansHC,Le GouillS,RuleS,etal.Newlydiagnosedandrelapsedmantle celllymphoma:ESMOClinicalPracticeGuidelinesfor diagnosis,treatmentandfollow-up.AnnOncol.2014;25 Suppl.3:iii83–92.
5. BurkeJS.Lymphoproliferativedisordersofthe gastrointestinaltract:areviewandpragmaticguideto diagnosis.ArchPatholLabMed.2011;135(10):1283–97.
6. Remes-TrocheJM,De-AndaJ,OchoaV,Barreto-Zu ˜nigaR, Arista-NasrJ,ValdovinosMA,etal.Ararecaseofmultiple lymphomatouspolyposiswithwidespreadinvolvementofthe gastrointestinaltract.ArchPatholLabMed.2003;127:1028–30.
7. FuK,WeisenburgerDD,GreinerTC,DaveS,WrightG, RosenwaldA,etal.CyclinD1-negativemantlecell lymphoma:aclinicopathologicstudybasedongene expressionprofiling.Blood.2005;106(13):4315–21.
8.CornesJS.Multiplelymphomatouspolyposisofthe gastrointestinaltract.Cancer.1961;14:249–57.
9.AmbinderAJ,ShenoyPJ,NastoupilLJ,FlowersCR.Using primarysiteasapredictorofsurvivalinmantlecell lymphoma.Cancer.2013;119(8):1570–7.
10.Ruskoné-FourmestrauxA,AudouinJ.Primarygastrointestinal tractmantlecelllymphomaasmultiplelymphomatous polyposis.BestPractResClinGastroenterol.2010;24(1):35–42.
11.HosterE,DreylingM,KlapperW,GisselbrechtC,vanHoofA, Kluin-NelemansHC,etal.Anewprognosticindex(MIPI)for patientswithadvanced-stagemantlecelllymphoma.Blood. 2008;111(2):558–65.
12.DreylingM,LenzG,HosterE,VanHoofA,GisselbrechtC, SchmitsR,etal.Earlyconsolidationbymyeloablative radiochemotherapyfollowedbyautologousstemcell transplantationinfirstremissionsignificantlyprolongs progression-freesurvivalinmantle-celllymphoma:resultsof aprospectiverandomizedtrialoftheEuropeanMCLNetwork. Blood.2005;105(7):2677–84.
13.HosterE,MetznerB,ForstpointnerR,PfreundschuhM, TrümperL,HallekM,etal.Autologousstemcell
transplantationandadditionofrituximabindependently prolongresponsedurationinadvancedstagemantlecell lymphoma.(ASHAnnualMeetingAbstracts)Blood. 2009;114(22):880.