w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Original
article
Secondary
myeloid
neoplasms:
bone
marrow
cytogenetic
and
histological
features
may
be
relevant
to
prognosis
Roberta
Sandra
da
Silva
Tanizawa
a,∗,
Maria
Claudia
Nogueira
Zerbini
b,
Ricardo
Rosenfeld
c,
Cristina
Aiko
Kumeda
a,
Raymundo
Soares
Azevedo
b,
Sheila
Aparecida
Coelho
Siqueira
a,
Elvira
Deolinda
Rodrigues
Pereira
Velloso
aaUniversidadedeSãoPaulo,FaculdadedeMedicina,HospitaldasClínicas,SãoPaulo,SP,Brazil
bUniversidadedeSãoPaulo,FaculdadedeMedicina,SãoPaulo,SP,Brazil
cUniversidadeFederaldeSãoPaulo(UNIFESP),HospitalSãoPaulo,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received22July2015 Accepted21September2016 Availableonline22December2016
Keywords:
Myelodysplasticsyndromes Secondmalignancy Secondneoplasm Secondaryeffect
Therapy-associatedneoplasm;
a
b
s
t
r
a
c
t
Background:Secondary myeloid neoplasms comprise a group of diseases arising after chemotherapy,radiation,immunosuppressivetherapyorfromaplasticanemia.Fewstudies haveaddressedprognosticfactorsintheseneoplasms.
Method:Forty-twopatientsdiagnosedfrom1987to2008withsecondarymyeloidneoplasms wereretrospectivelyevaluatedconcerningclinical,biochemical,peripheralblood,bone mar-rowaspirate,biopsy,andimmunohistochemistryandcytogeneticfeaturesatdiagnosisas prognosticfactors.TheInternationalPrognostic ScoringSystem wasapplied.Statistical analysisemployedtheKaplan–Meiermethod,log-rankandFisher’sexacttest.
Results:Twenty-threepatients(54.8%)weremaleandthemedianagewas53.5years(range: 4–88years)atdiagnosisofsecondarymyeloidneoplasms.Previousdiseasesincluded hema-tologicmalignancies,solidtumors,aplasticanemia,autoimmunediseasesandconditions requiringsolid organ transplantations. One third of patients (33%) were submitted to chemotherapyalone,2%toradiotherapy,26%tobothmodalitiesand28%to immunosup-pressiveagents.Fivepatients(11.9%)hadundergoneautologoushematopoieticstemcell transplantation.Themedianlatencybetweentheprimarydiseaseandsecondarymyeloid neoplasmswas85months(range:23–221months).Eightpatientsweresubmittedto allo-geneichematopoieticstem celltransplantationto treat secondarymyeloid neoplasms. Importantchangesinbonemarrowweredetectedmainlybybiopsy,immunohistochemistry andcytogenetics.ThepresenceofclustersofCD117+cellsandp53+cellswereassociated
withlowsurvival.p53wasassociatedtoahigherriskaccordingtotheInternational Prognos-ticScoringSystem.Highprevalenceofclonalabnormalities(84.3%)andthrombocytopenia (78.6%)wereindependentfactorsforpoorsurvival.
∗ Correspondingauthorat:CytogeneticsLaboratory,HematologyService,HospitaldasClínicas,FaculdadedeMedicina,Universidadede
SãoPaulo,AvDr.EnéasdeCarvalhoAguiar,155,1◦andar,05403-000SãoPaulo,SP,Brazil.
E-mailaddress:[email protected](R.S.Tanizawa).
http://dx.doi.org/10.1016/j.bjhh.2016.09.015
Conclusion: Thisstudydemonstratedthatcytogenetics,bonemarrowbiopsyand immuno-histochemistryareveryimportantprognostictoolsinsecondarymyeloidneoplasms.
©2016Associac¸ ˜aoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.Published byElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Secondary myeloid neoplasms(s-MN) comprise a group of diseases arising as late complications after chemotherapy and radiation and are associated with risk factors such as congenital disorders and acquired bone marrow (BM) failure.1–4
Themoststudiedoftheses-MNarerelatedto chemother-apyandradiotherapy.Therateofthesediseasesisincreasing as the survival of patients with cancer improves. Patients submittedtoautologoushematopoieticstemcell transplan-tation (HSCT)with intensive chemotherapyand total body irradiation (TBI), a type of complimentary therapy, have demonstrated apotential ofdevelopingsecondary myeloid disorders.5The2008WorldHealthOrganization(WHO)
classi-ficationadoptedthetermtherapy-relatedmyeloidneoplasms (t-MN)forcases ofmyeloid malignancies after chemother-apy/radiotherapy (CH/RT) that fulfill morphological criteria includingmyelodysplasticsyndromes (MDS),acutemyeloid leukemia (AML) and myeloproliferative neoplasms (MPN). Alkylating drugs/radiation and topoisomerase II inhibitor agentsareimplicatedinthesedisorders.Thecharacteristics oft-MNinthemajorityofcasesincludeanemiawith macro-cytosis,dysplasticchangesinneutrophilsandbasophilia.BM fibrosis,threelineagedysplasia,ringsideroblastsand abnor-malkaryotypesareseeninthemajorityofcases,withalmost 50%ofcaseshavingless than5%ofBMblasts. Theclinical courseistypicallyprogressiveandresistanttoconventional therapies.6
Long-survivingpatientstreatedwithimmunosuppressive therapy,suchasaplasticanemia(AA),autoimmunedisease and recipientsof solidorgan grafts have anincreasedrisk ofdevelopings-MN.7–9 Furthermore,theconcomitantuseof
immunosuppressiveagentswithhematopoieticgrowth fac-torshasbeenassociatedwiths-MDS.10Todate,littleisknown
about s-MNafter usingimmunosuppressivetherapy. There are few datain the literatureconcerningmorphologic and outcomestudies.However,cytogeneticabnormalitiesarean importantmarkerinthissubgroup withanomaliesusually involvingchromosomes6and8andinparticularmonosomy 7.11
Genetic diseases such as Fanconi anemia, dyskeratosis congenita,Diamond-Blackfananemia,Shwachman-Diamond syndromeandsomeformsofseverecongenitalneutropenia have an increased propensity for myeloid neoplasms.12
Furthermore, studies about host factors such as com-mon polymorphisms in drug metabolizing enzymes and biological markers of drug- and radiation-induced genetic damage may be useful in identifying patients at risk of therapy-related complications and secondary malignancies.13,14
Data concerning overall survival (OS) and prognosis of patientswiths-MNremainpoor.AllogeneicHSCTseemstobe theonlycurativetherapyforallsubgroupsincludedins-MN.15
Cytogeneticstatusplaysanimportantroleindetermining theoutcomeofthesepatients.Outcomeforprimarydisease, platelet count,hemoglobinlevel,age, totalproteinlevel, C-reactive proteinlevelandunfavorable karyotype havebeen describedasprognosticfactorsinsomestudies.16–18 Despite
the importance ofBM studies inpathological processesof secondary disease,fewinvestigations havebeenconducted concerning BM biopsies and immunohistochemistry. Orazi etal.19analyzed14patientswithpreviousdiseasesincluding
Hodgkin’slymphoma,Non-Hodgkinlymphoma, breast can-cer,plasmacellmyelomaandskincarcinomathatevolvedto therapy-relatedMDS.DatafromBMbiopsies,suchas abnor-mallocalizationofimmatureprecursors,marrowfibrosis,and overexpressionofCD34+cellshavebeenassociatedwithpoor
prognosis.Inaddition,p53proteinoverexpressioncanbe fre-quentlyobserved,particularlyincasesassociatedwithsevere ineffectivehematopoiesis.20
Objective
Theaimofthisstudy wastoanalyze clinical,biochemical, morphological(peripheralblood,BMaspirateandbiopsy)and cytogenetic characteristicsasprognosticfactors inpatients withs-MNdiagnosedandtreatedatasinglecenter.
Methods
Of428patientswithMDSinthedatabaseofHC-FMUSP,a pub-lichospitalinSãoPaulo,Brazil,42patients(10%)withs-MN aftertheuseofchemotherapy,radiotherapy(for hematolog-icalorsolidtumors)orimmunosuppressivetherapy(forAA, solidtransplantationandautoimmunediseases)from1987to 2008wereretrospectivelystudied.Thisstudywasconducted inaccordancewiththeDeclarationofHelsinkiandapproved by the Ethics Committeeof the institution. Medicalcharts wereevaluatedforclinicalcharacteristicsandlaboratorydata at diagnosis (Tables 1 and 2). BMaspirates were reviewed according tomorphologicalcriteria ofthe WHO 2008 crite-ria.BMbiopsieswere reviewedforcellularity,anestimated blastpercentage,fibrosisanddyspoiesis. Immunohistochem-istry was carried out for myeloperoxidase, Glycophorin A, CD61,FVIII,CD20,CD3,CD138,CD34,CD117andp53protein expressions.Thelatterwasdefinedas0to3+andconsidered positiveifanyexpressionwasdetected(Table2).Cytogenetics wasperformedatdiagnosisusingstandardG-banding21and
Table1–Univariateanalysisforprognosticfactorsonoverallsurvivalofpatientswithsecondarymyeloidneoplasms– clinicaldata.
Numberofcases Mediansurvival(months) p-Value
OverallsurvivalcensoringallogeneicHSCT 42 5.7
OverallsurvivalnotcensoringallogeneicHSCT 42 6
Gender(n=42)
Male 23 5.9 0.974
Female 19 5.1
Age(n=42)
<50years 18 8.7 0.135
≥50years(range4–88) 24 3.6
Primarydisease(n=42)
Hematologicmalignancies 19 3.5 0.018
Solidtumors 6 3.6 0.833
Aplasticanemia 11 20.7 0.041
Autoimmunedisordersandsolidorgantransplantations 6 12.2 0.651
Medianlatency(n=41)
<85months(range23–221) 20 3.6 0.264
≥85months 21 9.2
AllogeneicHSCT(n=42)
No 34 5.7 0.007
Yes 8 40
Previoustherapy(n=39)
CH 14 5.9 0.879
RT 1 3.6 0.599
CH+RT 11 2.5 0.749
AutologousHSCT 5 5.9 0.309
IST 12 7.1 0.764
CH:chemotherapy;HSCT:hematopoieticstem-celltransplantation;IST:immunosuppressivetherapy;RT:radiotherapy.
ScoringSystem(IPSS)forprimaryMDS23wascalculated.The
IPSShasalreadybeenvalidatedfortherapy-inducedMDS.24
Thedatawereanalyzedusingversion16.0oftheStatistical PackagefortheSocialSciences(SPSS)computerprogram. Sta-tisticalanalysisforOSusedtheKaplan–Meierproductlimit method,censoringthetimeofallogeneicHSCT,andlog-rank testforcomparingtheOSbetweensubgroups.Thesignificant variables inunivariateanalysis(except forhistological fac-torsandbiochemistrydatabecauseofthesmallnumberof samples)weresubmittedtothebinarylogisticregressiontest. Fisher’sexacttestwasusedforassociationsbetween categor-icalvariables suchasp53andabnormalcytogenetics,blast cellsandCD34+andCD117+cells.
Results
Twenty-threepatients(54.8%)weremale,withamedianageof 53.5years(range:4–88years)atthediagnosisofs-MN. Hema-tologicmalignancies,solidtumors,AA,autoimmunediseases and recipients ofsolid organ transplantations were identi-fiedaspreviousconditionsrelatedtothedisease.Forprevious therapy,33%ofpatientshadbeensubmittedtochemotherapy alone,2%toradiotherapy,26%tobothmodalitiesand28%to immunosuppressiveagents.Fivepatients(11.9%)had under-goneautologousHSCT.Thepatientcharacteristicsareshown inTable1andfurtherinformationaboutclinicaldataare avail-ableinapreviouspublication.22Themedianlatencybetween
theprimarydiseaseands-MNwas85months(range:23–221 months).EightpatientsunderwentallogeneicHSCTtotreat s-MN(Table1).
Peripheralbloodanalysiswasperformedinallcasesand showedanemia,neutropeniaandthrombocytopeniainmore than60%ofthecases;morethan25%presentedblastcells. Serumlactatedehydrogenasewasincreasedin41%,ferritin >1000ng/mL in50% and albumin <3.2g/dL in22.7% of the availablecases(Table2).
BM aspirates were available in 37 cases, with 38% of patients presentingblasts under 5%, 43% of patients with blasts between 5–19% and 19% of the cases with 20% of blasts or more. Two patients presented characteristics of MDS/myeloproliferativesyndrome,onechronic myelomono-cytic leukemia and one with thrombocytosis. Increases in eosinophil,basophilandplasmacellcountsweredetectedin fewcases,and>15%ofringsideroblastsinonly14.3%(Table2). Twenty-two BMbiopsiesanalyzedwithamedianlength of 1.4cm (range: 0.6–3.7cm) revealed global hypocellularity in9.1%.Hypobulatedmegakaryocyticwasthemostrelevant findingconcerningdysplasia;increasedfibrosiswasdetected in 62%, abnormal localization of immature precursors in 23.8%,lymphoid nodulesin40.9%,CD34+ and CD117+ cells
weredetectedinmorethan75%ofthecasesandelevatedp53 proteinexpressionin33.3%.CD117,butnotCD34,wasoften positiveinthecytoplasmofmegakaryocytes(Table2).
Table2–Univariateanalysisforprognosticfactorsonoverallsurvivalofpatientswithsecondarymyeloidneoplasms– laboratorydata.
Numberofcases Mediansurvival(months) p-Value
Peripheralblood(PB)
Hemoglobin(g/dL)–n=42
≥10.0 15 5.6 0.29
<10.0(mean:9,range5.8–14.7) 27 5.9
Neutrophils×109/L–n=42
≥1.8 15 5.1 0.615
<1.8(mean:1.2,range0.2–10.8) 27 5.9
Platelets×109/L–n=42
≥100 9 12.2 0.084
<100(mean:43,range7–368) 33 5.1
BlastsinPB–n=42
Absent 31 5.9 0.295
Present 11 2.4
Biochemical
LDH(U/L)–n=24
≤480 14 9.2 0.002
>480(mean:414,range271–4310) 10 1.7
Albumin(g/dL)–n=22
≥3.2 17 5 0.624
<3.2(mean:3.6,range2.1–4.5) 5 6.3
Ferritin(ng/mL)–n=16
≤1000 8 6.3 0.037
>1000(mean:822,range45–7842) 8 1.7
Bonemarrowaspirate
Globalcellularity–n=37
Hipocellularity 11 5.9 0.853
Normal 11 7.1
Hipercellularity 15 3.6
CellularityMGKserie–n=36
Hipocellularity 19 5.6 0.79
Normal 9 5.1
Hipercellularity 8 7.1
DysplasiaMGKserie–n=22
No 7 12.9 0.233
Yes 15 5.1
Pseudo-Pelger-Huëtanomaly–n=35
No 25 6.3 0.586
Yes 10 3.6
(%)BMBlasts–n=37
<5 14 5.1 0.825
≥5 23 5.6
Eosinophils(%)–n=37
≤5 34 5.9 0.243
>5 3 3.5
Basophils(%)–n=37
≤1 35 5.9 0.495
>1 2 3.5
Plasmacells(%)–n=37
≤5 35 5.9 0.139
>5 2 2
Bonemarrowbiopsy
Globalcellularity–n=22
Hipocellularity 2 12.7 0.948
Normal 7 5
Hipercellularity 13 9.2
CellularityMGKserie–n=22
Hipocellularity 7 1.7 0.977
Normal 6 7.1
Hipercellularity 9 9.2
Dysplasia
No 2 1.7 0.608
MGKserie–n=17
Table2–(Continued)
Numberofcases Mediansurvival(months) p-Value
Architecturalchanges
No 4 19 0.464
MGKserie–n=17
Yes 13 9.2
ALIP–n=19
No 14 7.1 0.31
Yes 5 20.7
CD34+cells–n=22
≤1% 5 Notreached 0.181
>1% 17 7.1
CD34+cells–n=17
(1–10%) 12 8.7 0.676
>10% 5 7.1
CD34+cluster–n=22
No 9 9.2 0.755
Yes 13 7.1
CD117+cells–n=17
≤1% 3 19 0.172
>1% 14 9.2
CD117+cells–n=14
(1–10%) 9 12.3 0.081
>10% 5 1.7
CD117+cluster–n=17
No 12 12.7 0.029
Yes 5 1.7
p53proteinexpression–n=21
No 14 12.7 0.056
Yes 7 3.5
Lymphoidnodules–n=22
No 13 12.2 0.81
Yes 9 9.2
Fibrosis–n=21
<Grade2 8 7.1 0.608
≥Grade2 13 9.2
Cytogenetics
Karyotype
Normalvsabnormal–n=32
Normal 5 Notreached 0.030
Abnormal 27 5
Complexvsothers–n=27
Complex 12 3.5 0.057
Others 15 8.7
Monosomy7vscomplex–n=22
Monosomy7 10 5 0.123
Complex 12 3.5
IPSSrisk–n=31
Low+intermediateI 6 12.2 0.038
IntermediateII+high 25 5
ALIP:abnormallocalizationimmatureprecursor;LDH:lactate-dehydrogenase;MGK:megakaryocytic.
In univariate analysis, hematologic malignancies, low plateletcount,highserumlactatedehydrogenaseandferritin levels,detectionofCD117clusters,p53+,abnormal
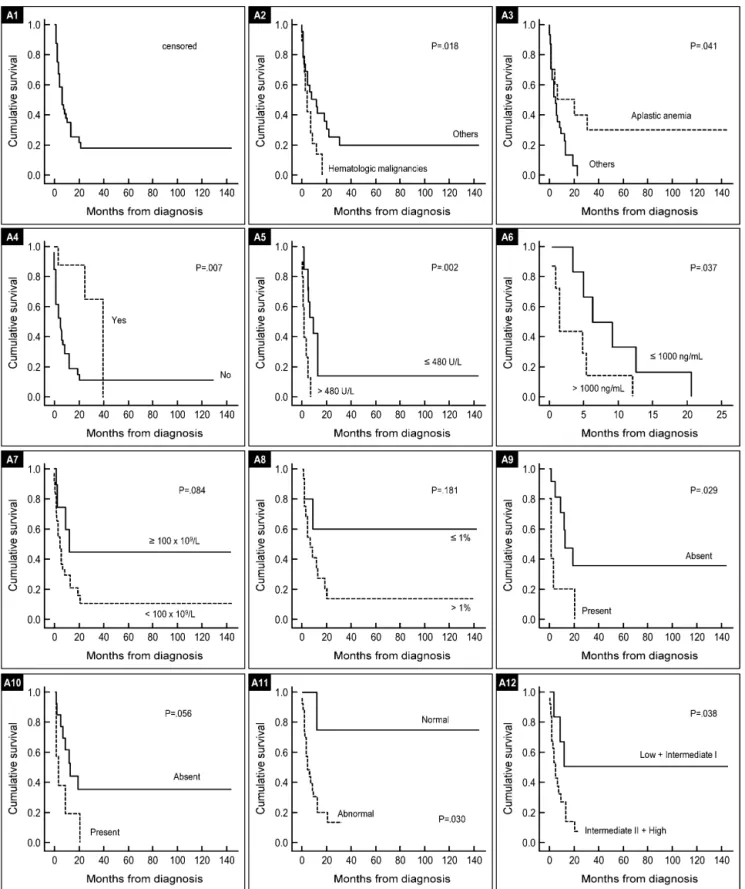
cytogene-tics,Intermediate-IIandhighriskIPSSgroupswerefoundtobe associatedwithpoorsurvival.NoparameterstudiedfromBM aspiratehadimpactonsurvival(Table2).Hematologic malig-nanciesasapreviousdisease,lowplateletcount,abnormal karyotype(Table2)andpatientswhohadnotundergone allo-geneicHSCTwereindependentfactorsthatpredictedpoorer survivalinthissample.Figure1showsOScurvesaccordingto themostrelevantprognosticfindingsins-MN.
Thebinarylogisticregressiontest,appliedto32patients with complete clinical, peripheral blood, BM aspirate and cytogeneticparameters,showedthatclonalabnormalities(p -value=0.012)andplateletcounts<100× 109/L(p-value=0.028) wereindependentfactorsforpoorsurvival.Fisher’sexacttest showednocorrelationsbetweenp53andabnormal cytogen-etics (p-value=0.092),p53 and CD34+ cells (p-value=0.554),
p53andCD117+ cells(p-value=0.176);blastcellsandCD34+
cells (p-value=0.674), blast cell and CD34+ cell clusters (p
-value=0.583),blastcellsandCD117+cells(p-value=0.604),and
Figure1–Kaplan–MeiersurvivalcurvesforsecondaryMNpatientsbysignificantpoorprognosticfactors.
Discussion
Nowadays the number of s-MN has become increasingly important.Thisincreaseismainlyrelatedtoanexpandeduse ofhigh-dosechemotherapy/radiotherapy.Theriskof develop-ings-MNafterimmunosuppressivetherapyseemsimportant aswellsinceseveralcaseshavebeenreportedsofarinthe literature.7–11 Thisisaretrospectivestudywithasmalland
heterogeneoussample;itreflectsconsecutivecasesofs-MN overaperiodof21 yearsdiagnosedandtreatedinasingle center.
Thisstudyincludedpatientssubmittedtodifferent previ-oustherapies(CH/RTandimmunosuppressivetherapy);the findingsofthisstudyareconsistentwiththeclinicalpicture seeninpatients witht-MN.Thefrequencyofs-MN inthis studywas10%ofcasesintheMDSdatabase,withamedianage of53years.Themostcommonpreviousdiseasewasplasma cellmyelomatreatedwithmelphalan(21.4%),andtherewere three patients with follicular lymphoma treated with flu-darabineassociatedwithcyclophosphamide,reinforcingthe theorythatthisassociationincreasestheriskofdeveloping t-MNassuggestedinapreviousstudy.25Breastcancerwasthe
mostfrequentsolidtumor(50%–4/8) consistentwith pub-lisheddatathathasreportedanincreasedrateofs-MNinthis groupofsurvivorsprobablyasaconsequenceofaneffective therapy.26,27
The median OS for all patients was six months, basi-callythesameobservedinotherseriesofpatientswitht-MN that reportedfour and eightmonths.15,28 There was a
sig-nificantdifferencebetweenpatientswhoweresubmittedto allogeneic HSCT(40 months) and those who were not(5.7 months)(p-value=0.007).Thisisinagreementwithpublished dataandshowedthecrucialimportanceofthismodalityof therapy.
ThefindingsofthisstudysuggestthatBMaspiratesprovide limitedresults,probablyduetoaspiratedilution,anddidnot contributetotheprognosisofthesepatients.Thepercentage ofblastsinBMaspiratewasnotsignificantlyassociatedwith survival.Thisresultmightbeexplainedbythepoorquality ofthesamplematerialandthepercentageofblastsmaybe underestimated,sincethevaluewasnotrepresentativeinone thirdofcases.
IndividualswithpreviousAAseemtobeadifferentsubset ofpatients,showingpeculiarcharacteristicsasinthis sam-plealongermedianperiodoflatencyandhigherprevalence ofmonosomy7wereseen.Aninterestingdiscussionpoint iswhetherthesepatientshad thiscytogenetic abnormality beforetreatmentornot.
Theimportanceofintegrateddataanalysiswas demon-strated inthis study withfive patients, whose evaluations ofBMaspirateswerenotavailable.Ofthese,twohad com-plex karyotypes. The remaining three patients presented remarkabledysplasiainatleastgranulocyteand megakary-ocyte lineages, fibrosis (Grade 2–3) and CD34+ or CD117+
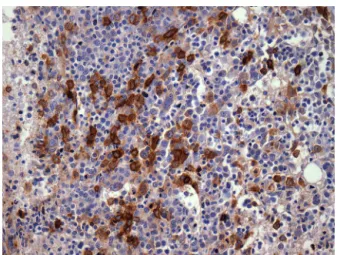
cells(1–10%)revealedinBMbiopsiesand immunohistochem-istry.TheimportanceofBMimmunohistochemistryshould bestressedinrespecttothep53proteinexpression(Figure2) andCD117/CD34blastevaluationstoidentifythepresenceof aggregatesofpositivecells(Figures3and4).
Figure2–Bonemarrowbiopsyofpatientwithsecondary myeloidneoplasmshowingp53+(immunohistochemical stains-400×),previousdisease:breasttumor.
BMbiopsiesshowedhypobulated megakaryocytesasthe mostrelevantfindingconcerningdysplasia(Figure5).CD117+
clusters andp53expressionhadan impactonthesurvival ofpatientswithmediansurvivalofonly1.7and3.5months, respectively.OScurvesforpatientswithCD34+versusCD34−
cells,didnotreachstatisticalsignificance,probablybecauseof thesmallnumberofpatients.Thecorrelationbetweenp53+
and abnormalcytogenetics didnotreach statistical signifi-canceprobablyduetosmallnumberofcases.Alterationsof p53+havebeenfoundinassociationwithaggressivedisease,18
andlargerseriesofcasesarenecessarytoconfirmour obser-vation of CD117 clusters as a prognostic marker for this condition.
Theimportanceofcytogeneticanalysisindiagnosis and prognosis of myeloid neoplasms is well documented. The results of this study are consistent with the literature29,30
andshowedthatnormalcytogeneticswasassociatedto bet-ter survival(p-value=0.03)andabnormalkaryotypewasan independentriskfactorforpoorsurvival(p-value=0.012).
Figure3–Bonemarrowbiopsyofpatientwithsecondary myeloidneoplasmshowingclusterCD34+cells
(immunohistochemicalstains-400×),previousdisease:
Figure4–Bonemarrowbiopsyofpatientwithsecondary myeloidneoplasmshowingclusterCD117+cells
(immunohistochemicalstains-400×),previousdisease:
severeaplasticanemia.
Figure5–Bonemarrowbiopsyofpatientwithsecondary myeloidneoplasmshowingdysplasiaandarchitectural changesinMGKserie(Hematoxylinandeosinstain -200×),previousrenaltransplant.
In addition, independent factors in multivariate analy-sisforpoor survivalincluded thrombocytopenia, abnormal karyotype and absence of allogeneic HSCT as therapy. Hypoproteinemia was not a poor prognostic factor in this investigation,asshowninapreviousJapanesestudy.18
Conclusion
Insummary, factors associatedinunivariate analysis with poorsurvivalincludedpreviousoncohematologicaldiseases, thrombocytopenia, elevatedlactatedehydrogenaseand fer-ritinlevels,CD117+ clusters,p53+,abnormalkaryotype,IPSS
risk(intermediateIIandhighsubgroups)andtheabsenceof allogeneicHSCTastherapy.DespitethefactthatIPSSwasnot designedforsecondaryMDS,itseemstobeusefulinthis sit-uation,mainlyinrespecttothrombocytopeniaandabnormal karyotypes,parameterswithhighprevalenceinMDS(79%and 84%ofpatientsrespectivelyinthisstudy).
Preventionofthislatecomplicationofprimarytreatment programsmustbecontinuouslyre-evaluated.Furtherstudies withalargernumberofcasesofs-MNshouldbeconducted toimprovetheunderstandingofthepathophysiologic mech-anismsofthediseaseandthedeterminationofbiomarkers, inordertodiagnoseandtreatthisaggressivedisease.
Conflict
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.FianchiL,PaganoL,PiciocchiA,CandoniA,GaidanoG,Breccia M,etal.Characteristicsandoutcomeoftherapy-related myeloidneoplasms:reportfromtheItaliannetworkon secondaryleukemias.AmJHematol.2015;90(5):E80–5.
2.Luna-FinemanS,ShannonKM,LangeBJ.Childhood monosomy7:epidemiology,biology,andmechanistic implications.Blood.1995;85(8):1985–99.
3.ImashukuS,HibiS,BesshoF,TsuchidaM,NakarataT, MyiazakiS,etal.Detectionofmyelodysplastic
syndrome/acutemyeloidleukemiaevolvingfromaplastic anemiainchildrentreatedwithrecombinanthumanG-CSF. Haematologica.2003;88(11):136–41.
4.ChurpekJE,LarsonRA.Theevolvingchallengeof therapy-relatedmyeloidneoplasms.BestPractResClin Hematol.2013;26(4):309–17.
5.LenzG,DreylingM,SchiegnitzE,HaferlachT,HasfordJ, UnterhaltM,etal.Moderateincreaseofsecondary hematologicmalignanciesaftermyeloablative
radiochemotherapyandautologousstem-celltransplantation inpatientswithindolentlymphoma:resultsofaprospective randomizedtrialoftheGermanLowGradeLymphomaStudy group.JClinOncol.2004;22(24):4926–33.
6.VardimanJW,ArberDA,BrunningRD,LarsonRA,MatutesE, BaumannI,etal.Therapy-relatedmyeloidneoplasms.In: SwerdlowSH,CampoE,HarrisNL,etal,editors.WHO classificationoftumoursofhaematopoieticandlymphoid tissues.Lyon:IARC;2008.p.127–9.
7.McCarthyCJ,SheldonS,RossCW,McCuneWJ.Cytogenetics abnormalitiesandtherapyrelatedmyelodysplastic syndromesinrheumaticdisease.ArthritisRheum. 1998;41(8):1493–6.
8.HuebnerG,KarthausM,PethigK,FreundM,GanserA. Myelodysplasticsyndromeandacutemyelogenousleukemia secondarytohearttransplantation.Transplantation. 2000;70(4):688–90.
9.Abu-ShakraM,BuskilaD,EhrenfeldM,ConradK,ShoenfeldY. Cancerandautoimmunity:immuneandrheumaticfeatures inpatientswithmalignancies.AnnRheumDis.
2001;60(5):433–41.
10.GurionR,Gafter-GvilliA,PaulM,VidalL,Ben-BassatI, YeshurunM,etal.Hematopoieticgrowthfactorsinaplastic anemiapatientstreatedwithimmunosuppressive
therapy-systematicreviewandmeta-analysis.Hematologica. 2009;94(5):712–9.
11.MaciejewskiJP,SelleriC.Evolutionofclonalcytogenetic abnormalitiesinaplasticanemia.LeukemiaLymphoma. 2004;45(3):433–40.
12.ParikhS,BesslerM.Recentinsightsintoinheritedbone marrowfailuresyndromes.CurrOpinPediatr.
2012;24(1):23–32.
polymorphismsindetoxificationandDNArepairenzymes. AnnOncol.2007;18(9):1523–8.
14.BozinaN,BrandamanteV,LovricM.Geneticpolymorphismof metabolicenzymesP450(CYP)asasusceptibityfactorfor drugresponse,toxicityandcancerrisk.AhrHigRada Toksikol.2009;60(2):217–42.
15.SmithSM,LeBeauMM,HuoD,KarrisonT,SobecksRM, AnastasiJ,etal.Clinicalcytogeneticassociationsin306 patientswiththerapy-relatedmyelodysplasiaandmyeloid leukemia:theUniversityofChicagoseries.Blood. 2003;102(1):43–52.
16.Pedersen-BjergaardJ,PhilipP,LarsenSO,JensenG,ByrstingK. Chromosomeaberrationsandprognosticfactorsin
therapy-relatedmyelodysplasiaandacutenonlymphocytic leukemia.Blood.1990;76(6):1083–91.
17.KantarjianHM,KeatingMJ,WaltersRS,SmithTL,CorkA, McCredieKB,etal.Therapy-relatedleukemiaand myelodysplasticsyndrome:clinical,cytogenetic,and prognosticfeatures.JClinOncol.1986;4(12):1748–57.
18.TakeyamaK,SetoM,UikeN,HamajimaN,InoT,MikuniC, etal.Therapy-relatedleukemiaandmyelodysplastic syndrome:alarge-scaleJapanesestudyofclinicaland cytogeneticsfeaturesaswellasprognosticfactors.IntJ Hematol.2000;71(2):144–52.
19.OraziA,CattorettiG,SoligoD,LukschR,
Lambertenghi-DelilierG.Therapy-relatedmyelodysplastic syndromes:FABclassification,bonemarrowhistology,and immunohistologyintheprognosticassessment.Leukemia. 1993;7(6):838–47.
20.OraziA.Histopatologyinthediagnosisandclassificationof acutemyeloidleukemia,myelodysplasticsyndromes,and myelodysplastic/myeloproliferativediseases.Pathobiology. 2007;74(2):97–114.
21.YunisJJ,SawyerJR,BallDW.Thecharacterizationof high-resolutionG-bandedchromosomesofman. Chromosoma.1978;67(4):293–307.
22.TanizawaRS,KumedaCA,AzevedoNetoRS,LealAM,Ferreira PB,VellosoEDRP.Karyotypicandfluorescentin-situ
hybridizationstudyofthecentromereofchromosome7in secondarymyeloidneoplasms.RevBrasHematolHemoter. 2011;33(6):425–31.
23.GreenbergP,CoxC,LeBeauMM,FenauxP,MorelP,SanzG, etal.Internationalscoringsystemforevaluatingprognosisin myelodysplasticsyndromes.Blood.1997;89(6):2079–88.
24.Quintás-CardamaA,DaverN,KimH,DinardoC,JabbourE, KadiaT,etal.Aprognosticmodeloftherapy-related myelodysplasticsyndromeforpredictingsurvivaland transformationtoacutemyeloidleukemia.ClinLymphoma MyelomaLeuk.2014;14(5):401–10.
25.TamCS,SeymourJF,PrinceHM,KenealyM,WolfM, JanuszewiczEH,etal.Treatment-relatedmyelodysplasia followingfludarabinecombinationchemotherapy. Hematologica.2006;91(11):1546–50.
26.ParkMJ,ParkYH,AhnHJ,ChoiW,PaikKH,KimJM,etal. Secondaryhematologicalmalignanciesafterbreastcancer chemotherapy.LeukLymphoma.2005;46(8):1183–8.
27.LeDeleyMC,SuzanF,CutuliB,DelalogeS,ShansaldinA, LinassierC,etal.Anthracyclines,mitoxantrone,radiotherapy andgranulocytecolony-stimulatingfactor:Riskfactorsfor leukemiaandmyelodysplasiasyndromeafterbreastcancer.J ClinOncol.2007;25(3):292–300.
28.JostingA,WiedenmannS,FranklinJ,MayM,SieberM,WolfJ, etal.Secondarymyeloidleukemiaandmyelodysplastic syndromesinpatientstreatedforHodgkin’sdisease:areport fromtheGermanHodgkin’sLymphomaStudyGroup.JClin Oncol.2003;21(18):3440–6.
29.Pedersen-BjergaardJ,AndersenMT,AndersenMK.Genetic pathwaysinthepathogenesisoftherapy-related
myelodysplasiaandacutemyeloidleukemia.HematologyAm SocHematolEducProgram.2007:392–7.
30.AndersenMK,JohanssonB,LarsenSO,Pedersen-BjergaardJ. ChromosomalabnormalitiesinsecondaryMDSandAML. Relationshiptodrugsandradiationwithspecificemphasis onthebalancedrearrangements.Haematologica.