w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Original
article
A
Phase
Ib
open
label,
randomized,
safety
study
of
SANGUINATE
TM
in
patients
with
sickle
cell
anemia
Hemant
Misra
a,∗,
James
Bainbridge
a,
John
Berryman
a,
Abraham
Abuchowski
a,
Kenneth
Mauricio
Galvez
b,
Luis
Fernando
Uribe
c,
Angel
Luis
Hernandez
d,
Nestor
Rodolfo
Sosa
eaProlongPharmaceuticals,SouthPlainfield,UnitedStates bHospitalPabloTobonUribe,Medellin,Colombia cFundaciónReinaIsabel,Cali,Colombia dFundaciónBIOS,Barranquilla,Colombia
ePanAmericanMedicalResearchInstitute,Pamri,Panama
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received22February2016 Accepted22August2016 Availableonline20October2016
Keywords:
Sicklecelldisease SANGUINATE Safety Clinicaltrial
a
b
s
t
r
a
c
t
Background: Treatment ofsicklecellanemia isachallengingtask anddespitethewell understoodgeneticandbiochemicalpathwayofsicklehemoglobin,currenttherapy contin-uestobelimitedtothesymptomatictreatmentofpain,supplementaloxygen,antibiotics, redbloodcelltransfusionsandhydroxyurea.SANGUINATEisacarbonmonoxidereleasing moleculeandoxygentransferagentunderclinicaldevelopmentforthetreatmentofsickle cellanemiaandcomorbidities.
Methods: Anopen-labelrandomizedPhaseIbstudywasperformedinadultsicklecell ane-miapatients.TwodoselevelsofSANGUINATEwerecomparedtohydroxyureain24 homozy-gotesforHbSS.Twelvesubjectsreceivedeitheralowdose(160mg/kg)ofSANGUINATEor 15mg/kghydroxyurea.Another12subjectsreceivedeitherahighdose(320mg/kg)of SAN-GUINATEor15mg/kghydroxyurea.TheprimaryendpointwasthesafetyofSANGUINATE
versushydroxyureainsicklecellanemiapatients.Secondaryendpointsincluded determi-nationoftheplasmapharmacokineticsandassessmentofhematologicmeasurements.
Results: Musculoskeletalrelatedadverse eventswerethe mostcommon. Transient tro-ponin Ilevels increased in three patients, one of whom had anincrease in tricuspid regurgitantvelocity;however,noclinicalsignswerenoted.Followinganassessmentofvital signs,tricuspidregurgitantvelocity,electrocardiogram,serumbiochemistry,hematology, urinalysis,andanalysisofreportedadverseevents,SANGUINATEwasfoundtobesafein stablesicklecellanemiapatients.
Conclusions: Theclinicaltrialmetitsprimaryobjectiveofdemonstratinganacceptable safetyprofileforSANGUINATEinpatientswithsicklecellanemia.Thistrialestablished thesafetyofSANGUINATEatbothdoselevelsandpermitteditsadvancetoPhaseIItrials.
©2016Associac¸ ˜aoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.Published byElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense (http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗
Correspondingauthorat:ClinicalDevelopment,300BCorporateCourt,SouthPlainfield,NJ07080,UnitedStates. E-mailaddress:[email protected](H.Misra).
http://dx.doi.org/10.1016/j.bjhh.2016.08.004
Introduction
Treatmentofsicklecellanemia(SCA)isachallengingtaskand thereisonlyonedrug,hydroxyurea,approvedbytheFoodand DrugAdministration(FDA)oftheUnitedStates.Painisthe mostfrequentmanifestationofSCAandisthoughttobea consequenceofvaso-occlusion.Vaso-occlusivecrisesarethe primarycauseoffrequenthospitalizationofSCApatientsand areamajorcauseofdeathinadultSCApatients.1,2Despitethe
well-understoodgeneticand biochemicalpathwayofsickle hemoglobinandmanydiscoveriesofbiomarkersofsicklecell pathophysiology,modern-daytherapycontinuestobelimited to symptomatic treatment of pain, supplemental oxygen, antibioticstherapy,redbloodcelltransfusions,and hydrox-yurea.SCAisaninheritedblooddisordercausedbyadefective hemoglobinprotein.Thepolymerizationofsicklehemoglobin isassociatedwithmanyabnormaldownstreamprocesses,but nosinglepathwayhasbeenshowntoplayaprimaryorcritical roleincomplicationsoccurringinSCApatients.Thiscascade ofeventsisresponsibleforthedevelopmentofcomorbidities associatedwithSCAsuchasvaso-occlusion,stroke,legulcers, andacutechestsyndrome.
SANGUINATE(pegylatedbovinecarboxyhemoglobin) rep-resentsanovelapproachtotreatingacuteexacerbationsof SCAbytargetingtheunderlyinginflammationandcausesof hypoxia.SANGUINATEisacarbonmonoxidereleasing/oxygen transferagentbeingdevelopedforthetreatmentofanemic andischemichypoxiathatresultfromcongenitaloracquired hemoglobinopathies and vasculopathies, such as SCA and thalassemia,andfromcerebrovascularorperipheralvascular diseases.
As SANGUINATE contains a hemoglobin core, there are particular concerns regarding potential vasoactivity. Trials performed with previous hemoglobin-based oxygen carri-ers reported adverse events such as hypertension, cardiac arrhythmias/conduction disorders, gastrointestinal symp-toms,abnormalliverfunctiontestsandhemorrhage/anemia.3
The underlying pathophysiological mechanisms for these cardiac effects are not precisely known but they have been attributed to the scavenging of nitric oxide.4
SAN-GUINATE,duetothemodificationbypolyethyleneglycoland the anti-vasoconstrictive activity ofcarbon monoxide, has demonstrated no vasoactivity in vivo.5 An ascending dose
studyofthreecohortsofeighthealthyvolunteersfoundno seriousadverseeventsatdosesof80,120or160mg/kg.6This
PhaseIbtrialrevealednoserioustreatment-relatedadverse effectsandshoweddose-proportionalpharmacokinetics.As SCApatientssuffer from inflammationand anemia,which causeanumberofcomorbidities,anopenlabel,randomized PhaseIbtrialwasundertakentoensurethesafety of SAN-GUINATEinclinicallystablepatientswhoarehomozygousfor SCA.
Methods
This open label randomized Phase Ib trial was conducted in two countries and four medical centers in Central and SouthAmerica.Thesestudieswereconductedincompliance withtheUSFoodandDrugAdministrationregulations.The
trialwasregisteredasNCT01848925.Protocolsweredesigned togetherwiththeinvestigators.Approvalsweregrantedbythe Ethics CommitteesandRegulatoryAuthorities.Theauthors hadaccesstoprimaryclinicaltrialdata.
AdultpatientswithconfirmedSCAwereenrolled.Eligibility criteriaincludedageof18yearsorolder,baselinehemoglobin level>6or<10g/dL,takinghydroxyureaornot,butmusthave been dose stabilized foratleast threemonths and ableto discontinuehydroxyureaforsevendayspriorto randomiza-tion. Female patients ofchildbearing age were requiredto useamedicallyacceptableformofcontraceptionduringboth studies and negative serum pregnancytests were required atenrollmentandpriortoinfusion.Patientexclusion crite-ria included individuals on a chronic transfusion program (definedasregulartransfusionsevery2–8weeks),acutechest syndrome,seriousinfections,allergiestohydroxyurea,history ofclinicallysignificantdiseasesandelectrocardiogram(ECG) abnormalities.Moreoverpatientswereexcludediftheyhad had morethan sixEmergency Roomvisits/hospitalizations peryearforSCA-relatedpainevents,renalorliver dysfunc-tion,troponinI >0.31ng/mL,amylaseor lipase>1.1×upper
limitofnormal,treatmentwithinvestigationaldrugwithin60 daysorintentiontobeginnewdrugtherapyduringthestudy period.
Preparationanddosing
SANGUINATETM (ProlongPharmaceuticals,LLC,South
Plain-field, New Jersey) 40mg/mL for intravenous infusion was providedin500mLethylenevinylacetatebloodbagswhich wereshippedinheat-sealedMylar,gasimpermeablefoil over-packbagscontaininganinertgas,whichservedtoprotectthe product.SANGUINATEwasstoredundersecureconditionsina locked,limited-accessrefrigerator,at2–8◦
C.Droxia® (hydrox-yurea;BristolMyersSquibb,PrincetonNJ)as100mgcapsules wasobtainedthroughacommercialpharmacyandprovided unalteredaspertheproductlabeling.
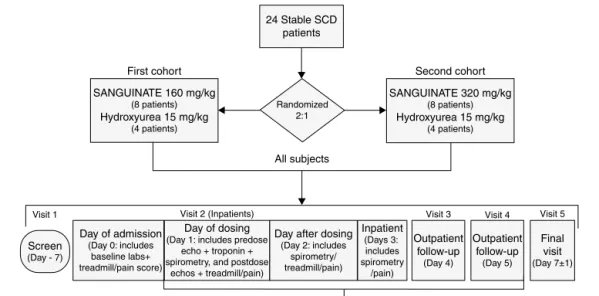
Twenty-fouradultSCApatients(HbSS)wererandomized 2:1toreceive,unblinded,eitherasingle2-hintravenous infu-sion of SANGUINATE, or a standard dose of hydroxyurea (HU)with2hatrestingstage.Thefirst12 patientswereto receive either160mg/kgofSANGUINATE(eight patients)or 15mg/kgofhydroxyurea(four patients),and thesecond 12 patients were to receive either 320mg/kg of SANGUINATE (eightpatients)or15mg/kgofhydroxyurea(fourpatients).The overallstudydesignispresentedinFigure1.
Safetyassessment
24 Stable SCD patients
First cohort Second cohort
All subjects
Randomized 2:1
Visit 1
Screen
(Day - 7)
Day of admission
(Day 0: includes baseline labs+ treadmill/pain score)
Day after dosing
(Day 2: includes spirometry/ treadmill/pain)
Inpatient
(Days 3: includes spirometry
/pain)
Outpatient follow-up
(Day 5)
Outpatient follow-up
(Day 4)
Final visit
(Day 7±1)
Day of dosing
(Day 1: includes predose echo + troponin + spirometry, and postdose
echos + treadmill/pain) Visit 2 (Inpatients)
+ PK blood draws for patients reciving SANGUINATE
Visit 3 Visit 4 Visit 5
SANGUINATE 160 mg/kg
(8 patients)
Hydroxyurea 15 mg/kg
(4 patients)
SANGUINATE 320 mg/kg
(8 patients)
Hydroxyurea 15 mg/kg
(4 patients)
Figure1–Overallstudydesign.
Pharmacokineticassessment
Plasma SANGUINATE concentrationswere quantified using avalidatedhighperformanceliquidchromatography(HPLC) method. Serial blood samples for pharmacokinetic analy-sis were collected at baseline and at 0.5, 1, 1.5, 2, 4, 6, 8, 12, 24, 36, 48, 72 and 96h from the start of infusion. Non-compartmentalpharmacokineticmethodswereusedto determinethepharmacokineticparameters,whichincluded maximum and minimum measured plasma concentration (CmaxandCmin,respectively),timetoreachmaximumplasma
concentration(tmax),theareaundertheplasmaconcentration versustimecurvefromtimezerotothetimeofthelast mea-surableplasmaconcentration[areaundercurve(AUC)0→],
areaundertheplasmaconcentrationversustimecurvefrom timezerotoInfinity(AUC0→∞),terminalhalf-life(t1/2)and
theapparenteliminationrateconstant(z).
Results
Demographicsanddisposition
Overall, the majority of patients were female (15) and of race ‘other’ (23 reported as Hispanic/Latino, and Black or mixed/multiracial).Patients inthe 160mg/kgSANGUINATE treatmentgroupwereonaverageslightlyyoungerthanthe other treatment groups, but this group also included the oldest patient inthe trial (54 years). There was no signif-icant difference inaverageheightand weight betweenthe hydroxyurea-treatedand theSANGUINATE-treatedpatients. There were no remarkable differences between treatment groupsinmedicalhistoryandtherewerenounexpected find-ings(notrelatedtoSCA)foranypatientinthebaselinephysical examination.
Atotalof24 stableSCApatientsfrom clinicalcentersin ColombiaandPanamawereenrolled.Ofthe24patients,22 receivedtheirassignedstudymedicationandcompletedthe studyasperprotocol.FifteenpatientsreceivedSANGUINATE
and sevenpatientsreceivedhydroxyurea.Two patients dis-continuedbeforereceivingmedications.
Pharmacokinetics
ThepharmacokineticsofSANGUINATEweredose-dependent. ThemeanbloodlevelsofSANGUINATEforthetwodosegroups are showninFigure2.For patientsreceivingthe160mg/kg dose ofSANGUINATE, the mean peak concentration (Cmax)
was2.59mg/mLandthemeanpeakconcentrationwiththe 320mg/kg dosewas 6.46mg/mL. Both maximums occurred at2h(completionoftheinfusion).Doublingthedose from 160mg/kgto320mg/kgledtoamean150%increaseinpeak bloodlevelofSANGUINATEinthisSCApatientpopulation.Ina previousstudyofhealthysubjectsreceivingasingleinfusion of160mg/kgSANGUINATE,allofthesixsubjectshadblood levelsbelowthelevelofdetectionat96haftertheinfusion.6
Safety
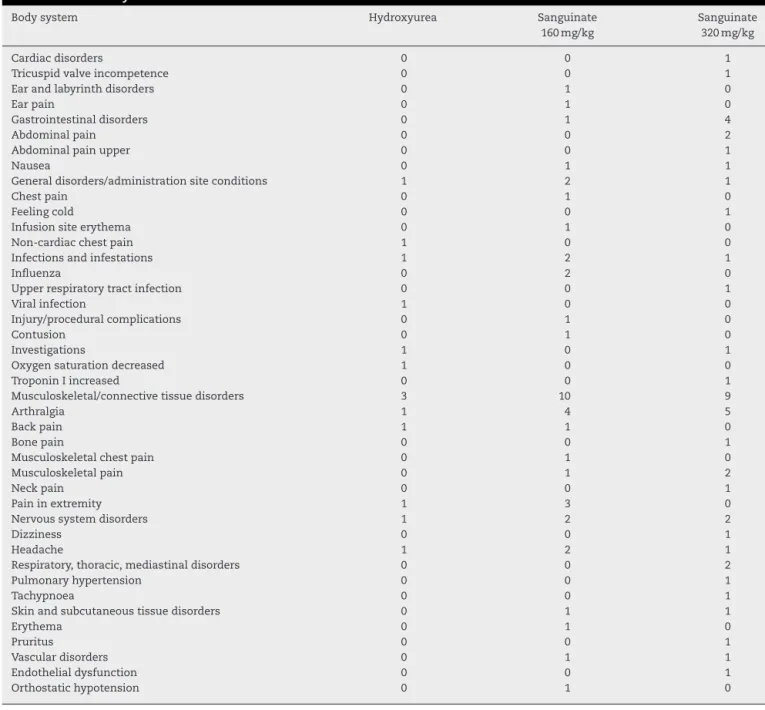
MoreadverseexperienceswerereportedintheSANGUINATE groups thanreportedinthe hydroxyureagroups. Ofthe 44 reported adverse events in SANGUINATE-treated patients, 16 were from only two of the 15 patients. In addition, 46 ofthe 51reportedadverse eventsinvolving pain(including headache).Musculoskeletal andconnectivetissue disorder-related adverse events were the mostcommonly reported, with arthralgia accounting forten (nineSANGUINATE, one hydroxyurea)ofthe51reports(Table1).
0.00 1.00 2.00 3.00 4.00 5.00 6.00 7.00
96 84
72 60
48 36
24 12
0
160mg/kg MEAN 320mg/kg MEAN
Figure2–MeanplasmaconcentrationofSANGUINATE(mg/mL)bydose.
Manyofthelaboratoryparametersthatwereabnormalat baselineremainedoutsideofthenormalrangeforthe dura-tionofthestudy,andformanylaboratoryparameters,there werenomeaningfuldifferencesbetweentreatmentgroups. Meanvaluesforhemoglobinandhematocritovertimeshow thattreatmentwithSANGUINATEdoesnotprovidean appre-ciableincreaseinquantityorconcentrationofhemoglobinin thesepatients.
However,thelevelsofdirect(conjugated)bilirubin(Table2) demonstratedaclearmeandecreaseonthedayofdosing rela-tivetobaselinelevelsforthepatientsreceivingSANGUINATE, which was not seen in the hydroxyurea treatment group. Notably,themeanlevelfollowinginfusionof320mg/kg SAN-GUINATE approximates the upperlimit of the laboratory’s normalrange.Thismeantreatmentdifferenceisnot appar-entintheleveloftotalbilirubin,butiscloselymirrored,albeit
50
40
30
20
10
0
0 20 40 60 80 100 120 140 160
-10
-20
HU SG160 SG320
Table1–Summaryofadverseevents.
Bodysystem Hydroxyurea Sanguinate Sanguinate
160mg/kg 320mg/kg
Cardiacdisorders 0 0 1
Tricuspidvalveincompetence 0 0 1
Earandlabyrinthdisorders 0 1 0
Earpain 0 1 0
Gastrointestinaldisorders 0 1 4
Abdominalpain 0 0 2
Abdominalpainupper 0 0 1
Nausea 0 1 1
Generaldisorders/administrationsiteconditions 1 2 1
Chestpain 0 1 0
Feelingcold 0 0 1
Infusionsiteerythema 0 1 0
Non-cardiacchestpain 1 0 0
Infectionsandinfestations 1 2 1
Influenza 0 2 0
Upperrespiratorytractinfection 0 0 1
Viralinfection 1 0 0
Injury/proceduralcomplications 0 1 0
Contusion 0 1 0
Investigations 1 0 1
Oxygensaturationdecreased 1 0 0
TroponinIincreased 0 0 1
Musculoskeletal/connectivetissuedisorders 3 10 9
Arthralgia 1 4 5
Backpain 1 1 0
Bonepain 0 0 1
Musculoskeletalchestpain 0 1 0
Musculoskeletalpain 0 1 2
Neckpain 0 0 1
Paininextremity 1 3 0
Nervoussystemdisorders 1 2 2
Dizziness 0 0 1
Headache 1 2 1
Respiratory,thoracic,mediastinaldisorders 0 0 2
Pulmonaryhypertension 0 0 1
Tachypnoea 0 0 1
Skinandsubcutaneoustissuedisorders 0 1 1
Erythema 0 1 0
Pruritus 0 0 1
Vasculardisorders 0 1 1
Endothelialdysfunction 0 0 1
Orthostatichypotension 0 1 0
Table2–DirectBilirubinandgamma-glutamyltranspeptidase(GGT).
Units Statistic Hydoxyurea Sanguinate(160mg/kg) Sanguinate(320mg/kg)
Baseline result
Visit result
Difference Baseline RESULT
Visit result
Difference Baseline result
Visit result
Difference
Bilirubin mg/dL n 7 7 7 8 8 8 7 7 7
Mean 0.7 0.7 0 1.2 0.5 −0.7 0.7 0.2 −0.5
Std.dev. 0.2 0.2 0.1 0.7 0.4 0.3 0.2 0.1 0.1
Median 0.7 0.6 0 1.2 0.4 −0.7 0.6 0.2 −0.4
Minimum 0.3 0.5 −0.2 0.4 0.1 −1.2 0.5 0 −0.7
Maximum 1.1 1.2 0.2 2.6 1.4 −0.3 1 0.4 −0.3
GGT U/L n 7 7 7 8 8 8 7 7 7
Mean 41 40.4 −0.6 55.5 33.5 −22 49.1 26.6 −22.6
Std.dev. 29.3 30.4 1.9 53 40 16.5 46.1 36.3 11.9
Median 42 41 −1 35.5 22.5 −19 24 9 −17
Minimum 10 10 −3 22 3 −59 14 1 −42
40
30
20
10
0
0 10 20 30 40 50
-10
-20
HU SG160 SG320
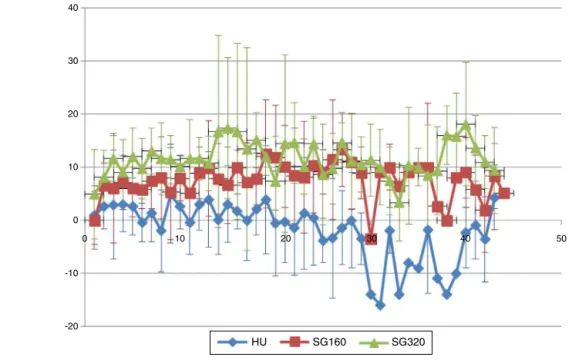
Figure4–Diastolicbloodpressure.
always within the normal range, in the levels of gamma-glutamyltranspeptidase.
Themeanresultsofthechemicalurinalysistestfor pres-enceofbloodintheurineshowatreatment-specific(though not apparently dose-specific) difference following infusion withSANGUINATE.Themeanredbloodcelllevelsseenupon microscopicanalysisapproximatelymirrorthisfinding,which may be the result of the increased colloid-osmotic pres-sureproducedbytheinfusion,causinganincreaseinforced glomerularfiltration.Asimilarresultwasseenforurinary pro-tein.
TherewerebriefbutsubstantialincreasesintroponinI lev-elsinthreepatientsreceivingSANGUINATE(320mg/kg)andin onepatientreceivingHU.Theincreaseswereofshortduration andnotaccompaniedbyanyclinicallyidentifiedorpatient reportedadverseexperiences.Oneofthethreepatientswith elevatedtroponinlevelsalsohadareportedseriousadverse event due to an increase in tricuspid regurgitant velocity (TRV)which was labeledas asign ofmoderate pulmonary hypertension;however,associatedsymptomsofpulmonary hypertensionwerenotpresentafterangiography.Theother twopatientshadbaselinevaluesnearorabovetheupperlimit ofthelaboratoryreferencerangefortroponinI(0.028ng/mL). Thehighestmeasuredlevelwasalsotheshortestlasting:the serumtroponinIlevelofonepatientwasassayedatnearly 16-timestheupperlimitat1haftertheendofSANGUINATE infusion.Yet,despitereadingabovethelimitatbaseline, tro-poninIwasdowntothelowlevel ofnormal(0.007)bythe timeofthenextmeasurement5hlater,whereitremainedfor thedurationofthestudy.Becauseoftheshortduration,and becauseitwasnotaccompaniedbyanyclinically-identifiedor patient-reportedadverseexperiences,thesewerenotreported bytheinvestigatorsasserious adverseevents.Onepatient receivinghydroxyureaalsohadabriefincreaseintroponin Ilevel(0.045ng/mL) abovethe upperlimitofthelaboratory referencerangeat72hafterdosing.
Discussion
The pathobiology ofSCA is characterizedbyinflammation and oxygen deprivation. While hydroxyurea therapy has decreasedthepainfulepisodesofSCA,poorcomplianceand non-response by a significant proportion of SCA patients resultsinthedevelopmentofvaso-occlusivecrisesandother acute comorbidities. SANGUINATE is a novel construct of hemoglobin that contains carbon monoxide and pegylated bovine carboxyhemoglobin. It has been shown to reduce infarctvolume inanimalmodels7,8 andhas been
adminis-tered undermultipleemergency InvestigationalNewDrugs (eINDs).9,10 Invitrostudieshavedemonstrated theabilityof
SANGUINATE to return SCA blood cells to a more normal morphology11 and demonstrated the transfer ofoxygen to
hypoxiccells.
This first in-patients study assessed the safety-related effectsofSANGUINATEinSCApatients.Sinceonly15patients received SANGUINATEand sevenpatients received hydrox-yurea, the size of the study population was too small to allowacalculationofstatisticalsignificancebetween treat-ment groups. It wasobserved that many ofthe laboratory parameters being measured were abnormal at baseline in this population as expected. The damage that has devel-opedinthesepatientsfromalifetimeofhemolyticanemia andischemichypoxiameansthattheypresentanextremely diverserangeofpossiblephysiologicalresponsesthatmaybe undetectableusingtheparametersandmethodsofthisstudy. Thedecreaseinbilirubinandgamma-glutamyl transpep-tidase maybeduetothe impactofSANGUINATEupon the redbloodcell.SANGUINATEhasbeenshownto‘unsickle’red bloodcellsinSCApatientsinvitro.12Theimprovementinred
Theclinicalsignificanceofthetransientincreasesin tro-ponin I levels seen in some of these patients is also not clear.ThetransientelevationoftroponinIinthreeof15 sub-jectslastedafewhoursorafewdays,without sequelaeor repeatedelevations.CurrentAmericanCollegeofCardiology Foundation(ACCF)/AmericanHeartassociation(AHA) guide-linesdonotdefinethedurationoftroponinelevationneeded toindicatepathology,anddonotrecommendtheir diagnos-ticor prognosticuse alone inheart failure.13 Furthermore,
asclarifiedinthe2007JointEuropeanSocietyofCardiology (ESC)/ACCF/AHA/WorldHeartFederation(WHF)report “Uni-versalDefinition ofMyocardialInfarction”, serial measures ofcardiactroponinaftertheonsetofclinicalsymptomsare neededfordiagnosisofcardiacischemia.14Arapidriseand
fallof troponinI does notfit the standard cardiac disease paradigm, and the return oftroponinI levels tonormal is indicativeofresponsetotreatmentorspontaneous improve-ment.
Theresponseofonepatient,whoreceived320mg/kg SAN-GUINATE, ofmulti-day increases in TRV tolevels typically associatedwithmoderate-to-severepulmonaryhypertension, substantialincreasesinsystemicbloodpressure,andelevated troponinItonearly4-foldtheupperlevelofnormal,lasting severaldays,areresultswhich,albeitparadoxical,were associ-atedwithnoclinically-identifiedorpatient-reportedadverse effects.Pulmonary hypertension,definedbypersistentTRV valuesabove3.0m/s,hasbeencorrelated withasignificant increasedriskofmortalityinSCApatients.15Theimpactof
TRVelevationsabove 3.0m/s that lastforonlya fewdays, however,occurringinSCApatientswithaverageTRVlevels >2.0m/shasnotbeendetermined.Giventhelackofclinical adverseeffectsofthepatient,herprofessedwell-being,and theisolatednatureofthisevent,theimpactofthereported eventontheunderstandingofriskrelatedtothestudydrug inSCApatientsisverylimited.
InfusionofSANGUINATEatboth160and320mg/kg gen-erated anexpected increase inarterial pressure due toits colloid osmotic properties, which resolved without appar-ent sequelae. Meansystolic and diastolic systemic arterial pressurewasincreasedinSANGUINATE-treatedpatients com-pared to hydroxyurea-treated patients, but accompanying mean increasesinTRVvalueswere notseeninthis study. TheknowntransienteffectofSANGUINATEonarterial pres-sure,possiblyincludingpulmonaryarterialpressurethatwas undetectableinthissmallstudy,isbelievedtobeduesolely toitsoncoticeffect.Thelackofclinicallymeaningfuladverse effectsresultingfromthepressureincreasefurthersupports atransientfluid-volumebasisforthemechanism.
Pharmacokinetic results found that SANGUINATE (160mg/kg) had a prolonged T1/2 in stable SCA patients
(19.56h) compared to that found in healthy volunteers (13.75h).7InthePhaseIstudywithhealthyvolunteers,itwas
observedthathaptoglobinlevels weresignificantlyreduced followingSANGUINATEadministration.Becausethecoreof SANGUINATEishemoglobin,it hasbeenproposed thatthe clearance mechanismwill bethe same asthe mechanism used to clear native hemoglobin following hemolysis by the reticuloendothelial system. Because ofthe widespread hemolysisinSCApatients,thisclearancemechanismwould beburdenedbythepatient’sextensivecell-freehemoglobin,
thus reducing the rate atwhichthis mechanism canclear SANGUINATE, which would lead to a longer circulatory half-life.
Conclusion
Thisisafirstin-patientstudyofpatientswithstableSCAwith either160mg/kgor320mg/kgofSANGUINATE.Whilethere weremoreadverseeventsintheSANGUINATEarm,theywere mild and self-limited. Following assessment ofvital signs, echocardiographicmeasuresofTRV,electrocardiogram anal-ysis,laboratorymeasuresofserumbiochemistry,hematology andurinalysis,andreportedadverseevents,noclearevidence ofclinicallymeaningfulsafetyconcernswereidentified.These resultssupportfurtherdevelopmentofSANGUINATEforthe treatmentofSCAcomorbiditiesandinitiationoffurther clin-icaltrialsdesignedtooptimizedosingandselectappropriate endpointstoassesssafetyandefficacy.
Funding
ThisstudywassupportedbyresearchfundingfromProlong Pharmaceuticals.
Conflicts
of
interest
HM,JB,JBandAAareemployeesofProlongPharmaceuticals and InvestigatorsKMG, LFU,ALH and NRSwere fundedby ProlongPharmaceuticals.
r
e
f
e
r
e
n
c
e
s
1.PerronneV,Roberts-HarewoodM,BachirD,Roudot-Thoraval F,DelordJM,ThuretI,etal.Patternsofmortalityinsicklecell diseaseinadultsinFranceandEngland.HematolJ.
2002;3(1):56–60.
2.PlattOS,BrambillaDJ,RosseWF,MilnerPF,CastroO, SteinbergMH,etal.Mortalityinsicklecelldisease.Life expectancyandriskfactorsforearlydeath.NEnglJMed. 1994;330(23):1639–44.
3.LanzkronS,StrouseJJ,WilsonR,BeachMC,HaywoodC,Park H,etal.Systematicreview:hydroxyureaforthetreatmentof adultswithsicklecelldisease.AnnInternMed.
2008;148(12):939–55.
4.SilvermanTA,WeiskopfRB.Hemoglobin-basedoxygen carriers:currentstatusandfuturedirections.Anesthesiology. 2009;111(5):946–63.
5.CabralesP.Examiningandmitigatingacellularhemoglobin vasoactivity.AntioxidRedoxSignal.2013;18(17):2329–41.
6.ZhangJ,CaoS,KwansaH,CrafaD,KiblerKK,KoehlerRC. Transfusionofhemoglobin-basedoxygencarriersinthe carboxystateisbeneficialduringtransientfocalcerebral ischemia.JApplPhysiol.2012;113(11):1709–17.
7.MisraH,LickliterJ,KazoF,AbuchowskiA.PEGylated carboxyhemoglobinbovine(SANGUINATE):resultsofaPhase Iclinicaltrial.ArtifOrgans.2014;38(8):702–7.
8.AnanthakrishnanR,LiQ,O’SheaKM,QuadriN,WangL, AbuchowskiA,etal.CarbonmonoxideformofPEGylated hemoglobinprotectsmyocardiumagainst
9. KlausJA,KiblerKK,AbuchowskiA,KoehlerRC.Early treatmentoftransientfocalcerebralischemiawithbovine PEGylatedcarboxyhemoglobintransfusion.ArtifCellsBlood SubstitImmobilBiotechnol.2010;38(5):223–9.
10.AlaaliY,IocoE,VarelasP,AbdelhakT,MastorodimosV, MendezM.UseofSanguinateinacutechestsyndrome.J SickleCellDisHemoglobinopat.2014;1:1.
11.ParmarD.AcasestudyofSANGUINATETMinapatientwitha
comorbidityduetoanunderlyinghemoglobinopathy.JSickle CellDisHemoglobinopat.2014;1:2.
12.JubinR,BuontempP,YglesiasRA,AbuchowskiA,ChenY, KazoG,etal.Rapidreversalofredbloodcellsickling promotedbyPEGylatedcarboxyhemoglobinbovinegas transferproperties.Abstract1371.In:56thASHannual meetingabstractsandprogram.2014.
13.MisraH,BuontempoP,BuontempoC,Yglesias,R,ChenY, JubinR,etal.Anti-inflammatoryactivityandrapidreversalof sicklecellmorphologybyPEG-COHbmediatedgastransferin vitro.PresentedinHEMOBRAZIL2015,Braziliancongressof hematology,hemotherapy,andcelltherapy.November20, 2015.
14.YancyCW,JessupM,BozkurtB,ButlerJ,CaseyDE,Drazner MH,etal.2013ACCF/AHAguidelineforthemanagementof heartfailure:areportoftheAmericanCollegeofCardiology Foundation/AmericanHeartAssociationTaskForceon PracticeGuidelines.JAmCollCardiol.2013;62(16):e147–239.