Original Article
SCREENING OF BODY M ASS INDEX AND FUNCTIONAL FLATFOOT
IN ADULT: AN OBSERVATIONAL STUDY
Ashw ini Chougala
1, Vidit Phanse *
2, Erohit Khanna
3, Sudipta Panda
4.
* 1 Lect urer, Dept . of Physiot herapy, KLE’U Inst it ute of Physiot herapy, Belagavi, Karnataka, India. 2,3,4 BPT Intern, Dept . of Physiot herapy, KLEU’S Inst it ute of Physiot herapy, Belagavi, Karnataka,
India.
Background: There is a r elat ion bet w een flat foot and increased Body M ass Index (BM I). Incr eased w eight leads t o increase plant ar pr essur e causing reduced dist ance bet w een ground and ar ches of t he foot . The purpose of t he present st udy is t o estim at e t he prevalence of flat feet in college going st udents, t o determ ine the relationship bet w een flat foot and Body M ass Index (BM I), and t o com pare prevalence of flat foot am ong college boys and gir ls.
M at erials and M ethod: Sam ples w ere t aken according t o w illingness for par t icipat ion; inf orm ed consent w as given and signed from t hem . Height and w eight of subject s w ere m easured by using standard apparat us. Total num bers of m ales screened w ere 46 and fem ales w ere 182. BM I w as considered as t he index of obesit y .The int ernat ional BM I cut –off values w er e used t o det er m ine obesit y (BM I> 95t h percent ile), and foot st ruct ure assessm ent w as perform ed w it h Denis M et hod. Significant relat ionship bet w een obesit y and flat foot w as observed.
Result: A significant relat ionship (Pd” 0.01) w as found bet w een t he prevalence of f lat foot and BM I. Also m ales w er e found t o have higher prevalence of f lat foot t han w om en in t he age group of 18-25 years.
Conclusion: The result s of t his st udy suggest t hat t here is r elat ionship bet w een incr eased w eight of person and st r uct ur e of t he foot . M ales ar e m or e prone t o flat foot t han fem ales in t he age group of 18-25 years.
KEY W ORDS: Flat foot , Body M ass Index, Obesit y.
ABSTRACT
INTRODUCTION
Address for correspondence:: Dr. Vidit Phanse, BPT Intern, Dept . of Physiot herapy, KLEU’S Instit ute of Physiot herapy, JNM C Campus, Nehru Nagar, Belagavi - 590 010, Karnataka, India.
E-M ail: vidit [email protected]
International Journal of Physiotherapy and Research, Int J Physiother Res 2015, Vol 3(3):1037-41. ISSN 2321-1822 DOI: ht t p:/ / dx.doi.org/10.16965/ ijpr.2015.133
Quick Response code
Access this Article online
International Journal of Physiotherapy and Research
ISSN 2321- 1822
w w w.ijm hr.org/ ijpr.htm l
DOI: 10.16965/ ijpr.2015.133
Received: 13-04-2015 Peer Review : 13-04-2015 Revised: None
Accept ed: 05-05-2015 Published (O): 11-06-2015 Published (P): 11-06-2015
Flat foot is also called as pes planus or fallen arches. Flat foot i.e. acquired flat foot develops due t o injury , prolonged st ress t o t he foot , obesit y, illness, fault y biomechanics [1]. It is a post ural deformit y in w hich t he arch of t he foot collapses. Flat foot is oft en a complex disorder w it h sympt oms and varying degrees of defor-mit y and disabilit y. There are several t ypes of flat foot in w hich one of t hem have a common
the biomechanics of the normal arch and respond w it h a t reat ment t hat st rengt hens t he support -ing st ruct ures of t he arch or w eakens t he arch-flat t ening effect s on t he arch [2].
Flat foot i.e. acquired flat foot develops due t o injury, prolonged st ress t o t he foot , obesit y, illness, f ault y biom ech anics [ 3] . It is t hat recognized post erior tibia t endon dysfunction as a common cause of acquired adult flat foot [4].
It w asreport ed t hat t he incidence of flat foot in t he populat ion st udied w as found t o be 16.4%, of w hich 18.1% w ere males and 14.6% females. Fift y percent show ed slight flat-footedness (1st
degree), 28% moderat e (2nd degree) and 22%
show ed ver y m ar ked f lat - foot edn ess (3r d
d egr ee). Th e f r eq uen cy o f o b esi t y an d overw eight in t he same populat ion w as found t o be 27.3% (Cole index>120). Analysis of t he v ar i ance sh o w ed a si gni f i can t d i f f er ence betw een t he Cole Index in subject s w it h flat feet (121.77 +/ - 19.2) and t he rest of t he populat ion examined (110.12 +/ - 15.3). In t his st udy, t he children suffering from t his dysmorphism w ere also found t o be obese or overw eight[4].BM I cat egories - Normal = 18.5 - 24.9, Overw eight =
25 - 29.9, Obesit y = BM I of 30 or greater. M ain
cont ribut ing fact ors for t he increase in body mass index is sedent ary lifest yle, foods in high fat and calories. St ress is also an import ant fact or for obesit y. Grow ing older, t his can lead t o less m uscle m ass and a low er m et abolism making it easier t o gain w eight .
Th e BM I is gen er al l y u sed as a m ean o f correlat ion bet w een groups relat ed by genera m ass and can ser ve as a v ague m ean s of est imat ing adiposit y. The dualit y of t he BM I is t hat , w hilst easy t o use as a general calculat ion, it is limit ed in how accurat e and pert inent t he data obtained from it can be. Generally, the index i s su it ab le f or r eco gni zi ng t r en d s w i t h i n sedent ary or overw eight individuals because t here is a smaller margin for errors[5]. BM I is
used different ly for children. It is calculat ed t he same w ay as for adult s, but t hen compared t o t ypical values for ot her children of the same age. Inst ead of set t hresholds for underw eight and overw eight , t hen, t he BM I percent ile allow s comparison w it h children of t he same sex and age.BM I can be calculat ed quickly and w it hout expensive equipment . How ever, BM I categories
do not take int o account many fact ors such as frame size and muscularit y [6].
M ETERIALS AND M ETHODS
Et hi cal cl ear ance w as o bt ai ned f r o m Inst it ut ional Et hical Commit t ee. Pat ient s w ere screened based on t he inclusion and exclusion crit eria.
Inclusion crit eria included st udent s from KLE universit y campus, age group of 18-25 years. Exclu si on cr i t er ia in clu ded any con genit al deformit ies, callus or corn, unw illingness for part icipat ion. Part icipant s w ere briefed about the nat ure of the study and intervent ion and only t hose part icipant s w illing t o t ake part w ere recruited for the study and informed consent w as obtained. Follow ing requirement s w ere taken from each subject : Name, Age, Gender, Height , Weight , Date of birt h, Sport ing act ivit ies and it s t ime per w eek in hours. Height and w eight w as measured on each individual in light clot hes and w it hout foot w ear using st andard apparat us. Height w as measured from nearest 0.5 cm, w it h t he help of measuring tape. And t o measure t he height m easuring t ape w as fixed t o t he w all. Height w as measured w hile t he subject st ands w it h heel, shoulder and occiput t ouching t he vert ical t ape. Head w as held erect w it h t he ext ernal audit ory meat us and t he low er border o f t h e o r bi t in h or i zon t al p l an e. Al l m easur em en t s w er e t aken by on e of t h e investigat ors. BM I w as calculat ed as w eight (kg) divided by square of the height in meter. Subjects w ere classified according t o WHO classificat ion according t o t heir BM I and w ere classified as underw eight , normal w eight , over w eight and obesit y groups. Also, foot st ruct ure assessment w as perform ed w it h Denis m et hod pr ior t o t est ing, college st udent s feet w ere screened by one of t he invest igat or t o ident ify and exclude subject s w it h any external fact ors t hat may have cont ribut ed t o variat ions in plant ar pressures, such as cal l u ses. Al l su b j ect s u n der w en t foot print screening.
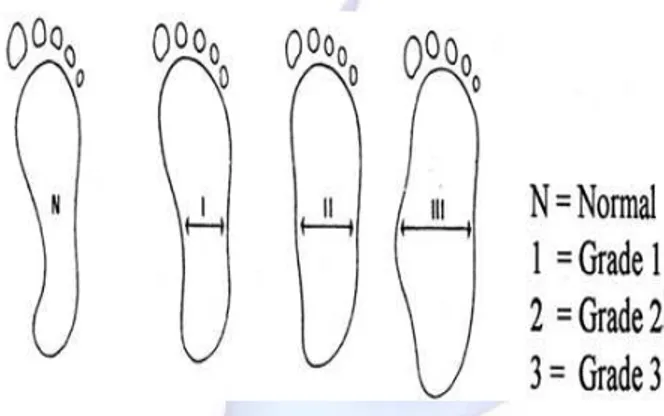
The plant ar foot print w as classified according t o Denis int o t hree grades of flat feet :
Grade 1: The support of lat eral edge of t he foot is half of t hat of met at arsal support .
and forefoot are equal.
Grade 3: Support in t he cent ral zone of t he foot is great er t han t he w idt h of t he m et at arsal support.
These obt ained r esult s w ill be st at ist ically calculat ed for arch index.
Fig.1. Classificat ion of plantar foot print according t o Denis M et hod [11,14].
Statistical Analysis: St at ist ical analysis for t he present st udy w as done manually as w ell as using t he st at ist ic soft w are SPSS 16.0 version so as t o verify t he result s obt ained. For t his pur-pose dat a w as ent ered in an excel spread sheet , t abulat ed and subject ed t o st at ist ical analysis. Stat ist ical test used was Fisher Exact test w hich was ut ilized calculat ion of ‘p-value’, chi-square and degree of freedom w ere calculat ed, signifi-cant differ ence in grades of BM I and DENIS met hod grading w as also calculat ed. ‘p-value’ w as also calculat ed for com parison bet w een males and females t o find out t he prevalence of flat foot . Probabilit y value less t han or equal t o 0.05 w ere st at ist ically significant .
RESULTS
The result of final st udy w as analyzed by DENIS M ETHOD and component s like height , w eight and BM I w ere calculat ed so as t o screen t he correlat ion bet w een BM I and flat foot .
DEM OGRAPHIC PROFILE
Table 1: Represent s num ber of people included in each grade of DENIS m et hod and t heir percent age.
Level of significance, p = 0.001. This t able represent s number of subject having flat foot according to DENIS grading . Grade 2 and Grade 3, w hich represent s people flat foot . It account s t o t ot al of 23.6 %. 11.8% bot h in Grade 2 and Grade 3. Here the p value was found to be 0.001, w hich is st at ist ically significant .
Table 2: According t o gender.
Total numbers of subject s screened w ere 228. Out of t he 228 subject s screened 182 subject s w ere females, of t hem 33 females had flat foot . 46 males w ere screened and out of w hich 21 had f lat f oot . These v alu es w er e st at i cal ly analyzed and p-value w as found t o be 0.001 w hich is highly significant . Also chi-square value w as cal cul at ed , i t w as 13.410. Degr ee o f freedom w as found t o be 3.
Table 3: According t o BM I classificat ion.
This table represent s total number of bot h males and females in relat ion t o DENIS met hod, where t ot al number of subject s w ho fall under grade 0 is 127. Grade 1 consist ed of 47 subject s. Grade 2 and grade 3 w ho have flat foot have, t ot al number of subject are 27 and 27 each. St atist ical analysis w as done and p-value found w as 0.001 w hich is st at ist ically significant . Chi-squar e value found w as 17.410. Degree of freedom w as 3.
DISCUSSION
Flat foot also called as pes planus or fallen arches. It is a post ural deformit y in w hich t he arch of t he foot collapses. There is a funct ional relat ionship bet w een t he st ruct ure of t he arch
DENIS GRADES NUM BERS PERCENTAGE (%) GRADE 0 127 55.7 GRADE 1 47 20.5 GRADE 2 27 11.8 GRADE 3 27 11.8
DEN IS GRADES FEM ALE M ALE GRADE 0 112 15 GRADE 1 37 10 GRADE 2 17 10 GRADE 3 16 11
DENIS GRADES UN DER W EIGHT
NORM AL W EIGHT
OVER
W EIGHT OBESE TOTAL
GRADE 0 26(83%) 80(65%) 15(29.4%) 5(23.8%) 127
GRADE 1 4(12.90%) 25(20.30%) 15(29.4%) 3(14.3%) 47
GRADE 2 0 11(8.9%) 10(19.60%) 6(28.6%) 27
GRADE 3 1(3.2%) 7(5.7%) 11(21.60%) 7(33.3%) 27
of t he foot and t he biomechanics of t he low er l i m b .Thi s st u d y co m p ar es t h e p r eval en ce bet w een flat foot and gender. It also states t he comparison betw een different grades of BM I and flat foot . This w ill help us in giving a clear cut idea w het her t he w eight and gender of a person is responsible for t he arch of t he foot .
It has been proven t hat t here is a vast variat ion in t he prevalence of flexible flat feet report ed by various aut hors [7, 8]. According t o our st udy, t hese differences could be explained by t he t heorem t hat t he aut hors used different age groups or perhaps only made t heir findings at t he end of t he usual evolut ionary period w hen ext r a ev o l ut i o n t o w ar d heal t h y f eet w as improbable. But in our st udy w e used only one age group w here all t he mat urit y is at t ained and so t hese differences in age groups are nullified and result s can be proven reliable. Our st udy st udied adult s bet w een t he ages 18-25 years. A body of higher m ass w it h w eak m usculat ure exer t s ext ra forces on t he arch of t he foot causing w eakness of t he respect ive m uscles causing collapsed arches. It significant ly alt ers t he cont act surface of t he arch and t he ground.
In our st udy, stat ic w eight-bearing foot print s for t he right and t he left foot w ere taken by dipping bot h t he foot one by one inside cont ainer of co lored w at er. As t h e st udy in clud ed t he populat ion of age group 18-25 years t hey had already m at ured and also at t ained puber t y. Obesit y w as permanent fact or in our st udy t hat may cause significant relat ionship bet w een flat fo ot and ob esi t y. Becau se m ass i ncr eases result ed in increased st at ic and dynamic plant ar pressures, causing significant change t o t he st ruct ure of t he feet . How ever, long-term mass increases associat ed w it h obesit y appeared t o f lat t en t he m edial longit udinal ar ch of t he subject s as confirmed by an increased area of foot cont act w it h t he ground [9].
Our st udy show ed t hat t he BM I w as associat ed w it h flat f oot . This can be associat ed w it h excessive belly fat causing w eak abdominals and in t urn causing excessive lordot ic post ure. This causes change in passing of line of gravit y and t ransfer of force t hrough foot . As a result the weight bearing areas are changed. Along w ith t h is i ncr eased f at an d decr eased m u scl e st rengt h due t o decreased muscle fibers causes
collapse arches.
Our st udy show ed t hat males w ere more prone t o f lat f oo t t han f em ales. This r esult s ar e consist ence w it h relat ionship of flat foot and high arch w it h main ant hropological variables w hich is a st udy based on BM I. The higher incidence of males more prone t o flat foot can be given by t he foot w are t hey use. If t he foot -w are is harder t hen it may cause flat foot[10].
Alt hough obesit y and overw eight is a temporary, but it can be t he cause of flat foot . Therefore subject s should pay at t ent ion t o incr easing w eight t hat may cause flat foot and also ot her problems in t he fut ure.
The foot adapt s it self under loading condit ion by m aint aining t he m edial longit udinal arch. Incr easi n g t h e l o ad i n g f u r t h er act i v at es compensat ory mechanisms w hich maint ain t he longit udinal arch and shift s he loads t o t he central and medial forefoot .[11] But treatment and
prevent ion of flat foot may have an effect on an individual’s overall healt h and occurrence of ot her foot and ankle pat hologies [12].
We also found t hat t he presence or absence of flat foot does not modify qualit y of life. Act ivit ies of daily living are not affect ed by flat foot and also t here are no hurdles for performing it . St udies also st at es t hat t here is no problem or short coming in performance in physical funct ioning and also part icipat ion in st ernous physical w ork w ere foot pat hology is included recent . Qualit y of life has been used as a t ool of result s for surgical t reat ment of t he f eet . So m e au t h o r s h ave n ot f ou n d an y dif f er ences in q ualit y of l if e based on t he abnormalit ies found[13].
Conflicts of interest: None
REFERENCES
[ 1] . St ev e n Lo w Sh o es, Si t t i n g, an d Lo w er Bo d y Dysfunct ions Published: Novem ber 22, 2009. [2] . Van Boerum DH1, Sangeorzan BJ , Depar t m ent of
Or t ho pedics and Spor t s M edicin e, Har bo r view M edical Cent er, P.O. Box 359798, Seatt le, WA 98104, USA.
[4] . D. Bordin, De Giorgi, G., M azzocco, G. and Rigon, F. Flat and caves f oot , indexes of obesit y and over w ei ght in a po pul at ion of p r im ar y-scho ol chi ldren. M inerva Pediat r. 2001, 53:7-13.
[5]. Jeukendrup, A.; Gleeson, M . (2005). Sport s Nutrit ion. Hum an Ki net i cs: An Int r o du ct i o n t o En er gy Product ion and Perf orm ance. ISBN 978-0-7360-3404-3.
[ 6] . M .J. Gardner. and D.G. Alt m an. St at ist ics w it h confidence. Brit ish M edical Association: London, 1989.
[ 7] . A. Gar cía-Rodr íguez, et al. Flexible f lat f eet in children: A r eal problem ? Pediat rics. 1999, 103: 84-89.
[8] . Robbins JM . Recognizing, t reat ing, and prevent ing co m m o n f o o t p r o b l em s. Cl ev e Cl i n J M ed . 2000;67(1):45–7,51–2,55–6.
[9] . Shibuya N, Jupit er DC, Cilibert i LJ, VanBuren V, La Font aine J. Char act er ist ics of adult flat foot in t he Unit ed St at es. J Foot Ankle Surg. 2010;49(4):363–8. [10]. Dunn JE, Link CL, Felson DT, Crincoli M G, Keysor JJ, M cKi n l ay JB. Pr e v al e n ce o f f o o t an d an kl e condit ions in a m ult iet hnic com m unit y sam ple of older adult s. Am J Epidem iol.2004;159(5):491–8.
[ 11] .Hassan d esp an d e Nad e r Rah n e m a Rah i m eh M ehdizadeh Relat ionship bet w een obesit y and flat foot in high-school boys and girls. Int ernat ional Journal of Sport s Science and Engineering. 2009;03 (01): 043-049.
[12].A. M . Dowling, J. R. Steele. and L. A . Baur. Does obesity in f l uen ce f o ot st r u ct ur e and pl ant ar p r essu r e pat t erns in pr epubescent childr en? Int J Obese. 2001;25:845 - 852.
[13]. Groarke P, Galvin R, Kelly J, St ephens M M . Qualit y of life in individuals w it h chronic foot condit ions: a cross sect ional observat ional st udy. Foot (Edinb). 2012; 22(2):66–9.
[14]. A. Denis. Pied plat valgus st at ique. Encyclopedie M edico-Chirurgicale Apparei l Locom ot eur. Paris, France: Edit ions Techniques.1974.
How to cite this article
:
Ashw ini Chougala, Vidit Phanse, Erohit Khanna, Sudipta Panda. SCREENING OF BODY M ASS INDEX AND FUNCTIONAL FLATFOOT IN ADULT: AN OBSERVATIONAL STUDY. Int J Physiot her Res 2015;3(3):1037-1041.