Vol-7, Special Issue-Number2-April, 2016, pp1426-1432 http://www.bipublication.com
rt po Re e as C
The effect of orthoses in the management of patients with stroke
Pourghasem Ali1*, EbrahimiTakamjani Ismail2, TaghiKarimi Mohammad3,
Kamali Mohammad4, Jannesari Ladani Mohammad5
and Salafeyan Esfahani Iman6.
1
Department of orthotic and prosthetic, Iran university of Medical Sciences, Tehran, Iran.
2Department of physiotherapy, Iran university of Medical Sciences, Tehran, Iran. 3
Musculoskeletal Research Center, Isfahan University of Medical, Isfahan Iran.
4Rehabilitation Management Department, Iran university of Medical Sciences, Tehran, Iran.
5Department of mechanical engineering, Isfahan University of Technology, Isfahan, Iran. 6
University of Nebraska-Lincoln, Lincoln, Nebraska, United States.
*Corresponding Author: poorghasem@rehab.mui.ac.ir, Phone Number: +989136000225
ABSTRACT
Background: The abilities of the subject with stroke during walking differ from that of normal subjects. They have to use various Ankle foot orthosis (AFO) to control the motions of ankle joint and improve their stability. This case study compared kinematic and kinetic parameters of a stroke subject while walking with plastic and Carbon AFO. Moreover, the gait of stroke subject was compared with that of a matched normal subject.
Method: A normal and a stroke subjects were recruited in this study. A motion analysis system (Qualysis) was used to monitor the motions of the joints. Moreover, the force applied on the leg was evaluated by a Kistlerforceplate. Result and discussion: The range of motions and moments of the lower limb joints differed significantly from that of normal subject. Although the plantar flexor moment of ankle joint improved by use of orthosis (especially Carbon AFO), none of the orthoses influenced spatiotemporal gait parameter significantly. It seems that plastic AFO increases stability of ankle joint more than that with carbon AFO.
Key words: stroke, motion analysis, ankle foot orthosis
No conflict of interest
INTRODUCTION
Stroke is one of the leading causes of disability throughout the world and is considered to be the second cause of disability and death[1-4]. It affects the performance of upper and lower extremities in one side; depending on the side of brain affected. Hemiplegia is a term used to describe the disability of limb associated with stroke. Decreasing of the walking speed, asymmetry in the gait pattern, muscle weakness, abnormal movement synergies and spasticity have been observed in the subjects with stroke. Moreover, their standing and walking stability are altered
velocity, decreases double limb support andstance duration, improves symmetry of force applied on the limbs, improves step length and decreases body sway during stance phase[10-12].
Pohl et al. observed that a well fitted AFO
orthosis improved the stability of hemiplegic subjects during standing and walking[13]. Esquenazialso emphasized that gait improved following the use of AFO orthosis in individuals with stroke, depending on the time of post injury[11].
However, various designs of AFO orthoses have different effects on the performance of subjects while standing and walking. Gok observed that gait of hemiplegic subjects improved more with metal orthosis compared to plastic AFO, due to its better stabilization during stance phase[12].
In contrast, De Wit et al. reported that although
the effects of AFO on walking ability in stroke subjects was statistically significant, the difference was small to be clinically relevant[14].
Various kinds of AFO orthoses have been designed for stroke subjects.The most commonorthoses are posterior leg spring (PLS) and carbon AFO (CAFO).
It has been indicated that CAFO stores energy during first part of stance phase and releases it during push off[15]. Therefore, it seems that CAFO may be more effective on gait performance in stroke subjects than the commonly used AFO orthosis (PLS). Danielson et al. claimed that the
use of CAFO increased speed and decreased energy cost during walking[15].
In contrast, Slijper showed that using dynamic AFO resulted in longer walking distance and faster stair climbing compared to CAFO[16]. Although there are studies on energy expenditure of subjects walking with CAFO[15,17], there is not enough evidence in literature regarding the difference between walking performances of stroke subjects using CAFO and PLS orthoses. Therefore, the aim of this study was to evaluate the walking ability of stroke subjects while walking with PLS and CAFO.
METHODS
A normal and a post stroke subject were recruited into this study. They were asked to walk on a walking surface plate. Both subjects were matched based on age, height, and weight. The post stroke subject was participated in this study 11 Months after Cerebrovascular Accident (CVA). Ethical approval was obtained from Isfahan University of Medical Science Ethics Committee. Both subjects were asked to sign consent form before data collection. The age, weight and height of stroke subject were 45 years old, 65 kg and 1.64 m, respectively compared to 45 years old, 67 kg and 1.63 m for the normal subject.
Parameters:
Outcome variables included ankle, knee, hip, pelvic, and trunk rang of motions in three planes. Maximum ground reaction force was applied on both legs in three phases. In addition, the moment transmitted through hip, knee and ankle joints and spatio-temporal gait parameters were collected in this study.
Procedure:
For tracing the movements of the subjects, an array of 7 high speed cameras by Qualysis Company was used. Moreover, the force applied on the leg was measured using a Kistler force plate. The force plate data and the motions of the markers were recorded using a Track–manager software (QTM) produced by Qualysis company. The markers were labeled and determined in Track manager and export as 3D files. The subject’s lower body anatomy was reconstructed by visual 3D software produced by C Motion Company. This parameter was also used for calculating the hip, knee, ankle joints angles, during waking. Force plate data were also processed with 3D to calculate the resulting moments of lower limb joints.
two sample t-test with a significant point set at 0.05.
RESULTS
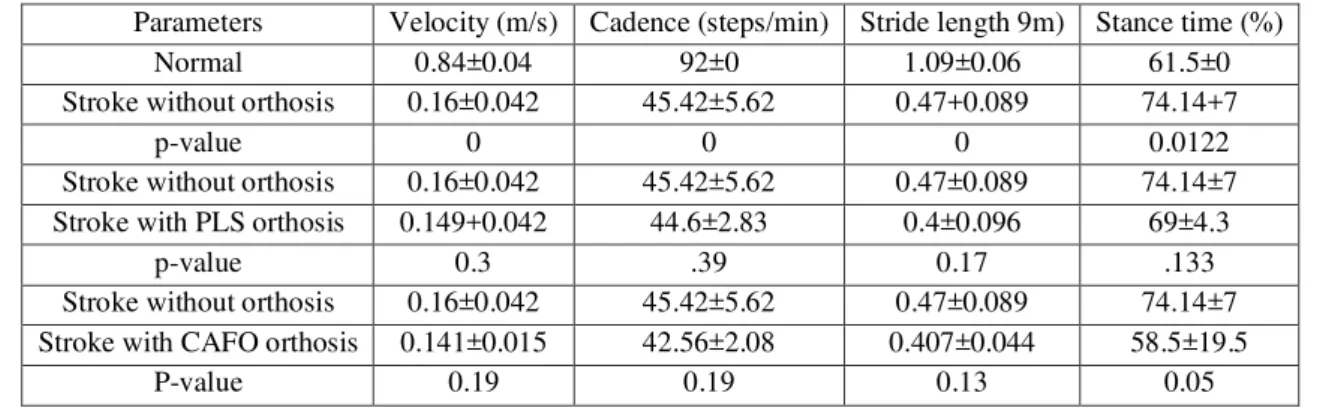
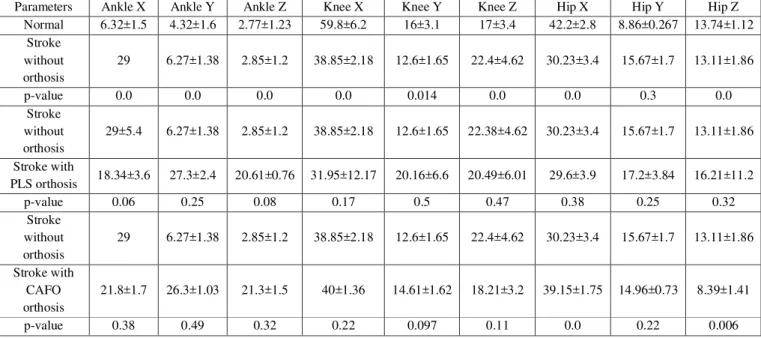
The spatiotemporal gait parameters of the normal and stroke subject are shown in Table 1. There was a significant difference between the mean values of these parameters between the normal and stroke subjects. The walking velocity of the stroke subject in normal walking, walking with PLS, and walking with CAFO were 0.16±0.042 m/s, 0.149±0.042 and 0.141±0.015 m/s, respectively (p > 0.05). The stride length of the stroke subject was 0.47±0.089 and 0.4± 0.096 m, in walking with and without PLS orthosis (Table 1). The percentage of stance phase was also collected in this study. Based on this parameter, there was no difference between walking with and without PLS orthosis. However, CAFO decreased stance phase duration and improved symmetry of walking (p = 0.05). The ranges of motions of ankle, knee, hip and pelvic are shown in Table 2. The range of plantar/dorsi flexion of ankle in the normal subject was 6.32 ± 1.54 degree compared to 22.38±2.7 in stroke subject (p < = 0). The range of motion of the knee joint in sagittal plane was 38.85± 2.18 degree in the stroke subject compared to 59.8±6.2 innormal subject.
Although the range of motion of pelvic in horizontal plane was the same in both subjects, the range of pelvic motions increased significantly in sagittal and transverse planes in the stroke subject (Table 3). The mean of planar flexor moment of ankle joint was 1.33±0.069 Nm/BM in normal subject. There was a significant difference between flexion and extension moments applied on the hip joint of normal and stroke subjects(Table 4).
The gait parameters of stroke subjects were walking with PLS are shown in Tables 2 and 3. The range of motion of ankle joint in the stroke subject was 18.34±3.6 and 22.38±4.62 during walking with and without PLS, respectively. The ankle joint excursion in transverse plane was
18.34±3.6 with walking with PLS and 27.85±1.2 without PLS.
There was no difference between kinematic parameters of the hip joint and pelvic of stroke subject in walking with and without PLS (p > 0.05). The mean value of plantar flexion moment (applied during Push off) in the stroke subject was 0.6±0.086 Nm/BW during normal walking compared to 0.687±0.15 while walking with PLS (p = 0.25). The rotation moment of knee joint decreased, by more than two times, in walking with PLS in contrast to normal walking. The difference between pelvic ranges of motion in three planes between walking with and without PLS was not significant (p > 0.05).
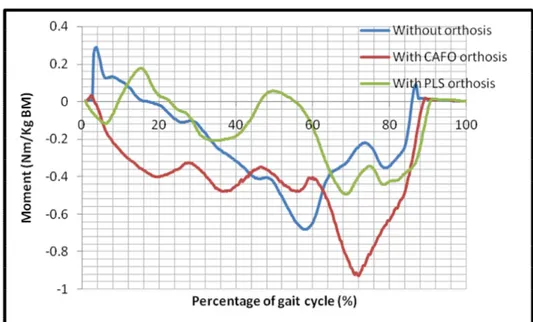
Using PLS influenced the moment transmitted through the hip joint in the sagittal and frontal planes. The stroke subject was also asked to walk with CAFO orthosis. The range of ankle motion in sagittal plane in walking with CAFO was 21.8±1.7, compared to 22.38±2.7 in walking without the orthosis (p = 0.38). The knee joint Flexion/extension range of motion was 38.85±2.16 in normal walking compared to 40±1.36 in walking with CAFO. There was a significant difference between hip joint flexion extension excursion while walking with CAFO and without this orthosis (p = 0). Moreover, CAFO decreased the excursion of the hip joint rotation (p = 0.006). The plantar flexion moment of the ankle joint was 0.978±0.12 Nm/BM in walking with CAFO orthosis compared to 0.6±0.068 NM/BM (p = 0). CAFO also controlled the moment of ankle in transverse plane (Table 4). Figures 1 and 2 show the plantar/dorsi flexion motion and the moment applied on the ankle joint of stroke subject, respectively.
DISCUSSION
This study represents the walking performance of a stroke subject compared to a normal and also the influences of using two different types of AFO on the kinetic and kinematic parameters. As it can be seen from Tables 2 and 3, the stroke subject had more excursions in ankle joint in sagittal plane, decreased range of motion of knee and hip joints, and had an increase in range of motion of pelvic in sagittal plane. Moreover, she had instability of ankle joint in frontal and transverse planes. The main reason was related to weakness of muscles surrounding these joints. The results of the moments of the joints may be indicated that the moments produced by muscles of these joints decreased significantly in contrast to the normal subjects. The stroke subject put her hip and knee joints in an extended posture to increase the stability during stance phase. Use of PLS controlled the motion of paralyzed ankle joint, especially in sagittal plane.However, it did not influence the moment of ankle joint significantly. This may mean that the rigidity of this orthosis was not enough to improve the moments required for a comfortable walking. In contrast, the use of CAFO increased the plantar flexor moment of the ankle joint during push off which improved the abilities of the subject. It should be emphasized that the spatiotemporal gait parameters of the stroke subject walking with CAFO did not differ significantly from that with PLS.
The results of this case study are different from the finding of Danielson et al. He showed that the walking speed of stroke subjects increased by more than 20% in walking with AFO[15,17]. Although the energy consumption was not measured in the present study, it is possible that the ability of stroke subjects during long time walking with CAFO increased due to its effect on plantar flexor moment of the ankle joint. The results of the present study did not support the finding of Danielson et al. who showed that use of
CAFO increased speed of walking[15].
Based on the results of this study, it appears that the PLS orthosis stabilized the ankle joint better than the CAFO. This finding may support the
results of Slijper that most of stroke subjects felt more confident with traditional design (dynamic AFO) than with CAFO[16]. They mentioned that this parameter is more important than speed and distance walked. There are limitations to the present study. This is a case study, therefore, it is difficult to generalize the findings. As a result, future studies with larger sample size should be conducted to authenticate the present findings.
CONCLUSION
The results of this case study showed that subject with stroke has inability to walk efficiently. The use of PLS orthosis did not influence the performance of the subjects. However, CAFO improved plantar flexion moment of ankle joint and symmetry of walking. The results of this study should be used with caution as it is only a case study.
ACKNOWLEDGEMENT:
The authors of this article would like to thank the subject participated in this study. We also would like to thank Dr Mohammad JafarSedigh (Associate Professor of Tehran University, Mechanic Department) for his support and advice regarding designing of the orthosis.
REFERENCES:
1. Wu X, Zhu B, Fu L, Wang H, Zhou B, Zou S, et al. Prevalence, incidence, and mortality of stroke in the chinese island populations: a systematic review. PLoS One. 2013;8(11):e78629.
2. Azarpazhooh MR, Shahripour RB, Kapral MK, Mokhber N, Shoeibi A, Farzadfard MT, et al. Incidence of first ever stroke during Hajj ceremony. BMC Neurol. 2013;13(1):193. 3. Bjorn-Mortensen K, Lynggaard F, Pedersen
ML. Incidence of Greenlandic stroke-survivors in Greenland: a 2-year cross-sectional study. Int J Circumpolar Health. 2013;72:22626. 4. Correia M, Magalhaes R, Silva MR, Matos I,
survival in a community-based study. Cerebrovasc Dis Extra. 2013;3(1):137-49. 5. Verma R, Arya K, Sharma P, Garg R.
Understanding gait control in post-stroke: Implications for management. Journal of bodywork and movement therapies. 2012;16(1):14-21.
6. Perry J, Garrett M, Gronley J, Mulroy S. Classification of walking handicap in the stroke population. Stroke. 1995;26(6):982-9. 7. Chen G, Patten C, Kothari D, Zajac F. Gait
differences between individuals with post-stroke hemiparesis and non-disabled controls at matched speeds. Gait & posture. 2005;22(1):51-6.
8. Patterson KK, Parafianowicz I, Danells CJ, Closson V, Verrier MC, Staines WR, et al. Gait asymmetry in community-ambulating stroke survivors. Arch Phys Med Rehabil. 2008 Feb;89(2):304-10.
9.Jørgensen HS, Nakayama H, Raaschou HO, Olsen TS. Recovery of walking function in stroke patients: the Copenhagen Stroke Study. Archives of physical medicine and rehabilitation. 1995;76(1):27-32.
10. Blaya JA, Herr H. Adaptive control of a variable-impedance ankle-foot orthosis to assist drop-foot gait. Neural Systems and Rehabilitation Engineering, IEEE Transactions on. 2004;12(1):24-31.
11. Esquenazi A, Ofluoglu D, Hirai B, Kim S. The effect of an ankle-foot orthosis on temporal
spatial parameters and asymmetry of gait in hemiparetic patients. PM&R. 2009;1(11):1014-8
12. Gök H, Küçükdeveci A, Altinkaynak H, Yavuzer G, Ergin S. Effects of ankle-foot orthoses on hemiparetic gait. Clinical rehabilitation. 2003;17(2):137-9.
13. Pohl M, Mehrholz J. Immediate effects of an individually designed functional ankle-foot orthosis on stance and gait in hemiparetic patients. ClinRehabil. 2006 Apr;20(4):324-30. 14. De Wit DC, Buurke JH, Nijlant JM, Ijzerman
MJ, Hermens HJ. The effect of an ankle-foot orthosis on walking ability in chronic stroke patients: a randomized controlled trial. ClinRehabil. 2004 Aug;18(5):550-7.
15. Danielsson A, Sunnerhagen KS. Energy expenditure in stroke subjects walking with a carbon composite ankle foot orthosis. J Rehabil Med. 2004 Jul;36(4):165-8.
16. Slijper A, Danielsson A, Willen C. Ambulatory Function and Perception of Confidence in Persons with Stroke with a Custom-Made Hinged versus a Standard Ankle Foot Orthosis. Rehabil Res Pract. 2012;2012:206495.
17. Danielsson A, Carin W, Katharina S. Comparison of energy cost of walking with and without a carbon composite ankle foot orthosis in stroke subjects. 13th ISPO World Congress; 10-15 May; Leipzig, Germany2010.
Tables:
Parameters Velocity (m/s) Cadence (steps/min) Stride length 9m) Stance time (%)
Normal 0.84±0.04 92±0 1.09±0.06 61.5±0
Stroke without orthosis 0.16±0.042 45.42±5.62 0.47+0.089 74.14+7
p-value 0 0 0 0.0122
Stroke without orthosis 0.16±0.042 45.42±5.62 0.47±0.089 74.14±7
Stroke with PLS orthosis 0.149+0.042 44.6±2.83 0.4±0.096 69±4.3
p-value 0.3 .39 0.17 .133
Stroke without orthosis 0.16±0.042 45.42±5.62 0.47±0.089 74.14±7
Stroke with CAFO orthosis 0.141±0.015 42.56±2.08 0.407±0.044 58.5±19.5
P-value 0.19 0.19 0.13 0.05
Parameters Ankle X Ankle Y Ankle Z Knee X Knee Y Knee Z Hip X Hip Y Hip Z Normal 6.32±1.5 4.32±1.6 2.77±1.23 59.8±6.2 16±3.1 17±3.4 42.2±2.8 8.86±0.267 13.74±1.12
Stroke without orthosis
29 6.27±1.38 2.85±1.2 38.85±2.18 12.6±1.65 22.4±4.62 30.23±3.4 15.67±1.7 13.11±1.86
p-value 0.0 0.0 0.0 0.0 0.014 0.0 0.0 0.3 0.0
Stroke without orthosis
29±5.4 6.27±1.38 2.85±1.2 38.85±2.18 12.6±1.65 22.38±4.62 30.23±3.4 15.67±1.7 13.11±1.86
Stroke with
PLS orthosis 18.34±3.6 27.3±2.4 20.61±0.76 31.95±12.17 20.16±6.6 20.49±6.01 29.6±3.9 17.2±3.84 16.21±11.2
p-value 0.06 0.25 0.08 0.17 0.5 0.47 0.38 0.25 0.32
Stroke without orthosis
29 6.27±1.38 2.85±1.2 38.85±2.18 12.6±1.65 22.4±4.62 30.23±3.4 15.67±1.7 13.11±1.86
Stroke with CAFO orthosis
21.8±1.7 26.3±1.03 21.3±1.5 40±1.36 14.61±1.62 18.21±3.2 39.15±1.75 14.96±0.73 8.39±1.41
p-value 0.38 0.49 0.32 0.22 0.097 0.11 0.0 0.22 0.006
Table 2: The range of motions of ankle, knee and hip joints of normal and stroke subject
Parameters Pelvic X Pelvic Y Pelvic Z
Normal 7.3± 0.47 14.6±3.89 8.25±0.86
Stroke without orthosis 18.93±2.7 15.33±7.9 31.63±2.79
p-value 0.45 0.0 0.0
Stroke without orthosis 18.93±2.7 15.33±7.9 31.63±2.79 Stroke with PLS orthosis 16.18± 16.23± 29.84±3.5
p-value 0.46 0.432 0.21
Stroke without orthosis 18.93±2.7 15.33±7.9 31.63±2.79
Stroke with CAFO
orthosis 27.24±3.2 15.47±2.56 27.65±3.9
p-value 0.14 0.48 0.11
Table 3: The range of motion of pelvic of normal and stroke subject
Parameters Ankle
X Ankle Y Ankle Z Knee X Knee Y Knee Z Hip X1 Hip X2 Hip Y Hip Z
Normal 1.33± 0.067 0.282±. 046 0.292+.0 129 0.357±0. 118 0.705±0. 02 0.33±0.0 24 0.525±0. 193 0.956±0 .3 1.55±0.1 8 0.275±0. 03 Stroke without orthosis 0.6±.0 86 0.2±.02 6 .029±0.0 14 0.13±0.0 23 0.223±0. 038 0.182±0. 009 0.267±0. 029 0.55±0. 19 0.512±0. 048 0.155±0. 028
p-value 0 0.03 0 0.02 0 0.001 0.05 0.036 0 0.001
Stroke without orthosis 0.6±.0 86 0.2±.02 6 0.029±0. 014 0.13±0.0 23 0.223±0. 038 0.182±0. 009 0.267±0. 029 0.55±0. 19 0.512±0. 048 0.155±0. 028 Stroke with PLS 0.687 ±0.15 0.11±0.
018 0.2±0.23
Table 4: The moments of leg joints of normal and stroke subject
Figure 1: The ankle motion in sagittal plane in various conditions
Figure 2: The moments applied on the ankle joint in sagittal plane in various conditions
orthosis
p-value 0.25 0.008 0.14 0.26 0.22 0.0 0.0 0.037 0.04 0.22
Stroke without orthosis
0.6±.0 86
0.2±.02 6
0.029±0. 014
0.13±0.0 23
0.223±0. 038
0.182±0. 009
0.267±0. 029
0.55±0. 19
0.512±0. 048
0.155±0. 028
Stroke with CAFO orthosis
0.978 ±0.12
0.3±0.0 2
0.06±0.0 16
0.146±0. 037
0.33±0.0 36
0.154±0. 023
0.4±0.03 3
0.28±0. 016
0.69±0.1 9
0.071±0. 02