142 LETTERSTOTHEEDITOR
1On behalf of The Change Pain Latin America Advisory
Panel: ArgeliaLara-Solares,José AlbertoFlores Cantisani, César Amescua-García, María del Rocío Guillén Nú˜nez, AzizaJreigeIskandar,PatriciaBonilla,OsvandréLech, Dur-val Campos Kraychete, María Antonieta Rico, John Jairo Hernández-Castro,FrantzColimon,CarlosGuerrero,William
Delgado Barrera, Manuel Sempértegui Gallegos, María Berenguel Cook, João Batista Santos Garcia, Concepción PérezHernández.
6March2013
http://dx.doi.org/10.1016/j.bjane.2013.03.004
Contraction
versus
contracture
and
centronuclear
myopathy
versus
central
part
myopathy
in
malignant
hyperthermia
DearEditor,
We read with great interest the review article by Cor-reiaetal.‘‘Malignanthyperthermia:clinicalandmolecular aspects’’1 (Hipertermia maligna: aspectos moleculares e clínicos)andwouldliketocommentonsomeaspects.
In the section ‘‘Malignant hyperthermia’’, item ‘‘Contraction to exposure to halothane-caffeine (TCHC) Test’’,Correia etal. use theterm ‘‘contraction’’instead oftheoriginalterm‘‘contracture’’.Thetest fordiagnosis of susceptibilityto malignanthyperthermia (MH) is based onanabnormalcontractureresponseafter administration ofcaffeine/halothane, andnotonthenormalresponseof muscle contraction after electrical stimulation, which is appliedthroughoutthetesttoproveviabilityofthemuscle fragment tested. Fig. 1 shows the difference between contractionandcontractureinthechartofapositivetestin apatientsusceptibletoMH.Thus,thenomenclatureshould be‘‘contracturetest’’ in Englishandteste decontratura inPortuguese.2---4
Alsointhissubsection,weemphasizethatthecutoff lev-elsofTCHCcitedcorrespondtovaluesusedintheU.S.group ofHM (MHAUS --- www.mhaus.org)protocol. Moreover,the protocoloftheEuropeanMHGroup(EMHG---www.emhg.org) differs fromthe U.S. onein additional aspectsthat were notmentioned,suchasthenumberoffragmentstested(six intheU.S. andfourin theEuropean protocol),halothane administration(singledoseof3%intheU.S.andan increas-ingdosefrom0.5%to3%intheEuropeanprotocol)andfinally thecutoff, whichis 0.2gtoforhalothane2%and0.2gfor caffeine2mmintheEuropeanprotocol.5,6
UnlikethatnotedbyCorreiaetal.,inBraziltheCedhima (CenterfortheStudy,DiagnosisandResearchforMalignant Hyperthermia),Escola Paulista de Medicina, Universidade FederaldeSãoPaulo(UNIFESP)usestheEuropeanMHgroup protocolforinvitromusclecontracturetesting(IVCT).4
In the same section ‘‘Malignant hyperthermia’’, item ‘‘Treatment’’,Correiaetal.includeasanindicated mea-surethe‘‘Replacementofanesthesiacircuitbyothercircuit uncontaminated by anesthetic agent’’. It is important to emphasizeherethatthereisnoindicationforthismeasure duringthetreatmentofacrisis,butonlyinthepreparation oftheanestheticmachineforanesthesiainapatientwitha historyofHM.AtthetimeofaMHcrisiswemust‘‘disconnect thevaporizer,butwithnowasteoftimechangingthe cir-cuitor the anesthetic machine’’.7 In ‘‘Dantrolene’’ item,
although Correiaetal. state thatthe modernclinical use ofdantroleneisrestrictedtomalignanthyperthermia,this drugisstillemployedinthemanagementofspasticity.8
Furthermore,themaintenanceofdantrolenefor24---48h aftertheinitialtreatmentofHMcrisisisimportanttoavoid
1 min 0.6 g
0.5% 1%
Figure1 Invitromusclecontracturetest(IVCT)inresponse
tohalothane.Thetwolowerarrowsindicatethetimeatwhich
thedrugwasadded.Theupperarrowindicatesthelinesthat
correspondtomusclecontractionstriggeredbyelectrical
stim-ulation.Thelateraldoublearrowindicatestheascensionofthe
baseline,whichcorrespondstoanabnormal muscle
LETTERSTOTHEEDITOR 143
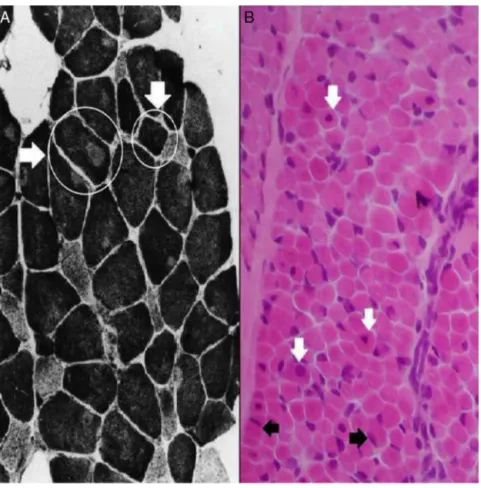
Figure2 Cross-sectionalhistologicalsectionsofstriatedmuscle(freezing).(A)Miopatiadapartecentral,orcentralcore
myopa-thy:thehorizontalarrowindicatesamusclefiberwithunmarked centralcirculararea(core);theverticalarrowdepictsafiber
withhomogeneous normalmarking; histochemicalreaction withNADH. (B)Centronuclearmyopathy: Whitearrows show fibers
withcentralnucleus,andblack arrowsshowfibers withnormalpositionofthenucleus,justbelowthecytoplasmic membrane
(subsarcolemmal);hematoxylinandeosinstain.
relapses; however,in adosage of1mg/kg every4---8h, or continuouslyat0.25mg/kg/h(or6mg/kg/d).9
In the section ‘‘RYANODYNE RECEPTORS (RYRs)’’’, in ‘‘Correlated channelopathies’’ item,the term doenc¸a do núcleocentral appears twice asa translation of ‘‘central coredisease’’.However,thesuggestedtranslationinto Por-tuguese for central core myopathy would bemiopatia da parte central (C05.651.575.300 C10.668.491.550.300), as recommended by the site Descriptors in Health Sciences (http://decs.bvs.br/), under the Unified Medical Lan-guage System (http://www.nlm.nih.gov/research/umls/). Thisdistinctionisimportantbecause,amongotherclinical andmutationalassociated differences,thehistopathology is distinct, as can be seen in Fig. 2. Fig. 2A depicts the appearance of miopatiaor doenc¸ada partecentral (cen-tralcorediseaseorCCD):Thereisacentralmarkingflawin oxidativehistochemicalreactions(suchasSDHandNADH), thankstotheabsenceofmitochondria.10Ontheotherhand, Fig.2Bdepictstheappearanceofcentronuclearmyopathy (i.e.,miopatiacentronuclear),inwhichthenucleusassumes acentralplacein themusclefiber,while usuallyit would occupyasubsarcolemmalposition,i.e.,justbelowthe cyto-plasmicmembrane.11
References
1.Correia AC, Silva PC, da Silva BA. Malignant hyperther-mia: clinical and molecular aspects. Rev Bras Anestesiol. 2012;62:820---37.
2.EllisFR,HalsallPJ,OrdingH,etal.Aprotocolforthe investiga-tionofmalignanthyperpyrexia(MH)susceptibility.BrJAnaesth. 1984;56:1267---9.
3.Larach MG, for the North American Malignant Hyperther-miaGroup.Standardizationofthecaffeinehalothanemuscle contracturetest.AnesthAnalg.1989;69:511---5.
4.SilvaHCA.Biópsiaetestedecontraturamuscular.Rev Neuro-cienc.2005;13:63---4.
5.LitmanRS, RosenbergH.Malignanthyperthermia:update on susceptibilitytesting.JAMA.2005;293:2918---24.
6.UrwylerA,DeufelT,McCarthyT,etal.Guidelinesformolecular geneticdetectionofsusceptibilitytomalignanthyperthermia. BrJAnaesth.2001;86:283---7.
7.GlahnKP,EllisFR,HalsallPJ,etal.Recognizingandmanaging amalignanthyperthermiacrisis:guidelinesfromtheEuropean MalignantHyperthermiaGroup.BrJAnaesth.2010;105:417---20.
8.KhederA,NairKP.Spasticity:pathophysiology,evaluation,and management.PractNeurol.2012;12:289---98.
144 LETTERSTOTHEEDITOR
AdamMP,editors.Genereviews.Seattle:Universityof Wash-ington;1993---2003[Internet].
10.Jungbluth H. Central core disease. Orphanet J Rare Dis. 2007;2:25.
11.JungbluthH,Wallgren-PetterssonC,LaporteJ.Centronuclear (myotubular)myopathy.OrphanetJRareDis.2008;3:26.
HelgaCristinaAlmeidaDaSilva∗,PamelaVieiraDe
Andrade, JoséLuizGomesDoAmaral
EscolaPaulistadeMedicina,UniversidadeFederaldeSão Paulo(Unifesp),SãoPaulo,SP,Brazil
∗Correspondingauthor.
E-mail:halsilva@uol.com.br(H.C.AlmeidaDaSilva). 27February201310June2013