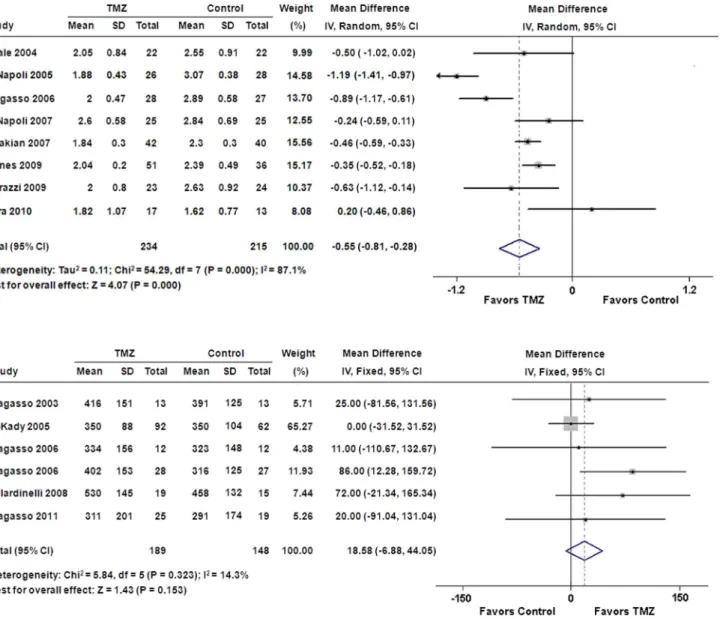
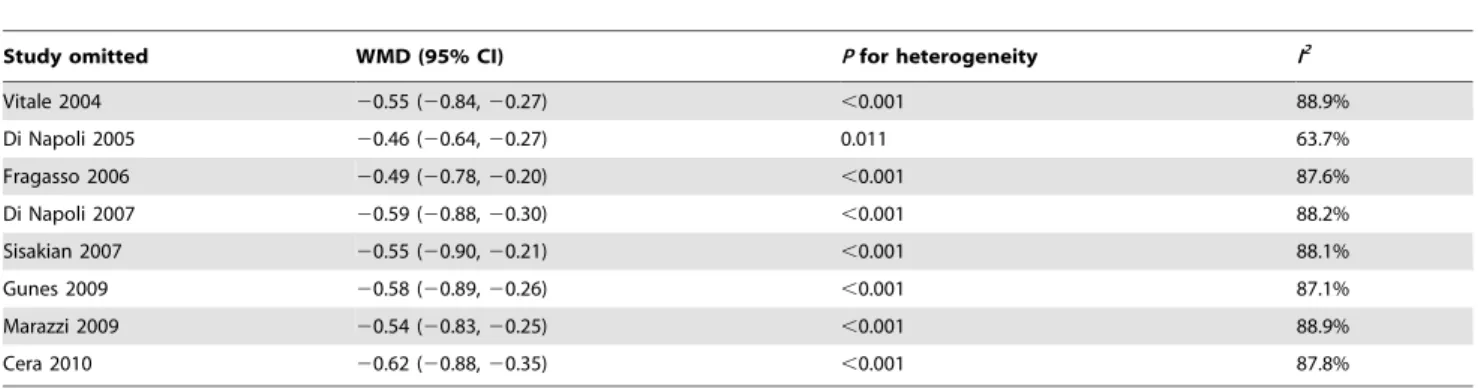
Is treatment with trimetazidine beneficial in patients with chronic heart failure?
Texto
Imagem
Documentos relacionados
For Axis 1 - Target validation and biomarker research (efficacy and safety), the main aims are the: a) Reclassification of tumours on the molecular level; b) Identification of
Conforme podemos perceber com o resultado do questionário e indo de encontro a vários autores, mesmo não sendo o total das entidades, grande parte tem noção que inovar
LVEDDi: left ventricular end-diastolic diameter indexed to body surface area; LVEDD/LVWTd: ratio between left ventricular end-diastolic diameter and left ventricular
RESUMO - Sementes de três cultivares de soja foram submetidas a testes de germinação, tetrazólio, frio, envelhecimento artificial, condutividade elétrica e emergência das plântulas
Eles estudaram separadamente os três componentes da graduação histológica de Bloom&Richardson em 1262 pacientes com carcinoma ductal invasivo e mostraram que os
Cardiac structure and functions - As shown in Table 2, patients with SCA had higher indexes of left ventricular systolic and diastolic diameter, left ventricular wall
Objective: We investigated the agreement and correlation between left ventricular ejection fraction (LVEF), end- diastolic volume (EDV), and end-systolic volume (ESV)
BSA = body surface area, HR = heart rate; 2DE = two-dimensional echocardiography, LVEDV = left ventricular end-diastolic volume; LVESV = left ventricular
