JPediatr(RioJ).2014;90(2):209---212
www.jped.com.br
LETTERS
TO
THE
EDITOR
International
collaborative
research
for
pediatric
and
neonatal
lung
injury:
the
example
of
an
ESPNIC
initiative
to
validate
definitions
and
formulate
future
research
questions
夽Pesquisa
colaborativa
internacional
sobre
lesão
pulmonar
pediátrica
e
neonatal:
exemplo
de
uma
iniciativa
da
ESPNIC
para
validar
definic
¸ões
e
formular
questões
de
pesquisas
futuras
DearSir,
An interesting review of acuterespiratory distress(ARDS) definitionshasbeenrecentlypublishedintheJornalde Pedi-atria, focusingon actual needs in terms of research and clinicalcareofpediatricARDS.1
Unfortunately,timingpreventedtheconsiderationofan importantstepforwardinthisfield.TheEuropeanSociety forPediatricandNeonatalIntensiveCare(ESPNIC),together withsomemembersoftheoriginalARDSTaskForce,haveset upaninternationalcollaborativeprojecttovalidatethenew Berlindefinitionforinfantsandtoddlers.2Thisprojectisthe
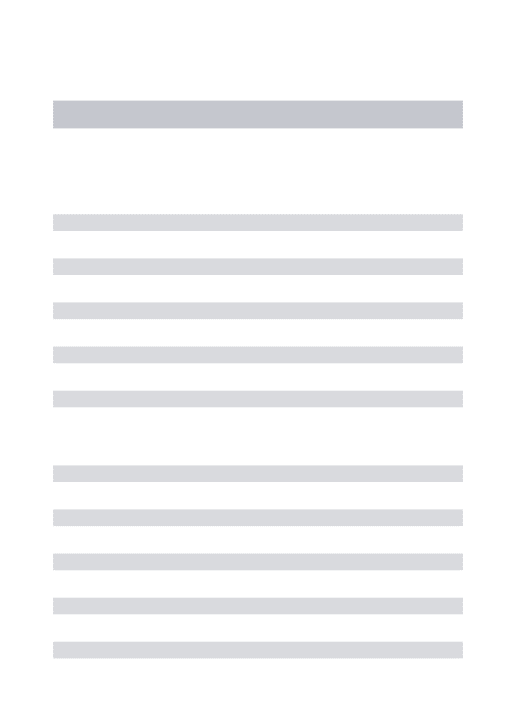
firstinitiativelinkingdifferentpediatricintensivecareunits (PICU)inordertoreachenoughstatisticalpowertoaddressa specificresearchneed.Figure1showstheESPNICnetforthis project.Indeed,asFiorettoetal.summarized,1nospecific
pediatricvalidationhadeverbeenconducted,eventhough somechildrenwereincludedintheoriginalARDSdefinition proposedbyAshbaughetal.in1967.3
Fiorettoetal.described severalpossible limitationsof theBerlindefinition:however,someofthepointsraisedby theseauthorsshouldnotbeconsideredasalimitation,since the newBerlin definitionis not supposed to be a predic-tivetool,butratheraframeworktodefineasyndromefor epidemiology,clinicalcare,andresearch.
夽 Pleasecitethisarticleas:DeLucaD,KneyberM,Rimensberger
PC.Internationalcollaborativeresearchforpediatricandneonatal lunginjury:theexampleofanESPNICinitiativetovalidate defi-nitionsandformulatefutureresearchquestions.JPediatr(RioJ). 2014;90:209---11.
Inaddition,concernswereexpressedregardingthe appli-cationofthenewBerlincriteriatothepediatricpopulation, as there were no children in their original development population.4,5 This isthe reasonwhythe Respiratory
Fail-ureSectionofESPNICstartedtheabove-mentionedproject to evaluate the reliability of the new Berlin definition in a homogeneous and adequately large pediatric popu-lation. The project focused on the early pediatric age (range: 30 days to 18 months), since especially at this age, the syndrome is distinctly different from ARDS in adults.2,6Infact,infantsandtoddlerspresentpeculiarities
regardinglungdevelopment,respiratorysystemmechanics, andco-morbidities, whichareresponsible forthepeculiar epidemiologyandprognosisofARDSinthesepatients.6
ThemainresultsdemonstratedthatthenewBerlin def-initionhasthe samereliabilityboth for the pediatricand adultpatientsintermsofmortalityandneedfor extracor-poreallife support.2 To aid the clinical applicationof the
definition,asetofchestX-rayswithaninterpretationguide andalistofARDSriskfactors,asestimatedbyresearchers participatinginthiscollaborativeeffort,wereestablished. Botharepractical tools thathave proventobehelpful in clinicalpracticeandresearch.2,4,7,8
However,the ESPNIC collaborative work validating the newBerlincriteriaforpediatricARDSpatientshassome lim-itationsthathavealreadybeen pointedout.2,9Besidesthe
retrospective character of this pediatric validation study, only one of the several secondary variables that have beentestedinadults(i.e.standardizedminuteventilation [(Vecorr) =minute ventilation xworst PaCO2/40])couldbe
tested.2However,othervariables(suchaslungvolume
esti-mation,surfactantamountandactivity,biomarkers)could havebeentested,andthenewBerlindefinitioncouldhave beenmoretailoredtopediatricpatientswithanadequate prospectivestudypopulation.Infact,theMurraylunginjury scorereviewedbyFiorettoelal.hasalreadybeenmodified forpediatricARDS,10butitwasneversubjectedtofurther
validationstudies.Finally,otherpediatricageshadnotbeen considered:whileARDSinadolescentscouldbeconsidered asverysimilartothesyndromeinadults,neonatesdeserve aspecificprojecttodefinethesyndromeanddistinguishit fromotherformsofneonatallunginjury.
Thus,the ESPNICcollaborativework wasan initialand substantialstepforward,anddisseminatedavalidatedARDS definitionforaparticularpediatricpopulation,answeringa specificneedof pediatricintensivists.Clearly,many other questionsremainopen,andtheycanbeaddressedonlywith
210 LETTERSTOTHEEDITOR
Figure1 CentersparticipatingintheESPNICRespiratorySectionprojecttovalidatetheBerlindefinitionofARDSfortheearly
pediatricage.221patientswereenrolled.
similarinternationalcollaborativeprojects.Suchstudiesare needed,giventhecomplexrealityofasyndromewith mul-tiplecausesandco-morbiditiessuchasARDS.Furthermore, itisnecessarytostudylargerpediatricpopulationsinorder toreachanadequatestatisticalpower,sinceARDSis signif-icantlylessfrequentinchildrenandneonatesthaninadult patients.
We are looking forward to proceed with other similar projects in order to answer some of the open questions described above. To do this, and toachieve more repre-sentativeresults,aworldwidecollaborativeworkbetween the Respiratory Failure Section of ESPNIC and other non-Europeanresearchersandclinicalcenterswillbeneeded.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Fioretto JR, de Carvalho WB. Temporal evolution of acute respiratory distress syndrome definitions. J Pediatr (Rio J). 2013;89:523---30.
2.DeLucaD,PiastraM,ChidiniG,TissieresP,CalderiniE,Essouri S, et al. on behalf of the Respiratory Section of the Euro-pean Society for PediatricNeonatal Intensive Care (ESPNIC)
TheuseoftheBerlin definitionforacuterespiratorydistress syndromeduringinfancyandearlychildhood:multicenter eval-uation and expert consensus. Intensive Care Med. 2013;39: 2083---91.
3.AshbaughDG,BigelowDB,PettyTL,LevineBE.Acute respira-torydistressinadults.Lancet.1967;290:319---23.
4.ARDSdefinitiontaskforce.Acuterespiratorydistresssyndrome: theBerlindefinition.JAMA.2012;307:2526---33.
5.FergusonND,FanE,CamporotaL,AntonelliM,AnzuetoA,Beale R,etal.TheBerlindefinitionofARDS:anexpandedrationale, justification,andsupplementarymaterial.IntensiveCareMed. 2012;38:1573---82.
6.Randolph AG. Management of acute lung injury and acute respiratory distress syndrome in children. Crit Care Med. 2009;37:2448---54.
7.AngoulvantF,LlorJ,AlbertiC,KhenicheA,ZaccaruaI,Garel C,etal.Inter-observervariabilityinchestradiographreading fordiagnosingacutelunginjuryinchildren.PediatrPulmonol. 2008;43:987---91.
8.MeadeMO,CookRJ,GuyattGH,GrollR,KachuraJR,BedardM, etal.Interobservervariationininterpretingchestradiographs forthediagnosisofacuterespiratorydistresssyndrome.AmJ RespirCritCareMed.2000;161:85---90.
9.KhemaniRG, Wilson DF,Esteban A, FergusonND. Evaluating the Berlin definition in pediatric ARDS. Intensive Care Med. 2013;39:2213---6.
LETTERSTOTHEEDITOR 211
DanieleDeLucaa,b,∗,MartinKneyberc,d,
PeterC.Rimensbergere
aDivisionofPediatricsandNeonatalCriticalCare,
DepartmentofFAME,SouthParisUniversityHospitals, MedicalCenter‘‘A.Béclére’’---APHP,Paris,France
bInstituteofAnesthesiologyandCriticalCare,Catholic
UniversityoftheSacredHeart,Rome,Italy
cDepartmentofPediatrics,DivisionofPediatricIntensive
Care,BeatrixChildren’sHospital,UniversityMedical CenterGroningen,Groningen,TheNetherlands
dPeri-operativeMedicineandEmergencyMedicine(CAPE),
UniversityofGroningen,Groningen,TheNetherlands
eServiceofNeonatologyandPediatricCriticalCare,
DepartmentofPediatrics,UniversityHospitalofGeneva, Geneva,Switzerland
∗Correspondingauthor.
E-mail:[email protected](D.DeLuca).
http://dx.doi.org/10.1016/j.jped.2013.12.003
ARDS
definitions
in
children:
one
step
forward
夽Definic
¸ões
da
SDRA
em
crianc
¸as:
um
passo
adiante
DearSir,
It waswith greatinterest and pleasure that we read the Letter tothe Editor entitled ‘‘International collaborative researchforpediatricandneonatallunginjury:theexample of an ESPNIC initiative to validate definitions and formu-latefutureresearchquestions’’byDanieleDeLucaetal.1
The authors commented that the European Society for Pediatric and Neonatal Intensive Care (ESPNIC) published the first validation of the acute respiratory distress syn-drome (ARDS) Berlin Definition (BD) in early childhood.2
MembersoftheESPNICRespiratorySectionperformeda ret-rospective international(Italy,Spain, France,Austria, and theNetherlands)multicenterstudyincludingchildrenaged between30daysand18monthswithARDSaccordingtothe American-EuropeanConsensusConference(AECC)criteria.3
Itelegantlyaddressesourconcerns onthe applicabilityof BDinpediatricswhenwedescribed theevolutionofARDS definitions.4
A time lapse between the two publications prevented exact connections between them; nowis the opportunity todoso.TheBD5foradultsandchildrenisanadvance,in
thesensethatARDSstratificationisimportantfordiagnosis andtreatment.However,itwasobvious thatpediatricians workinginclinicalorbasicresearchneededtovalidatethe new datain children. The work performed by The Respi-ratory Section of ESPNIC2 enrolled 221 children, median
age6months(range2-13months),whichwerecategorized according to the two definitions. The authors found very interesting andimportantresults. Applying AECC,36 chil-drenwereclassifiedasALIand185asARDS,withmortality ratesof13.9%and17.8%,respectively.Conversely,36were classifiedasmild,97 asmoderate, and88assevereARDS
DOIofreferstoarticle:http://dx.doi.org/10.1016/j.jped.2013. 12.003
夽
Please cite this article as: Fioretto JR, de Carvalho WB. ARDSdefinitionsinchildren:onestepforward.JPediatr(RioJ). 2014;90:211---2.
when applyingthe BD. The BD described the clinical sit-uationbetterthan AECC, withsimilarresults publishedin adults.Also,themainoutcomesweresignificantlydifferent onlyfor severe ARDS; mortalitywas13.9% for mild ARDS, 11.3%formoderateARDS,and25%forsevereARDS.Theydid notfindsignificantdifferencesbetweenmildandmoderate classes.However,theinclusionofaseverecategoryinthe BDhelpedtoincreaseitsvalidity.Despitenotaimedat iden-tifyingrisk factors andtheir association withARDS, some werepresented (sepsis, near-drowning, congenital immu-nodeficiencies,thoracic trauma, etc.). As expected, they aredifferent than those in the adult population. A prop-erlydesigned study is therefore necessary toaddress this issue.TheauthorsconcludedthatthenewARDS definition correctlyadjustsandisabletodefinethesyndromein its population, subdividing it into mild/moderate and severe ARDS.
Some limitations were addressed. Firstly, the number of patients included was not large. This is a difficulty in all pediatric studies, as populations of children in inten-sivecare aremuchsmallerthanthoseofadults.Secondly, clinicaldatawasnotcorrelatedwithlungmorphology. How-ever,lungbiopsyisnotcommonlyperformedincriticallyill children.
The Brazilian Pediatric ARDS Study Group6 performed
a prospective, multicentre cohort study from March to Septemberof2013,whichaimed:(1)toevaluatethe preva-lenceofARDS;(2)todetermineriskfactorsforARDS;and (3)toevaluatewhethertheuseofBDincriticallyillchildren canbetterdiscriminatetheseverityofthediseasecompared withtheAECCdefinition.Thedistributionandoutcomesof the patients according to the AECC and BD areshown in Table1.
TheBDbetterdiscriminatestheseverityofARDSin chil-drenwhen comparedtothe AECCdefinition, asshown by the incremental increase in mortality rates and reduced number of ventilation-free days in patients with severe ARDS.
In summary, we congratulateDe Luca etal.2 for their