www.jped.com.br
REVIEW
ARTICLE
Effect
of
preterm
birth
on
motor
development,
behavior,
and
school
performance
of
school-age
children:
a
systematic
review
夽
,
夽夽
Rafaela
S.
Moreira
a,b,∗,
Lívia
C.
Magalhães
c,
Claudia
R.L.
Alves
daPrograminHealthSciences:ChildandAdolescentHealth,SchoolofMedicine,UniversidadeFederaldeMinasGerais(UFMG),
BeloHorizonte,MG,Brazil
bDepartamentofPhysicalTherapy,UniversidadeFederaldeSantaCatarina(UFSC),Araranguá,SC,Brazil cDepartmentofOccupationalTherapy,UniversidadeFederaldeMinasGerais(UFMG),BeloHorizonte,MG,Brazil
dDepartamentofPediatrics,FacultyofMedicine,UniversidadeFederaldeMinasGerais(UFMG),BeloHorizonte,MG,Brazil
Received15April2013;accepted27May2013 Availableonline24December2013
KEYWORDS
Prematurebirth; Dexterity; Behavior;Learningdisorders
Abstract
Objectives: to examineand synthesizetheavailable knowledge intheliteratureaboutthe
effectsofpretermbirthonthedevelopmentofschool-agechildren.
Sources: thiswas asystematicreview ofstudies publishedinthepasttenyears indexedin
MEDLINE/Pubmed,MEDLINE/BVS;LILACS/BVS;IBECS/BVS;Cochrane/BVS,CINAHL,Webof
Sci-ence,Scopus,andPsycNETinthreelanguages(Portuguese,Spanish,andEnglish).Observational
andexperimentalstudiesthatassessedmotordevelopmentand/orbehaviorand/oracademic
performanceandwhose target-populationconsisted ofpreterm children aged8to10years
wereincluded.ArticlequalitywasassessedbytheStrengtheningthereportingofobservational
studiesinepidemiology(STROBE)andPhysiotherapyEvidenceDatabase(PEDro)scales;articles
thatdidnotachieveascoreof80%ormorewereexcluded.
Summaryoffindings: theelectronicsearchidentified3,153articles,ofwhich33wereincluded
basedontheeligibilitycriteria.Onlyfourstudiesfoundnoeffectofprematurityonthe
out-comes(twoarticlesonbehavior,oneonmotorperformanceandoneonacademicperformance).
Amongtheoutcomesofinterest,behaviorwasthemostsearched(20articles,61%),followed
byacademicperformance(16articles,48%)andmotorimpairment(11articles,33%).
Conclusion: prematureinfantsaremoresusceptibletomotordevelopment,behaviorand
aca-demicperformanceimpairmentwhencomparedtoterminfants.Thesetypesofimpairments,
whoseeffectsaremanifestedinthelongterm,canbepreventedthroughearlyparental
guid-ance,monitoringbyspecializedprofessionals,andinterventions.
©2013SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Allrightsreserved.
夽 Pleasecitethisarticleas:MoreiraRS,MagalhãesLC,AlvesCR.Effectofpretermbirthonmotordevelopment,behavior,andschool
performanceofschool-agechildren:asystematicreview.JPediatr(RioJ).2014;90:119---34.
夽夽StudyconductedatthePost-GraduationPrograminHealthSciences,FacultyofMedicine,UniversidadeFederaldeMinasGerais.
∗Correspondingauthor.
E-mail:[email protected](R.S.Moreira).
PALAVRAS-CHAVE
Nascimentoprematuro; Destrezamotora; Comportamento; Transtornosde aprendizagem
Efeitodonascimentoprematuronodesenvolvimentomotor,comportamentoe desempenhodecrianc¸asemidadeescolar:revisãosistemática
Resumo
Objetivos: examinaresintetizaroconhecimentodaliteraturasobreosefeitosdonascimento
prematuronodesenvolvimentodecrianc¸asemidadeescolar.
Fontesdedados: revisãosistemáticadeestudosdosúltimos10anosindexadosnasbasesde
dadosMedline/Pubmed;Medline/BVS;Lilacs/BVS;IBECS/BVS;Cochrane/BVS;Cinahl;Webof
Science;Scopus ePsycNET,em trêslínguas (português,espanhol einglês).Foramincluídos
estudos observacionaiseexperimentais queavaliaramo desenvolvimentomotor e/ou
com-portamentoe/oudesempenhoescolarequetinhamcomopopulac¸ão-alvocrianc¸asprematuras
nafaixaetáriadeoitoa10anos.AqualidadedosartigosfoiavaliadapelasescalasSTROBEe
PEDroeutilizou-seainda,comocritériodeexclusão,artigosquenãoatingissemumapontuac¸ão
correspondentea80%oumaisnositensdasreferidasescalas.
Síntesededados: abuscaeletrônicaidentificou3.153artigos,sendoque33foramincluídosa
partirdoscritériosdeelegibilidade.Apenasquatroestudosnãoencontraramqualquerefeito
daprematuridade sobreosdesfechospesquisados(doisartigossobreocomportamento, um
sobredesempenhomotoreumsobredesempenhoescolar).Dentreosdesfechosdeinteresse,o
comportamentofoiomaispesquisado(20artigos/61%)seguidododesempenhoescolar(16/48%)
edosproblemasmotores(11/33%).
Conclusão: crianc¸asprematurassãomaissusceptíveisaprejuízosnodesenvolvimentonasáreas
motoras,decomportamentoededesempenhoescolaremlongoprazoquandocomparadasa
crianc¸asnascidasatermo.Portanto,essesdiferentestiposdeagravos,cujosefeitosse
mani-festam,emlongoprazo,podemserprevenidosprecocementeatravésdeorientac¸ãodospais,
acompanhamentodosprofissionaisespecializadoseintervenc¸ão.
©2013SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Todososdireitos
reservados.
Introduction
Preterm birth has been the subject of concern for fam-ilies, professionals, and healthcare managers, as early detection of its consequences can facilitate therapeutic interventions and minimize future sequelae. Thus, pro-gramswere created tofollow prematureinfants; in most cases, these programs follow the children until the age of 2 years, and are intended primarily for the detec-tion of severe disabilities such as cerebral palsy.1 This
follow-uppolicydoesnotappeartobebasedonevidence, since a small number of premature infants will develop severe sequelae, yet many will have lifelong social lim-itations and restrictions, as they will have mild motor skill,behavior, schoolperformance, and language impair-ments,among others,and they often are notspecifically diagnosed.2
More extensive follow-up programs require time and implyinadditionalcosts.Hospitalizationduringthe neona-talperiodhasahighcost,3butthelong-termeconomicand
social impact of these children’s outcomes in the differ-entsectorsofsocietycannotbeunderestimated.Although preventionandinterventionprogramsdemandahigh short-terminvestment, thecosts relatedtospecial schoolsand socialservicescanbesignificantlyreducedinthelongrun, aswellasratesofschoolfailure.4
Pretermchildrenhaveahistoryofbiological vulnerabil-ityandagreaterriskofdevelopmentalproblems.Manyof thesechildren,considered‘‘apparentlynormal’’,havemore learningdisabilities,aswellasaworsemotorrepertoireand behavioralproblemsthanchildrenbornatterm.5,6Itshould
beconsideredthat,inmanycases,preterminfantsmaybe exposedtomultiplerisks,andthecontextinwhichtheyare insertedcanbevitalforpositiveornegativeeffectsontheir development.7
Research worldwide has shown concern for the long-termeffectsofpretermbirth.This concernshouldalsobe extendedtothedevelopingcountries,suchasBrazil,asthe poor conditions of life can become an aggravating factor forbiologicalvulnerability.4However,therehavebeenfew
nationalstudiesthatinvestigatedthedevelopmentofthese childrenatschoolage.8
Inspiteofthetechnologicaladvancesinneonatologyand increasedsurvivalofpreterminfants,therearestill knowl-edgegaps inthis area.Studiesinvolving preterm children atschoolagehaveimportantlimitations,suchasdifferent assessmenttools;smallandheterogeneoussamples,which arenotrepresentativeofthepopulation;littleorno detail-ing of clinical and sociodemographic characteristics; and inadequatecomparisongroups,amongothers.9,10Thus,the
influenceofperinatalvariablesandthecumulativeeffects of multiple risk factorsduring the courseof development remain unconfirmed. It is essential to know the associa-tion between prematurity and the future performance of preterminfantsinordertoclarifyitspossibleeffectsonthe differentaspectsof thesechildren’slives, suchashealth, education,etc.
Methods
Thepresentstudyisasystematicreviewoftheexisting lit-erature, following the recommendations of the Cochrane Library11 and PRISMA.12 Studies were selected through
an electronic search in MEDLINE/Pubmed; MEDLINE/BVS; LILACS/BVS;IBECS/BVS;Cochrane/BVS;CINAHL;Webof Sci-ence;Scopus;andPsycNETdatabases.Thesearchstrategy of electronic databases included studies published in the past ten years(January, 2002 to February,2012) in three languages(Portuguese,Spanish,andEnglish).
Observational studies (cross-sectional, case-control, and cohort) and experimental studies (randomized con-trolledtrials,randomizedorquasi-randomizedtrials)were included. Literatureor systematic reviews,letters, edito-rials, and case reports were excluded. Only studies that assessedmotordevelopmentand/orbehaviorand/orschool performanceandhadastargetpopulationpretermchildren thatincluded theagerangeof 8to10 yearswere consid-ered.
Thequalityofthearticleswasassessedbythe Strength-eningthereportingofobservationalstudiesinepidemiology (STROBE) and Physiotherapy Evidence Database (PEDro) scales;duetothegreatquantityandvariabilityof method-ologicalqualityofthe identifiedarticles,qualitywasalso usedasanexclusioncriterion.Articlesthatdidnotachieve atleasta scoreof 80%intherequirementsestablishedby thesescaleswerenotincluded.13Thekeywordsusedvaried
accordingtodatabasesearched,andwerechosenafter con-sultingtheMeSHterms:‘‘premature,environment,family, child development, psychomotor performance, dexterity, socioeconomic factors, learning disability, child behavior, andchildbehaviordisorder.’’
The eligibility assessment and article quality analysis were performed by a single independent reviewer. The assessment of methodological quality of the experimen-tal studies wasperformed throughthe PEDro scale,14 and
for observational studies, it was based on the STROBE recommendations.13 The PEDro scale is basedon the
Del-philist, andconsists of 11 items,of which only the item ‘‘specificationofinclusioncriteria’’isnotscored.Thescale items are: subjectinclusion criteria; random assignment; confidentialityofallocation;similarityofgroupsatthe ini-tial stage; blinding of subjects, therapist and evaluator; measurement of at least one key outcome; intention-to-treat analysis; results of statistical comparisons between groups;andreportedmeasures ofvariabilityandprecision ofatleastoneoutcome.Eachcriterionisworthonepoint. Studiesscoringlessthanthreepointsareconsideredtohave lowmethodologicalquality.15,16
The STROBEchecklist hasbeen recentlytranslatedand adaptedtoBrazilianPortuguese.It contains22itemswith features that should be present in the different sections of an article to increase the quality of observational studies. The items help to focus on the quality of the title and abstract. In the introduction, the focus is the context and objectives; in the methodology, it is the studydesign,thecontext,theparticipants,variables,data sources/measurements,bias,samplesize,thequantitative variables,and thestatistical methods used.Inthe results section,thefocusisonthequalityofparticipant descrip-tion,descriptivedata,outcomesandkeyresults,whereas
in thediscussion, the essential items checked are limita-tions,generalization,andinterpretation.This listwasnot developedtoassessthemethodologicalqualityofstudies; however,itiscommonlyusedinBrazilforthispurpose.13,17
Brazilianresearchershave established threecategories to classifythequalityofarticles:A,whenthestudymeets80% ormoreoftheSTROBEcriteria;B,whenitmeets50%to79% ofthe STROBEcriteria, and C,when lessthan 50%of the criteriaaremet.18,19
Fordataextraction,aformwascreated,whichincluded the following variables: study identification (title and authors),yearofpublication,countrywherethestudywas conducted,methodologicaldesign,objectives,samplesize andcharacteristics(gestationalageandbirthweight),ageof subjects,outcomes,assessmenttools,results/conclusions, andSTROBE/PEDroscores.
The present study is part of a larger project enti-tled‘‘Evaluationoftheoveralldevelopmentofschool-age children born prematurely from 2002 and followed-up in theOutpatient Clinicof Children at Risk (Ambulatóriode Crianc¸as de Risco --- ACRIAR) of the Hospital das Clínicas of the Universidade Federal de Minas Gerais’’which was approvedbytheResearchEthicsCommitteeofthe Univer-sidade Federal de Minas Gerais (UFMG), under No. CAAE 0456.0.203.000-11.
Results
Theelectronic searchretrieved3,153 articlesindifferent databases,andonly33wereincludedaccordingtothe eli-gibilitycriteria.Atotalof3,120articleswereexcludedfor variousreasons, suchasrepetitionsindifferentdatabases orthefactthattheywerenotavailableinelectronicmedia ordidnotmeet theeligibilitycriteria, suchasage ofthe children;additionally,articleswithlowmethodologicalrigor wereexcluded
All selected articles were observational studies (25 cohort,threecase-control,fourcross-sectionalstudies,and onewasasecondarydataanalysisfromaprospectivestudy) and obtained a score ≥ 80% in the STROBE scale
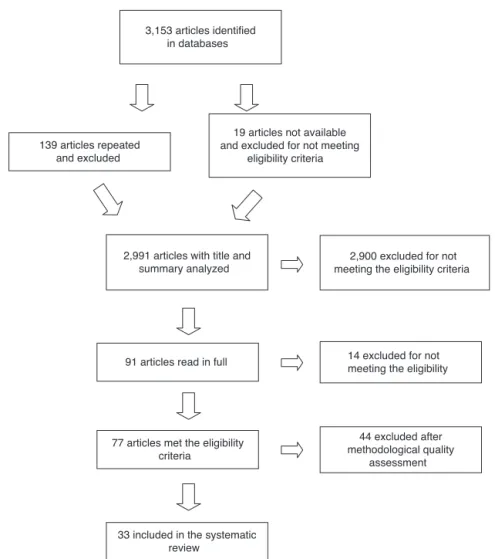
(classi-fication A). No experimental studies with a score > 80% onthePEDroscalewereretrieved.Figure1detailsarticle selection.Theresultsoftheanalyzedoutcomes(schooland motorperformance, aswell asbehavior)were subdivided intotopicsforeaseofunderstanding.
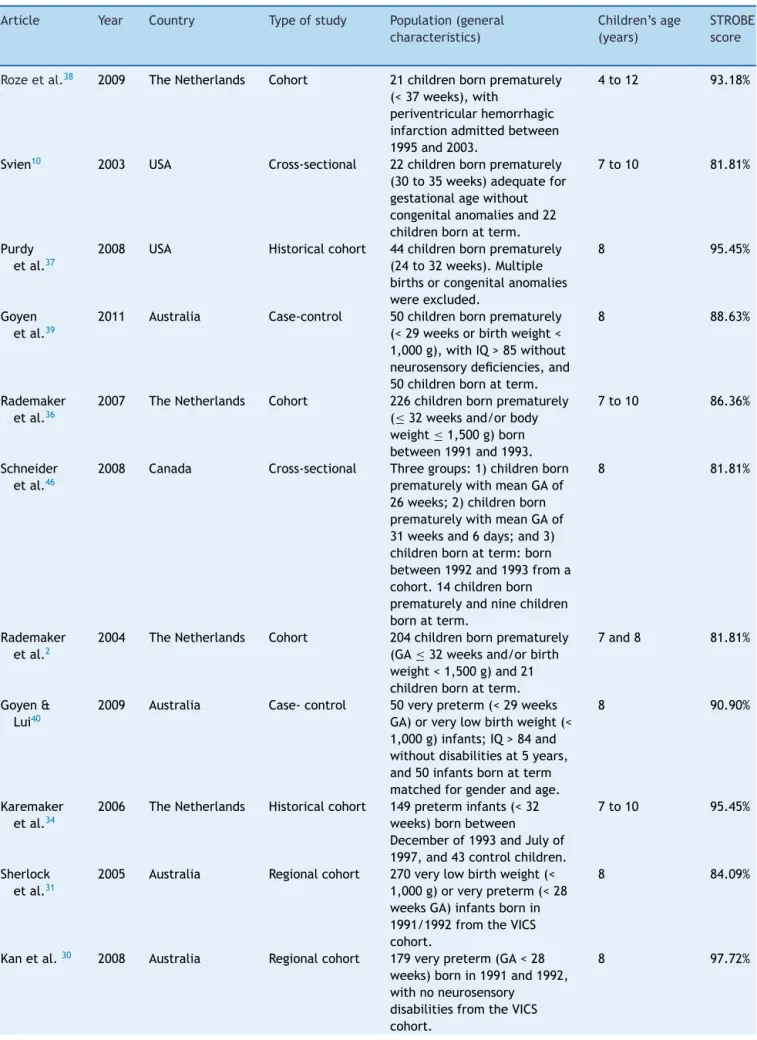
Table 1 presents the general characteristics of the selectedstudies,includingyear andcountrywhere it was conducted, study type, population, age of children, and STROBEscores.
All selected articles were conducted in developed countries:UnitedStates(12articles,36%),Australia(6 arti-cles,18%),the Netherlands(5 articles,15%),Denmarkand France(3articleseach, 9%),Sweden(2 articles,6%),and finallyEnglandandCanada(onearticleeach,3%)(Table1). Manyof theselected studies (14articles, 42%) originated fromlarge,internationallyrecognizedcohorts.
Table1 Generalcharacteristicsofidentifiedstudies,BeloHorizonte,Brazil,2012.
Article Year Country Typeofstudy Population(general
characteristics)
Children’sage
(years)
STROBE score
Rozeetal.38 2009 TheNetherlands Cohort 21childrenbornprematurely (<37weeks),with
periventricularhemorrhagic infarctionadmittedbetween 1995and2003.
4to12 93.18%
Svien10 2003 USA Cross-sectional 22childrenbornprematurely (30to35weeks)adequatefor gestationalagewithout congenitalanomaliesand22 childrenbornatterm.
7to10 81.81%
Purdy etal.37
2008 USA Historicalcohort 44childrenbornprematurely (24to32weeks).Multiple birthsorcongenitalanomalies wereexcluded.
8 95.45%
Goyen etal.39
2011 Australia Case-control 50childrenbornprematurely (<29weeksorbirthweight< 1,000g),withIQ>85without neurosensorydeficiencies,and 50childrenbornatterm.
8 88.63%
Rademaker etal.36
2007 TheNetherlands Cohort 226childrenbornprematurely (≤32weeksand/orbody
weight≤1,500g)born
between1991and1993.
7to10 86.36%
Schneider etal.46
2008 Canada Cross-sectional Threegroups:1)childrenborn prematurelywithmeanGAof 26weeks;2)childrenborn prematurelywithmeanGAof 31weeksand6days;and3) childrenbornatterm:born between1992and1993froma cohort.14childrenborn prematurelyandninechildren bornatterm.
8 81.81%
Rademaker etal.2
2004 TheNetherlands Cohort 204childrenbornprematurely (GA≤32weeksand/orbirth
weight<1,500g)and21 childrenbornatterm.
7and8 81.81%
Goyen& Lui40
2009 Australia Case-control 50verypreterm(<29weeks GA)orverylowbirthweight(< 1,000g)infants;IQ>84and withoutdisabilitiesat5years, and50infantsbornatterm matchedforgenderandage.
8 90.90%
Karemaker etal.34
2006 TheNetherlands Historicalcohort 149preterminfants(<32 weeks)bornbetween Decemberof1993andJulyof 1997,and43controlchildren.
7to10 95.45%
Sherlock etal.31
2005 Australia Regionalcohort 270verylowbirthweight(< 1,000g)orverypreterm(<28 weeksGA)infantsbornin 1991/1992fromtheVICS cohort.
8 84.09%
Kanetal.30 2008 Australia Regionalcohort 179verypreterm(GA<28 weeks)bornin1991and1992, withnoneurosensory
disabilitiesfromtheVICS cohort.
Table1(Continued)
Article Year Country Typeofstudy Population(general
characteristics)
Children’sage
(years)
STROBE score
Guellec
etal.24
2011 France Cohort 2,846preterminfantsbetween 24and32weeksofgestation selectedfromnineregionsof Francein1997,and666bornat termfromtheEPIPAGEcohort.
5and8 88.63%
Chyietal.3 2008 USA Cohort 970moderatelypreterm infants(32to33weeks)and latepreterminfants(34to36 weeks),and13,671children bornattermfromtheEarly ChildhoodLongitudinalStudy Kindergarten
10and11 93.18%
D’Angio etal.32
2002 USA Cohort 132preterminfants(<29 weeks),bornbetween 1985-1987.
0to15 86.36%
Charkaluk etal.1
2011 France Cohort 244preterminfantsbornafter 22to32weeksgestationin 1997,withnodisabilitiesor developmentalimpairment fromtheEPIPAGEcohort.
2to8 86.36%
vanBaar etal.29
2006 TheNetherlands Cohort 34preterminfants(<32 weeks)and34childrenbornat term.
10 81.81%
Msall etal.33
2004 USA Cohort 222preterminfantswithbirth weight<1,251gand
retinopathyofprematurityand noothermalformationsfroma multicentricstudy(CRYO-ROP)
5,5and8 respectively
90.90%
Caseyetal.9 2006 USA Cohort 221preterminfantswithbirth weight≤2,500g,gestational
age≤37weeks,without
severemedicalimpairments, and434controlsfromtheIHDP program.
8 84.09%
Larroque etal.35
2011 France Cohort 1,439preterminfantsbetween 22and32weeks,bornin1997, and327infantsbornatterm fromtheEPIPAGEcohort.
8 84.09%
Kirkegaard etal.6
2006 Denmark Cohort 211pretermand4,897term children.GAwasstratified: 33-36,37-38,39-40,and≥41
weeks,andGAfrom39to40 weeksfromtheAarhusBirth Cohort.
9to11 90.90%
Mathiasen etal.28
2010 Denmark Cohort Alllivebirthsin1988and1989: 118,891pretermorterm children.Population-based study.
0to15 84.09%
Linnet etal.20
2006 Denmark Case-control Allchildrenbornbetween1980 and1994withhyperkinetic disorder;834cases(preterm andlowbirthweight),and 20,100controls.
Table1(Continued)
Article Year Country Typeofstudy Population(general
characteristics)
Children’sage
(years)
STROBE score
Gurka
etal.27
2010 USA Cohort 53latepretermchildren(34to 36weeks)and1,245children bornatterm(37to41weeks) fromtheSECCYDcohort.
4to15 81.81%
Whiteside-Mansell etal.26
2009 USA Longitudinal 728children<37weeksand lowbirthweight(mosthad< 2,000g,butsomechildrenhad between2,001to2,500g) fromtheIHDPprogram.
8 81.81%
Jeyaseelan etal.5
2006 Australia Cross-sectional 45childrenwithextremelylow birthweight(<1,000g)or preterm(GA<27weeks).
7to9 84.31%
Conrad etal.23
2010 USA Cross-sectional 49childrenwithextremelylow birthweight(<1,000g)orvery lowbirthweight(1,000to 1,499g),and55childrenborn atterm.
7to16 81.81%
Purdy etal.44
2013 USA Cohort 45pretermchildrenwithmean GAof28weeks.
8 81.81%
Farooqi etal.43
2007 Sweden Cohort 86pretermchildrenborn before26weeksofgestation between1990and1992,and 86controls.
10to12 88.63%
Grayetal.25 2004 USA Cohort 985Pretermchildren(GA<37 weeks)andbirthweight< 2,500gatbirthfromtheIHDP program.
3.5and8 81.81%
Yuetal.45 2006 USA Dataanalysis 713pretermchildrenwith< 2,500gand<37weeksGA fromtheIHDPprogram.
8 84.09%
Anderson etal.42
2003 Australia Regionalcohort 298childrenwithextremely lowbirthweight(<1,000g)or verypreterm(<28weeksGA). 262controlinfantswithbirth weight>2,499g.
0to8 93.18%
Crombie etal.21
2011 England Cross-sectional 196preterm(<36weeksGA) and/orlowbirthweight(< 2,500g)childrenwere classifiedas‘‘atrisk’’,and 1,704controlinfantswere classifiedas‘‘norisk’’.
9to10 88.63%
Lindström etal.22
2011 Sweden Nationalcohort 67,543pretermchildrenwith GAbetween23and36weeks, and1,113,163bornatterm(> 37weeks).
6to19 81.81%
CRYO-ROP,Cryotherapyfor RetinopathyofPrematurity CooperativeGroup;EPIPAGE,TheEtudeEpidemiologique surlesPetitsAges Gestationnels;IHDP,InfantHealthand DevelopmentProgram; GA,GestationalAge;IQ,intelligencequotient;SECCYD,ChildHealth andDevelopmentStudyofEarlyChildCareandYouthDevelopment;STROBE,StrengtheningtheReportingofObservationalStudiesin Epidemiology;VICS,VictorianInfantCollaborativeStudy.
describethegestationalage at birth, butonly mentioned that the selected children were preterm (< 37 weeks of gestation).The sample size of the studies varied greatly, with a minimum of 14 and maximum of 67,543 preterm childrenevaluated(Table1).
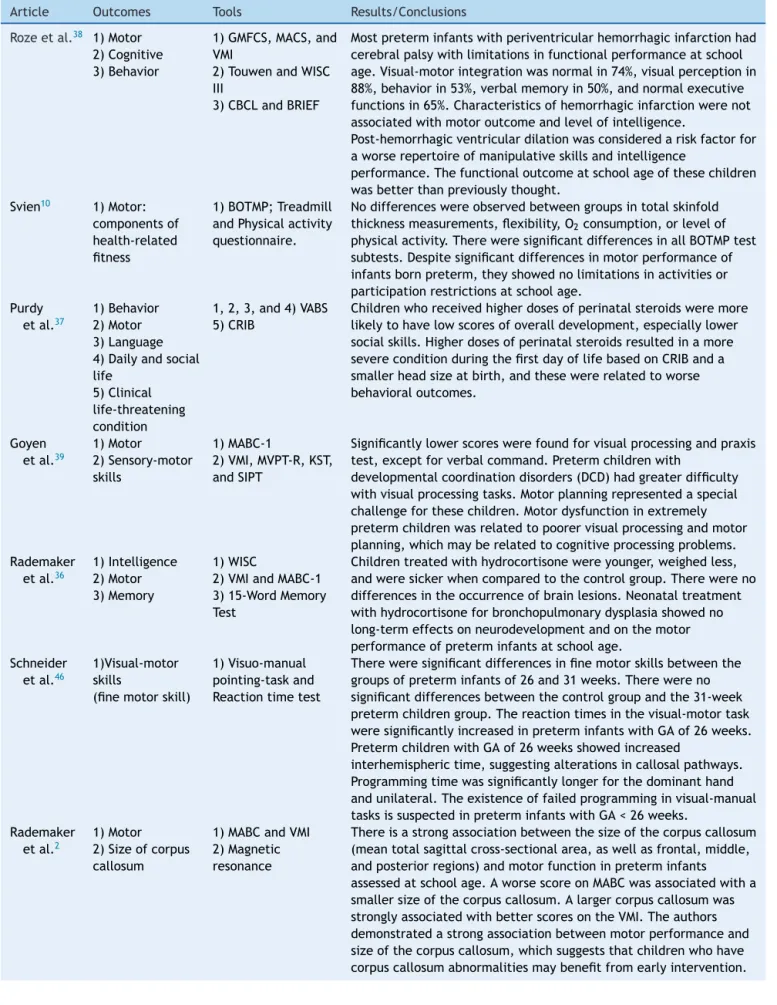
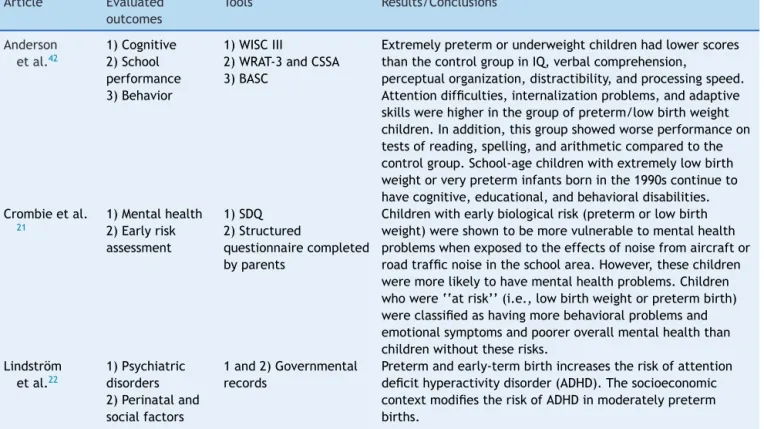
Tables2and3presentthestudiesanalyzedinthisreview, themainoutcomesevaluated,thetoolsused,andtheirmain findings/conclusions.
Table2 Studiesofmotordevelopmentinpreterminfantsandtheirmainfindings,BeloHorizonte,2012.
Article Outcomes Tools Results/Conclusions
Rozeetal.38 1)Motor 2)Cognitive 3)Behavior
1)GMFCS,MACS,and VMI
2)TouwenandWISC III
3)CBCLandBRIEF
Mostpreterminfantswithperiventricularhemorrhagicinfarctionhad cerebralpalsywithlimitationsinfunctionalperformanceatschool age.Visual-motorintegrationwasnormalin74%,visualperceptionin 88%,behaviorin53%,verbalmemoryin50%,andnormalexecutive functionsin65%.Characteristicsofhemorrhagicinfarctionwerenot associatedwithmotoroutcomeandlevelofintelligence.
Post-hemorrhagicventriculardilationwasconsideredariskfactorfor aworserepertoireofmanipulativeskillsandintelligence
performance.Thefunctionaloutcomeatschoolageofthesechildren wasbetterthanpreviouslythought.
Svien10 1)Motor: componentsof health-related fitness
1)BOTMP;Treadmill andPhysicalactivity questionnaire.
Nodifferenceswereobservedbetweengroupsintotalskinfold thicknessmeasurements,flexibility,O2consumption,orlevelof
physicalactivity.ThereweresignificantdifferencesinallBOTMPtest subtests.Despitesignificantdifferencesinmotorperformanceof infantsbornpreterm,theyshowednolimitationsinactivitiesor participationrestrictionsatschoolage.
Purdy etal.37
1)Behavior 2)Motor 3)Language 4)Dailyandsocial life
5)Clinical life-threatening condition
1,2,3,and4)VABS 5)CRIB
Childrenwhoreceivedhigherdosesofperinatalsteroidsweremore likelytohavelowscoresofoveralldevelopment,especiallylower socialskills.Higherdosesofperinatalsteroidsresultedinamore severeconditionduringthefirstdayoflifebasedonCRIBanda smallerheadsizeatbirth,andthesewererelatedtoworse behavioraloutcomes.
Goyen etal.39
1)Motor 2)Sensory-motor skills
1)MABC-1
2)VMI,MVPT-R,KST, andSIPT
Significantlylowerscoreswerefoundforvisualprocessingandpraxis test,exceptforverbalcommand.Pretermchildrenwith
developmentalcoordinationdisorders(DCD)hadgreaterdifficulty withvisualprocessingtasks.Motorplanningrepresentedaspecial challengeforthesechildren.Motordysfunctioninextremely pretermchildrenwasrelatedtopoorervisualprocessingandmotor planning,whichmayberelatedtocognitiveprocessingproblems. Rademaker
etal.36
1)Intelligence 2)Motor 3)Memory
1)WISC
2)VMIandMABC-1 3)15-WordMemory Test
Childrentreatedwithhydrocortisonewereyounger,weighedless, andweresickerwhencomparedtothecontrolgroup.Therewereno differencesintheoccurrenceofbrainlesions.Neonataltreatment withhydrocortisoneforbronchopulmonarydysplasiashowedno long-termeffectsonneurodevelopmentandonthemotor performanceofpreterminfantsatschoolage.
Schneider etal.46
1)Visual-motor skills
(finemotorskill)
1)Visuo-manual pointing-taskand Reactiontimetest
Thereweresignificantdifferencesinfinemotorskillsbetweenthe groupsofpreterminfantsof26and31weeks.Therewereno significantdifferencesbetweenthecontrolgroupandthe31-week pretermchildrengroup.Thereactiontimesinthevisual-motortask weresignificantlyincreasedinpreterminfantswithGAof26weeks. PretermchildrenwithGAof26weeksshowedincreased
interhemispherictime,suggestingalterationsincallosalpathways. Programmingtimewassignificantlylongerforthedominanthand andunilateral.Theexistenceoffailedprogramminginvisual-manual tasksissuspectedinpreterminfantswithGA<26weeks.
Rademaker etal.2
1)Motor 2)Sizeofcorpus callosum
1)MABCandVMI 2)Magnetic resonance
Table2(Continued)
Article Outcomes Tools Results/Conclusions
Goyen&
Lui40
1)Motor 1)MABC;Peabody MotorScales,and Griffithscale (locomotor)
‘‘Apparentlynormal’’childrenathigh-riskinearlychildhoodare alsoatriskformotordysfunctionintheirschoolyears.Mostofthese childrenwithmotorproblemsatschoolagecouldbeidentifiedat theageof3years.Developmentalcoordinationdisorderwas independentlyassociatedwithprolongedruptureofmembranesand retinopathyofprematurity,butnotwithparentaleducationor occupation.
Karemaker etal.34
1)Motor 2)Behavior 3)School performance
1)MABC 2)CBCL 3)TRF
Childrentreatedwithdexamethasoneintheneonatalperiodhad lowerschoolperformanceandpresentedmorebehavioralproblems thanchildrentreatedwithhydrocortisone.Furthermore,themotor impairmentappearstobesignificantlyhigherinthegrouptreated withdexamethasonethaninthecontrolgroup.Childrenwhoused hydrocortisonedidnotdifferfromuntreatedchildren,exceptfor ballskills.Theresultssuggestthathydrocortisoneisasafe alternativefortreatment.
Sherlock etal.31
1)Motor 2)Cognitive 3)School performance
1)MABC-1
2)WISCIII,TOL,RCF 3)WRAT3
Neurodevelopmentaldysfunctioninschool-agechildrenwith extremelylowbirthweightand/orveryprematurevariedinrelation totheseverityofintraventricularhemorrhage,exceptforgrade4 intraventricularhemorrhage.Thehigherthedegreeofhemorrhage, thehigherthemotorandschoolimpairment.
Kanetal.30 1)Motor 2)School performance 3)Cognitive
1)MABC 2)WRAT3 3)WISCIII
Veryprematurechildrenhadlowerweightandheadcircumference atallagestested.Headcircumferenceatbirthwasnotrelatedto outcomesatschoolage,butchangesinheadcircumferenceatages2 and8yearswereassociatedwithworseperformanceonmost evaluatedmeasurements,includingmotorperformance.Intrauterine growthrestrictionwasnotrelatedtothechild’scognitiveskillsat age8years.Weightathospitaldischargehadlittleinfluenceon neurodevelopment,butheadcircumferencewasimportantinearly childhood.
BOTMP,Bruininks-OseretskyTestofMotorProficiency;BRIEF,Behavior RatingInventoryofExecutiveFunction;CBCL,ChildBehavior Checklist;CRIB,ClinicalRiskIndexforBabies;GMFCS,GrossMotorFunctionClassificationSystem;KST,KinaestheticSensitivityTest; MABC-1,MovementAssessmentBatteryforChildren;MACS,ManualAbilityClassificationSystem;MVPT-R,Motor-FreeVisualPerception Test;RCF,ReyComplexFigure;SIPT,SensoryIntegrationandPraxisTest;TOL,TowerofLondon;TRF,Teacher’sReportForm;VABS,Vineland AdaptiveBehavioralScales;VMI,TestofVisual-MotorIntegration;WISC,WechslerIntelligenceScale;WISCIII,WechslerIntelligenceScale III;WRAT-3,WideRangeAchievementTest.
studies (85%) included children aged 8 years, 13 (39%) includedchildrenaged9years,and15(45%)included chil-drenaged10years.Amongtheoutcomesofinterestforthis review,behaviorwasthemostoftenassessed(20articles, 61%),followedbyschoolperformance(16articles,48%)and motorimpairment(11articles,33%)(Tables2and3).
Behavior
In most studies, the outcome ‘‘behavior’’ was compre-hensivelyassessedusingtoolsthatidentifiedthepresence of components of internalization (depression, anxiety) and/or externalization (aggression, impulsiveness, delin-quent behaviors), mental health, temperament, social skills,and presence/absenceof psychiatricdisorders.The behaviorassessmentwasperformedbyninedifferenttools, inaddition togovernmentrecordswhen the studieswere population-based.TheChildBehaviorChecklist(CBCL)was themost widely used scale (9 articles,45%), followed by the Strength andDifficulties Questionnaire (SDQ)and the VinelandAdaptiveBehavioralScales(VABS)(3articleseach,
15%), and governmentrecords(2 articles, 10%). Allother toolswereusedonlyonce(Tables2and3).
Biologicalriskfactorsandtheireffectsonthe develop-ment of preterm infants has been the subject of studies that analyzed the outcome of behavior. The perinatal factorsmost often searchedfor thisoutcome were gesta-tionalage(5articles,25%),1,9,20---22 birthweight(5articles,
25%),20---25 and classification of birth weightin relation to
gestationalage (2 articles,10%).9,24 Inadditionto
biolog-ical factors, the evaluation of socioeconomic risk factors (socioeconomicstatus,maternal education,andethnicity) wassignificant,22,23,25aswellasenvironmentalfactors(noise
exposure,familyconflicts,andpsychologicaldistressofthe mother),21,25,26 and the analysis of the motor and
devel-opment componentin early childhoodas arisk factor for behavioralproblemsatschoolage.5
Someofthesestudiesconcludedthatthelowerthe gesta-tionalage(4articles,20%)1,20---22andbirthweight(4articles,
20%),20,21,23,25 thehighertheriskofbehavioralalterations.
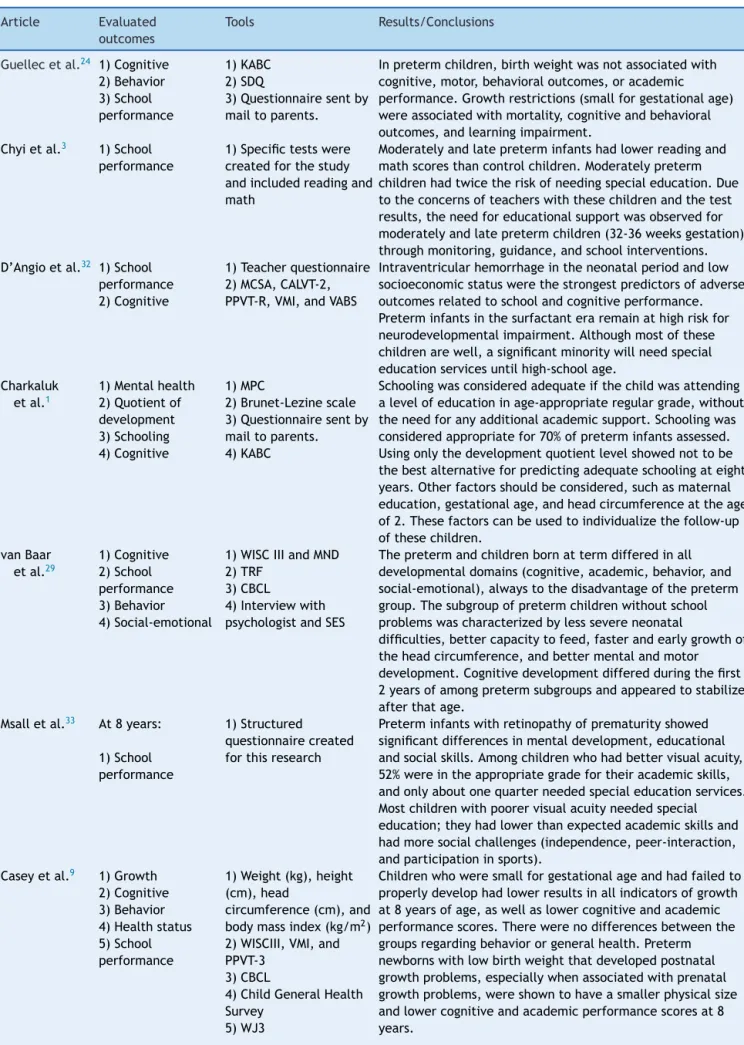
Table3 Studiesofschoolperformanceandbehaviorofpreterminfantsandtheirmainconclusions,BeloHorizonte,2012.
Article Evaluated
outcomes
Tools Results/Conclusions
Guellecetal.24 1)Cognitive
2)Behavior 3)School performance
1)KABC 2)SDQ
3)Questionnairesentby mailtoparents.
Inpretermchildren,birthweightwasnotassociatedwith cognitive,motor,behavioraloutcomes,oracademic performance.Growthrestrictions(smallforgestationalage) wereassociatedwithmortality,cognitiveandbehavioral outcomes,andlearningimpairment.
Chyietal.3 1)School performance
1)Specifictestswere createdforthestudy andincludedreadingand math
Moderatelyandlatepreterminfantshadlowerreadingand mathscoresthancontrolchildren.Moderatelypreterm childrenhadtwicetheriskofneedingspecialeducation.Due totheconcernsofteacherswiththesechildrenandthetest results,theneedforeducationalsupportwasobservedfor moderatelyandlatepretermchildren(32-36weeksgestation) throughmonitoring,guidance,andschoolinterventions. D’Angioetal.32 1)School
performance 2)Cognitive
1)Teacherquestionnaire 2)MCSA,CALVT-2, PPVT-R,VMI,andVABS
Intraventricularhemorrhageintheneonatalperiodandlow socioeconomicstatuswerethestrongestpredictorsofadverse outcomesrelatedtoschoolandcognitiveperformance. Preterminfantsinthesurfactanteraremainathighriskfor neurodevelopmentalimpairment.Althoughmostofthese childrenarewell,asignificantminoritywillneedspecial educationservicesuntilhigh-schoolage.
Charkaluk etal.1
1)Mentalhealth 2)Quotientof development 3)Schooling 4)Cognitive
1)MPC
2)Brunet-Lezinescale 3)Questionnairesentby mailtoparents. 4)KABC
Schoolingwasconsideredadequateifthechildwasattending alevelofeducationinage-appropriateregulargrade,without theneedforanyadditionalacademicsupport.Schoolingwas consideredappropriatefor70%ofpreterminfantsassessed. Usingonlythedevelopmentquotientlevelshowednottobe thebestalternativeforpredictingadequateschoolingateight years.Otherfactorsshouldbeconsidered,suchasmaternal education,gestationalage,andheadcircumferenceattheage of2.Thesefactorscanbeusedtoindividualizethefollow-up ofthesechildren.
vanBaar etal.29
1)Cognitive 2)School performance 3)Behavior 4)Social-emotional
1)WISCIIIandMND 2)TRF
3)CBCL
4)Interviewwith psychologistandSES
Thepretermandchildrenbornattermdifferedinall developmentaldomains(cognitive,academic,behavior,and social-emotional),alwaystothedisadvantageofthepreterm group.Thesubgroupofpretermchildrenwithoutschool problemswascharacterizedbylesssevereneonatal
difficulties,bettercapacitytofeed,fasterandearlygrowthof theheadcircumference,andbettermentalandmotor development.Cognitivedevelopmentdifferedduringthefirst 2yearsofamongpretermsubgroupsandappearedtostabilize afterthatage.
Msalletal.33 At8years:
1)School performance
1)Structured
questionnairecreated forthisresearch
Preterminfantswithretinopathyofprematurityshowed significantdifferencesinmentaldevelopment,educational andsocialskills.Amongchildrenwhohadbettervisualacuity, 52%wereintheappropriategradefortheiracademicskills, andonlyaboutonequarterneededspecialeducationservices. Mostchildrenwithpoorervisualacuityneededspecial education;theyhadlowerthanexpectedacademicskillsand hadmoresocialchallenges(independence,peer-interaction, andparticipationinsports).
Caseyetal.9 1)Growth 2)Cognitive 3)Behavior 4)Healthstatus 5)School performance
1)Weight(kg),height (cm),head
circumference(cm),and bodymassindex(kg/m2)
2)WISCIII,VMI,and PPVT-3
3)CBCL
4)ChildGeneralHealth Survey
5)WJ3
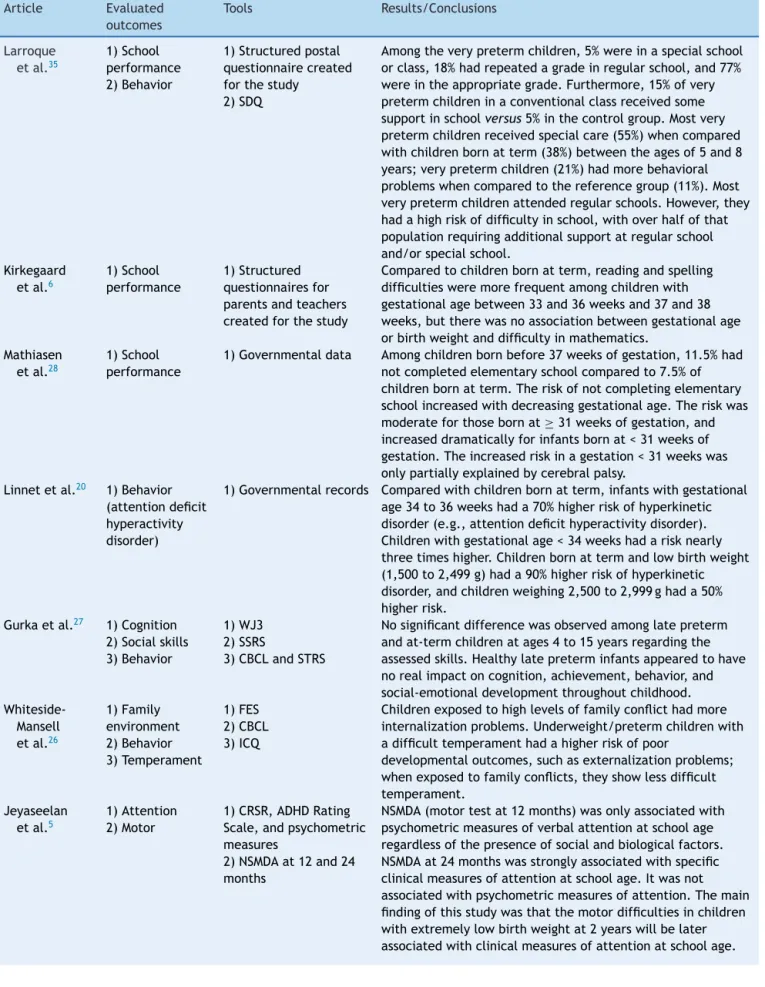
Table3(Continued)
Article Evaluated
outcomes
Tools Results/Conclusions
Larroque
etal.35
1)School performance 2)Behavior
1)Structuredpostal questionnairecreated forthestudy
2)SDQ
Amongtheverypretermchildren,5%wereinaspecialschool orclass,18%hadrepeatedagradeinregularschool,and77% wereintheappropriategrade.Furthermore,15%ofvery pretermchildreninaconventionalclassreceivedsome supportinschoolversus5%inthecontrolgroup.Mostvery pretermchildrenreceivedspecialcare(55%)whencompared withchildrenbornatterm(38%)betweentheagesof5and8 years;verypretermchildren(21%)hadmorebehavioral problemswhencomparedtothereferencegroup(11%).Most verypretermchildrenattendedregularschools.However,they hadahighriskofdifficultyinschool,withoverhalfofthat populationrequiringadditionalsupportatregularschool and/orspecialschool.
Kirkegaard etal.6
1)School performance
1)Structured questionnairesfor parentsandteachers createdforthestudy
Comparedtochildrenbornatterm,readingandspelling difficultiesweremorefrequentamongchildrenwith gestationalagebetween33and36weeksand37and38 weeks,buttherewasnoassociationbetweengestationalage orbirthweightanddifficultyinmathematics.
Mathiasen etal.28
1)School performance
1)Governmentaldata Amongchildrenbornbefore37weeksofgestation,11.5%had notcompletedelementaryschoolcomparedto7.5%of childrenbornatterm.Theriskofnotcompletingelementary schoolincreasedwithdecreasinggestationalage.Theriskwas moderateforthosebornat≥31weeksofgestation,and
increaseddramaticallyforinfantsbornat<31weeksof gestation.Theincreasedriskinagestation<31weekswas onlypartiallyexplainedbycerebralpalsy.
Linnetetal.20 1)Behavior (attentiondeficit hyperactivity disorder)
1)Governmentalrecords Comparedwithchildrenbornatterm,infantswithgestational age34to36weekshada70%higherriskofhyperkinetic disorder(e.g.,attentiondeficithyperactivitydisorder). Childrenwithgestationalage<34weekshadarisknearly threetimeshigher.Childrenbornattermandlowbirthweight (1,500to2,499g)hada90%higherriskofhyperkinetic disorder,andchildrenweighing2,500to2,999ghada50% higherrisk.
Gurkaetal.27 1)Cognition 2)Socialskills 3)Behavior
1)WJ3 2)SSRS
3)CBCLandSTRS
Nosignificantdifferencewasobservedamonglatepreterm andat-termchildrenatages4to15yearsregardingthe assessedskills.Healthylatepreterminfantsappearedtohave norealimpactoncognition,achievement,behavior,and social-emotionaldevelopmentthroughoutchildhood.
Whiteside-Mansell etal.26
1)Family environment 2)Behavior 3)Temperament
1)FES 2)CBCL 3)ICQ
Childrenexposedtohighlevelsoffamilyconflicthadmore internalizationproblems.Underweight/pretermchildrenwith adifficulttemperamenthadahigherriskofpoor
developmentaloutcomes,suchasexternalizationproblems; whenexposedtofamilyconflicts,theyshowlessdifficult temperament.
Jeyaseelan etal.5
1)Attention 2)Motor
1)CRSR,ADHDRating Scale,andpsychometric measures
2)NSMDAat12and24 months
Table3(Continued)
Article Evaluated
outcomes
Tools Results/Conclusions
Conradetal.23 1)Cognitive
2)Behavior evaluatedby parentsand teachers
1)WISC
2)PediatricBehavior Scale---30
Childrenbornattermhadfewerparentalreportsof hyperactivity/inattentionanddepression/anxietywhen comparedtochildrenofextremelylowbirthweightandvery lowbirthweight.Therewerenosignificantdifferences betweenthegroupsinteachers’evaluations.Birthweightwas thestrongestpredictorofbehavioraloutcomesthatappears nottobeinfluencedbythechild’sintelligence.Itwas observedthatnegativebehavioralsequelaeofpretermbirth remainsignificantinchildhoodandadolescence.
Purdyetal.44 1)Behavior 2)Stressatbirth 3)Perinatal factors
1)CBCL
2)CRIB,SNAPPE-II,and NBRS
3)Reviewof
retrospectiverecords (sepsis,retinopathy,and otherneonatalvariables)
ThereweresignificantassociationsbetweenCBCLandsepsis, cumulativeexposuretosteroidsintheperinatalperiod,time frominitialexposuretosteroids,andheightpercentileat discharge.Therewasalsoastrongassociationbetween problemsofsocialandschoolcompetenceandactivities assessedbytheCBCLandthevariablecumulativeexposureto steroids,heightpercentileofchildrenintheintensivecare unit,sepsis,retinopathy,CRIBscore,hearingloss,and biologicalmarkers.Childreninthegroupwithhigherexposure tosteroidspresentedmorebehavioralproblems,butitwas notpossibletodetectsignificantdifferences.Theresultsare reassuringregardingthelong-termeffectsofcumulative exposuretosteroidsonthebehavioraloutcomesofpreterm infants.
Farooqietal.43 1)Behavioral problems 2)Adaptive behavioratschool 3)Familyfunction (environment) 4)Depression
1)CBCLforparentsand teachers
2)Structured
questionnaireandTRF 3)NordicHealthand FamilyQuestionnaire 4)DSRS
Comparedwithcontrolchildren,parentsofprematureinfants reportedmoreinternalizationbehavior,attention,andsocial problems.Teachershadasimilaropinion.Reportsfromthe childrenshowedatrendofincreasedsymptomsofdepression comparedtothecontrolgroup.However,themajorityof extremelypretermchildren(85%)werestudyinginregular schoolswithoutmajoradjustmentproblems.Althoughthese resultsappearfavorable,teachersreportthatthesechildren havepooreradjustmenttotheschoolenvironmentandareat riskofmentalhealthproblems.
Grayetal.25 1)Maternal psychological problems 2)Behavior
1)GHQ 2)CBCL
Theprevalenceofbehavioralproblemswasapproximately20% atallagestested(3,5,and8years).Thissamplehadtwice theprevalenceofbehavioralproblemsexpectedinchildren. Thesignificantpredictorsoftheseproblemsweresmoking duringpregnancy,maternalpsychologicaldistress,maternal age,andHispanicethnicity.
Yuetal.45 1)Behavior 2)Learning failure
1)CBCL
2)WISCIIIandWJ3
Comparedwithchildrenwithverbalandnonverballearning disability,childrenwithverbaldisabilityweretwiceaslikely tohavebehavioralproblems,andwere89%morelikelyto haveexternalizationbehaviorproblems.Noassociationwas foundbetweenlearningdifficultiesinnonverbaldisabilityand behavioralproblems.Analysisofspecificbehavioralsubscales showedsignificantassociationwithbehaviorsof
Table3(Continued)
Article Evaluated
outcomes
Tools Results/Conclusions
Anderson
etal.42
1)Cognitive 2)School performance 3)Behavior
1)WISCIII
2)WRAT-3andCSSA 3)BASC
Extremelypretermorunderweightchildrenhadlowerscores thanthecontrolgroupinIQ,verbalcomprehension,
perceptualorganization,distractibility,andprocessingspeed. Attentiondifficulties,internalizationproblems,andadaptive skillswerehigherinthegroupofpreterm/lowbirthweight children.Inaddition,thisgroupshowedworseperformanceon testsofreading,spelling,andarithmeticcomparedtothe controlgroup.School-agechildrenwithextremelylowbirth weightorverypreterminfantsborninthe1990scontinueto havecognitive,educational,andbehavioraldisabilities. Crombieetal.
21
1)Mentalhealth 2)Earlyrisk assessment
1)SDQ 2)Structured
questionnairecompleted byparents
Childrenwithearlybiologicalrisk(pretermorlowbirth weight)wereshowntobemorevulnerabletomentalhealth problemswhenexposedtotheeffectsofnoisefromaircraftor roadtrafficnoiseintheschoolarea.However,thesechildren weremorelikelytohavementalhealthproblems.Children whowere‘‘atrisk’’(i.e.,lowbirthweightorpretermbirth) wereclassifiedashavingmorebehavioralproblemsand emotionalsymptomsandpooreroverallmentalhealththan childrenwithouttheserisks.
Lindström etal.22
1)Psychiatric disorders 2)Perinataland socialfactors
1and2)Governmental records
Pretermandearly-termbirthincreasestheriskofattention deficithyperactivitydisorder(ADHD).Thesocioeconomic contextmodifiestheriskofADHDinmoderatelypreterm births.
BASC,BehaviorAssessmentSystemforChildren;CALVT-2,Children’sAuditoryVerbalLearning;CBCL,ChildBehaviorChecklist;CRIB, ClinicalRiskIndexforBabies;CRSR,Conners’RatingScaleRevised-LongForm;CSSA,ComprehensiveScalesofStudentAbilities;DSRS, DepressionSelf-RatingScale;FES,FamilyEnvironmentScale;GHQ,MaternalGeneralHealthQuestionnaire;ICQ,InfantCharacteristics Questionnaire;KABC,KaufmanAssessmentBatteryforChildren;MCSA,McCarthyScalesofChildren’sAbilities;MND,minor neurolog-icaldysfunctions;MPC,MentalProcessing Composite;NBRS: NeurobiologicalRiskScore;NSMDA,Neurosensory MotorDevelopmental Assessment;PPVT-3,PeabodyPictureVocabularyTest-3;PPVT-R,PeabodyPictureVocabularyTest-Revised;SDQ,StrengthandDifficulties Questionnaire;SES,socio-economicstatusscore;SNAPPE-II,ScoreforNeonatalAcutePhysiologyPerinatal.ExtensionII;SSRS,SocialSkills RatingSystem---TeacherForm;STRS,Student-TeacherRelationshipScale;TRF,Teacherreportform;VABS,VinelandAdaptiveBehavior Scale;VMI,TestofVisual-MotorIntegration;WISCIII,WechslerIntelligenceScaleforChildren;WJ3,WoodcockJohnsonTestofAcademic Achievement;WRAT-3,WideRangeAchievementtest.
The general concept of behavior was the most often assessed outcome (11 articles, 55%), followed by more specific components, such as mental health (4 articles, 20%)andattentiondeficithyperactivitydisorder(3articles, 15%).Moreover,temperament,familyconflicts,depression, anxiety, and emotional development were also assessed (one article each, 5%). Only two of these studies found no effect of preterm birth on the school-age child’s behavior.9,27
School
performance
Schoolperformancewasalsoarecurringtheme,withmostof thestudies comparingtheperformanceofpreterminfants andthose born at termusing sixdifferent scales. Halfof thearticles(50%)investigatedschoolingthroughstructured questionnairesor tests created by the researchers them-selves,whichwereappliedtothechildrenortheirparents andteachers.TheWideRange AchievementTest(WRAT-3) wasthemostcommonlyusedstandardizedtool(3articles, 19%),followedbytheWoodcockJohnsonTestofAcademic Achievement(WJIII)(2articles,12%)(Table3).
Consideringschoolperformance,themostoftenassessed birth conditions were gestational age at birth (4 arti-cles, 25%),1,6,9,28 followed by birth weight6,24,29 and head
circumference (3articles,19%),1,29,30 periventricular
hem-orrhage (2articles,12%)andclassificationof birthweight in relation to gestationalage (2 articles, 12%).31,32 Other
variablesinvestigatedwereperinatalretinopathy,33 use of
corticosteroids,34anduseofsurfactants35(onearticleeach,
6%).
Allarticlesthat investigatedgestationalage,head cir-cumference, intraventricularhemorrhage,classificationof birth weight in relation to gestational age, retinopathy, use of surfactants and corticosteroids demonstrated an association with school performance. Most studies that investigated birth weight also found an association with schoolperformance(2articles,12%).6,29Fourarticles(25%)
assessed socioeconomic risk factors;29,32,33,35 the majority
(threearticles,19%)observedanassociationbetweenschool performanceandsocioeconomicmarkers.32,33,35
3,153 articles identified in databases
139 articles repeated and excluded
19 articles not available and excluded for not meeting
eligibility criteria
2,991 articles with title and summary analyzed
2,900 excluded for not meeting the eligibility criteria
91 articles read in full 14 excluded for not meeting the eligibility
77 articles met the eligibility criteria
44 excluded after methodological quality
assessment
33 included in the systematic review
Figure1 Flowchartforselectionofarticlesatthedifferentphasesofthesystematicreview,BeloHorizonte,Brazil,2012.
considered the viewpoints of parents and/or teachers regardingthechildren’sacademicskills,andonlyone arti-clewasbasedongovernmentdatatoevaluatetheacademic success of preterm children. It was also observed that moststudiesaimedtoassesswhetherthepretermchildren attended a grade appropriate for their age and whether theystudiedinspecialschoolsorneededanyschoolaid(6 articles, 37%). Only onestudy didnot find an association betweenpretermbirthandschoolperformance.32
Motor
performance
Articles that investigated the motor component focused onthe drugs usedin the neonatal periodand their influ-enceonthedevelopment,identificationofriskfactorsfor motor impairment, and concerns about social limitations andrestrictions ofpretermchildren comparedtochildren born at term. To assess the motor skills of preterm chil-dren,fivedifferenttoolswereused(MovementAssessment BatteryforChildren[MABC-1],DevelopmentalTestofVisual MotorIntegration[VMI],Bruininks-Oseretsky Testof Motor Proficiency [BOTMP], Vineland Adaptive Behavioral Scales [VABS],andGriffithsscale),aswellastwoclassification sys-tems(onetoassessgrossmotorfunction, theGrossMotor Function Classification System [GMFCS], and the other to
assessfinemotorskills,themanualAbilityClassification Sys-tem[MACS]).TheMABC-1wasthemostcommonlyusedtool todetectmotorabnormalities(7articles,64%),followedby VMI(4articles,36%). Theremainder toolswereusedonly once(Table2).
Mostarticlesthatinvestigatedmotorperformancesought toexamineperinatalriskfactorsandtheirimpactonschool age(7articles,64%),while otherarticlesfocused on ana-lyzingonlythe consequencesof pretermbirth (4articles, 36%).
The risk factors most often studied were the use of corticosteroids in the neonatal period (3 articles, 27%),34,36,37followedbyperiventricularhemorrhage(2
arti-cles,18%),31,38 headcircumference(onearticle, 9%),30 and
sizeofthecorpuscallosum(onearticle,9%).2Ofthethree
articlesthatanalyzedtheeffectsofdifferentdrugsonthe developmentofpretermchildren,twofoundanassociation betweentheuseofdexamethasoneandmotordisorders.34,37
Twoarticlesfoundnoeffectsofhydrocortisoneuseonmotor development,suggestingthatthisisasaferalternativefor useincasesoflungproblems.34,36
Of the two articles that investigated intraventricular hemorrhage,onlyoneobservedanassociationwithpoorer motorperformance.31Allarticlesthatinvestigatedthesize
associationwithmotordisorders.Theauthorsofthese stud-iesevaluateddifferentaspectsofmotorperformance,and themost oftenassessedareasweregross/finemotorskills and visual-motor integration. Only one study, among the seventhatanalyzedriskfactors,didnotobservelong-term effectsofpretermbirthonmotorperformance.36
Thefourremainingarticlesthatassessedmotor perfor-manceanalyzed, fromdifferent perspectives, the impact of preterm birth on school age. Two articles assessed sensorimotor skills,36,39 such as visual-motor integration;
one article assessed the fine/gross motor development;40
and the last article measured physical activity and car-diorespiratoryperformance.10 Allfourarticlesfoundmotor
impairmentsrelated topreterm birth.Considering allthe articlesthatassessedmotorbehavior,itwasobservedthat most researcherswere concerned with assessing fine and gross motor developmentof preterm children (7articles, 64%). Some articles also assessed aspects related to the visual-motorintegration(5articles,45%)andthe function-alityofpretermchildren(3articles,27%).
Theassessmentofmethodologicalqualityoftheselected studiesdemonstratedthat24articles(73%)met80%to90% oftheSTROBEscalecriteria,and9articles(27%)metover 90%oftheitemsofthisscale.Allarticlesmetalltheitems ofthefollowingcategories:‘‘datasources/measurements’’ (toprovidethesourceofdataanddetailsusedforthe mea-surement),‘‘outcome’’(topresenttheoutcomesandtheir summarymeasures),and‘‘mainfindings’’inthediscussion (to summarize themain findings,correlating them tothe studyobjectives).Thelowest-scoringitemwas‘‘studysize’’ (toexplainhowsamplesize wasdetermined)(23articles, 70%).
Thefindings/conclusionsoftheselectedstudiesshowed thattheassociationbetweenpretermbirthandpoormotor development,behavior,andschoolperformance abnormal-itieswasdemonstratedby most of thestudies. Of the47 differentdevelopmentoutcomesevaluated,32(68%)found anassociationofpretermbirthwiththestudied outcomes (7articlesonmotordevelopment,13onbehavior,and12on schoolperformance).Twelvestudiesfailedtoachieveallthe desiredgoals(3articlesonmotordevelopment,5on behav-ior,and3onschoolperformance),andonly4studiesfailed toshowanassociationbetweenpretermbirthandlong-term outcomes(onearticleonmotordevelopment,2onbehavior, andoneonschoolperformance)(Tables2and3).
Discussion/Conclusion
The main finding of this review was the confirmation of the long-term vulnerability of preterm infants regarding alldevelopmentalindicatorsassessed(motor,behavior,and schoolperformance). Thus,expansion of thefollow-up of preterm children is needed, as the school stage is a key momentfor the child’s development,because it requires skillsthathavenotbeenpreviouslydemanded,whichmight beimpaired.1Itisimportanttoconsiderthatfollow-uponly
untilto2 yearsof age is insufficient for the detectionof developmentproblemssuchasbimanualskills,behavior,and visual-motorintegrationabnormalities.
Anotherextremely importantfindingconcerns the ges-tational age studied. Most articles focused on studying
extreme prematurity, and only a small part investigated the development of moderate to late preterm infants.41
It is necessary toexpand the studies in ordertoproperly assessthedevelopmentofallpreterminfants bornat dif-ferentgestational ages.Moderatetolate preterminfants arealsosusceptibletodevelopmentalimpairment,andare moreprevalentthanextremelypreterminfants.41
Regarding the methodological design of the evaluated studies, it wasexpected that cohorts would be the most frequentmodel,astheyallowforthefollow-upofpreterm infants.Itwasalsotobeexpectedthatthesestudieswould be conducted in developed countries, as they have the financialresourcesrequiredforstudieswithlongfollow-up periods. However, these are troubling data, as they sug-gestthat,inthelasttenyears,nostudieswereconducted in developing countries such as Brazil using the quality parameters usedin thisstudy. To illustrate the situation, isnoteworthytoobservethatamongthe77studiesinitially selectedforthissystematicreview,onlytwohadbeen per-formedinBrazil;however,theypresentedaBscoreinthe STROBEscale,andwerethusremovedfromthisreview.
Thebehaviorofpreterminfantsisoneoftheoutcomes ofgreatestinterest amongresearches inthedevelopment area.Thereisagrowingeffortbyresearchersinanattempt toassesstheconsequencesofpretermbirthonthechildren’s mentalhealth.25Thisisanotherimportantresult,sincemost
ofthestudiesdemonstratedanassociationbetweenpreterm birth and behavioral problems.42---45 However, it is worth
mentioning that the greatnumber oftools usedto assess thisareamakesresultcomparisondifficult.
Another outcome that deserved the attention of researchers was school performance; most articles that assessedthissubjectconfirmedthattherearesome school-relatedproblems among pretermchildren.6,28 This finding
isofgreatrelevancetogovernmentagencies,asitsupports thecreationofpublicpoliciesaimedatthispopulation,such asearlydiagnosisandinterventionprograms.However,itis noteworthythathalfof thestudiesusednon-standardized tools (questionnaires created by the researchers them-selves),andthat,inmanycases,theviewpointsofparents about the children’s educational process were assessed ratherthanthechildren’sperformance.Thisfactbrings sub-jectivitytotheresearch,andshouldbefurtherexploredin futurestudies.
Mildmotorimpairments, oftenimperceptible tofamily and friends, were also targeted by the analyzed stud-ies.There is an agreement between the analyzed studies thatpreterm birthhasan effectonmotor performance.46
Although there is alsoa reasonable variabilityamong the toolsusedfordetecting motorimpairment,allscalesused were standardized; most studies used the MABC-1 in the evaluationofthesechildren.MABC-1isoneofthemostoften usedtoolstodetect disordersofmotor coordination,asit hasadequatepsychometricpropertiesanditsuseissimple andenjoyableforchildren.47,48
oftheresearchcontextandcharacteristicsofthestudy pop-ulation.Althoughtheyefficientlydescribedthelocationand thetimeofrecruitmentofthechildren,moststudiesfailed toreport itemssuch asthe periodof data collectionand follow-up.
Eventhoughtheydiscloseddescriptivedataofthe clini-calvariables,mostoftheselectedstudiesfailedtoprovide the description of sociodemographic variables, which can directlyinterferewiththedevelopmentofthesechildren. Theresultssectionlackedamoredetaileddescriptionofthe findings(confidenceintervals,forexample).
The main limitation of this study was that only one reviewerselectedandanalyzedthemethodologicalquality ofthestudies.Nevertheless,thisstudyattemptedtoprovide well-established,high-qualityevidence.Theimportanceof themethodologicalanalysisofobservationalstudiesandnot onlyofexperimentalonesisnoteworthy,anunusualfactin theBrazilianliterature.
It can be concluded, considering the evidence of the last ten years that preterm infants are more susceptible tomotor development,behavior, and school performance abnormalities when compared to children born at term. Theseabnormalitiesaremodulatedbybiologicaland envi-ronmentalfactorsthatdeterminetheirintensity.Therefore, a greater investment by managers of long-term monitor-ing programsand early intervention is necessary in order to minimize future sequelae. With these results, health-careprofessionalsandfamilymembersshouldremainalert toanychanges inthe developmentofpreterm infants,in additiontodemandingfromthegovernmentthe establish-ment of public policies aimed to promote positive early experiences for this population, such as the creation of higher-qualitypublicdaycarecenters.Furtherstudiesthat meettheinternationalqualitystandardsinthisarea, includ-ing randomizedcontrolledtrials, arerequired in orderto comparetheeffectsofdifferentearlyinterventionsonthe developmentofchildrenbornprematurely.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.CharkalukML,TruffertP,Marchand-MartinL,MurS,KaminskiM, AncelPY,etal.Verypretermchildrenfreeofdisabilityordelay atage2:predictorsofschoolingatage8:apopulation-based longitudinalstudy.EarlyHumDev.2011;87:297---302.
2.RademakerKJ,LamJN,VanHaastertIC,UiterwaalCS,Lieftink AF,GroenendaalF,etal.Largercorpuscallosumsizewith bet-termotor performance in prematurely born children.Semin Perinatol.2004;28:279---87.
3.Chyi LJ, Lee HC, Hintz SR, Gould JB, Sutcliffe TL. School outcomes of late preterm infants: special needs and chal-lengesforinfantsbornat32to36weeksgestation.JPediatr. 2008;153:25---31.
4.NationalScientific Councilon theDeveloping,Child.In: tim-ingand qualityofearlyexperiences combineto shapebrain architecture:WorkingPaper5.Cambridge,MA:Centeronthe DevelopingChild,HarvardUniversity;2007.p.1-9.
5.JeyaseelanD,O’CallaghanM,NeulingerK,ShumD,BurnsY.The associationbetweenearlyminormotordifficultiesinextreme
lowbirthweightinfantsandschoolageattentionaldifficulties. EarlyHumDev.2006;82:249---55.
6.KirkegaardI,ObelC,HedegaardM,HenriksenTB.Gestational ageandbirthweightinrelationtoschoolperformanceof 10-year-oldchildren:afollow-upstudyofchildrenbornafter32 completedweeks.Pediatrics.2006;118:1600---6.
7.VieiraME,LinharesMB.Developmental outcomesandquality oflifeinchildrenbornpretermatpreschool-andschool-age.J Pediatr(RioJ).2011;87:281---91.
8.Linhares MB,Chimello JT,Bordin MB,CarvalhoAE, Martinez FE. Psychological development of school-aged children born preterm in comparison with children born full-term. Psicol ReflexCrit.2005;18:109---17.
9.CaseyPH,Whiteside-MansellL,BarrettK,BradleyRH,Gargus R.Impactofprenataland/orpostnatalgrowthproblemsinlow birthweightpreterminfantsonschool-ageoutcomes:an8-year longitudinalevaluation.Pediatrics.2006;118:1078---86.
10.Svien LR. Health-related fitness of seven- to 10-year-old children with histories of preterm birth. Pediatr Phys Ther. 2003;15:74---83.
11.TheCochraneLibrary.JohnWiley&Sons,Inc.[cited2012Aug 5].Availablefrom:www.thecochranelibrary.com
12.Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting sys-tematic reviewsand meta-analysesof studies that evaluate healthcare interventions:explanationand elaboration.PLoS Med.2009;6:e1000100.
13.MaltaM,CardosoLO,BastosFI,MagnaniniMM,SilvaCM.STROBE initiative: guidelineson reporting observational studies.Rev SaudePublica.2010;44:559---65.
14.PhysiotherapyEvidenceDatabase.Sydney:TheGeorgeInstitute for Global Health;2013 [cited2012 May4]. Available from: http://www.pedro.org.au/portuguese/
15.DoddKJ, TaylorNF,Damiano DL.Asystematicreviewofthe effectiveness of strength-training programs for people with cerebralpalsy.ArchPhysMedRehabil.2002;83:1157---64.
16.SampaioRF,ManciniMC.Systematicreviewstudies:aguidefor carefulsynthesisofthescientificevidence.RevBrasFisioter. 2007;11:77---82.
17.von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP, et al. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) state-ment: guidelines for reporting observational studies. BMJ. 2007;335:806---8.
18.MataratzisPS,AcciolyE,PadilhaPC.Micronutrientdeficiencyin childrenandadolescentswithsicklecellanemia:asystematic review.RevBrasHematolHemoter.2010;32:247---56.
19.StoccoJG,CrozetaK,TaminatoM,DanskiMT,MeierMJ. Evalu-ationofthemortalityofneonatesandchildrenrelatedtothe useofcentralvenouscatheters:asystematicreview.ActaPaul Enferm.2012;25:90---5.
20.Linnet KM, Wisborg K, Agerbo E, Secher NJ, Thomsen PH, HenriksenTB. Gestationalage, birthweight, and theriskof hyperkineticdisorder.ArchDisChild.2006;91:655---60.
21.CrombieR,ClarkC,StansfeldSA.Environmentalnoise expo-sure, early biologicalrisk and mentalhealth in nine to ten yearoldchildren:across-sectionalfieldstudy.EnvironHealth. 2011;10:39.
22.LindströmK,LindbladF,HjernA.Pretermbirthand attention-deficit/hyperactivity disorder in schoolchildren. Pediatrics. 2011;127:858---65.
23.ConradAL,RichmanL, LindgrenS,NopoulosP.Biologicaland environmental predictors of behavioral sequelae in children bornpreterm.Pediatrics.2010;125:e83---9.
25.GrayRF,IndurkhyaA,McCormickMC.Prevalence,stability,and predictors of clinically significant behavior problems in low birthweightchildrenat3,5,and8yearsofage.Pediatrics. 2004;114:736---43.
26.Whiteside-MansellL,BradleyRH,CaseyPH,FussellJJ, Conners-Burrow NA.Triple risk:do difficult temperament and family conflictincreasethelikelihoodofbehavioralmaladjustmentin childrenbornlowbirthweightandpreterm?JPediatrPsychol. 2009;34:396---405.
27.Gurka MJ, LoCasale-Crouch J, Blackman JA. Long-term cognition,achievement,socioemotional,andbehavioral devel-opmentofhealthylate-preterminfants.ArchPediatrAdolesc Med.2010;164:525---32.
28.Mathiasen R, Hansen BM,Andersen AM,Forman JL, Greisen G. Gestational age and basic school achievements: a national follow-up study in Denmark. Pediatrics. 2010;126: 1553---61.
29.vanBaarAL,UlteeK,GunningWB,SoepatmiS,LeeuwR. Devel-opmentalcourseofverypretermchildreninrelationtoschool outcome.JDevPhysDisabil.2006;18:273---93.
30.KanE,RobertsG,AndersonPJ,DoyleLW,VictorianInfant Col-laborativeStudyGroup.Theassociationofgrowthimpairment withneurodevelopmentaloutcomeateightyearsofageinvery pretermchildren.EarlyHumDev.2008;84:409---16.
31.Sherlock RL, Anderson PJ, Doyle LW, Victorian Infant Col-laborative Study Group. Neurodevelopmental sequelae of intraventricular haemorrhageat 8years ofageina regional cohort of ELBW/very preterm infants. Early Hum Dev. 2005;81:909---16.
32.D’AngioCT,SinkinRA,StevensTP,LandfishNK,MerzbachJL, RyanRM,etal.Longitudinal,15-yearfollow-upofchildrenborn atlessthan29weeks’gestationafterintroductionofsurfactant therapyintoa region:neurologic,cognitive,andeducational outcomes.Pediatrics.2002;110:1094---102.
33.MsallME,PhelpsDL,HardyRJ,DobsonV,QuinnGE,Summers CG,etal.Educationalandsocial competenciesat8yearsin childrenwiththresholdretinopathyofprematurityinthe CRYO-ROPmulticenterstudy.Pediatrics.2004;113:790---9.
34.KaremakerR,HeijnenCJ,VeenS,BaertsW,SamsomJ,Visser GH,etal.Differencesinbehavioraloutcomeandmotor devel-opment at school age after neonatal treatment for chronic lungdiseasewithdexamethasoneversushydrocortisone. Pedi-atrRes.2006;60:745---50.
35.LarroqueB,AncelPY,Marchand-MartinL,CambonieG,Fresson J,PierratV,etal.Specialcareandschooldifficultiesin 8-year-oldverypretermchildren:theEpipagecohortstudy.PLoSOne. 2011;6:e21361.
36.RademakerKJ,UiterwaalCS,GroenendaalF,VenemaMM,van Bel F, Beek FJ, et al. Neonatal hydrocortisone treatment: neurodevelopmentaloutcomeandMRIatschoolagein preterm-bornchildren.JPediatr.2007;150:351---7.
37.PurdyIB,WileyDJ,SmithLM,HowesC,GawlinskiA,Robbins W,etal.Cumulativeperinatalsteroids:childdevelopmentof preterminfants.JPediatrNurs.2008;23:201---14.
38.RozeE,VanBraeckelKN,vanderVeereCN,MaathuisCG, Mar-tijnA, BosAF.Functionaloutcome atschoolageofpreterm infantswithperiventricularhemorrhagicinfarction.Pediatrics. 2009;123:1493---500.
39.GoyenTA,LuiK,HummellJ.Sensorimotorskillsassociatedwith motordysfunctioninchildrenbornextremely preterm.Early HumDev.2011;87:489---93.
40.Goyen TA, Lui K. Developmental coordination disorder in ‘‘apparentlynormal’’schoolchildrenbornextremelypreterm. ArchDisChild.2009;94:298---302.
41.vanBaarAL,VermaasJ,KnotsE,deKleineMJ,SoonsP. Func-tioningatschoolageofmoderatelypretermchildrenbornat32 to36weeks’gestationalage.Pediatrics.2009;124:251---7.
42.Anderson P, Doyle LW, Victorian Infant Collaborative Study Group.Neurobehavioraloutcomesofschool-agechildrenborn extremelylowbirthweightorverypreterminthe1990s.JAMA. 2003;289:3264---72.
43.FarooqiA,HägglöfB,SedinG,GotheforsL,SereniusF.Mental health and social competencies of 10- to 12-year-old chil-dren born at 23 to 25 weeks of gestation in the 1990s: a Swedish national prospective follow-up study. Pediatrics. 2007;120:118---33.
44.Purdy IB, Smith L, Wiley D, Badr L. A psychoneuroimmuno-logic examination of cumulative perinatalsteroid exposures and preterm infant behavioral follow-up. Biol Res Nurs. 2013;15:86---95.
45.YuJW,BukaSL,McCormickMC,FitzmauriceGM,IndurkhyaA. Behavioralproblemsand theeffectsofearlyinterventionon eight-year-oldchildrenwithlearningdisabilities.MaternChild HealthJ.2006;10:329---38.
46.SchneiderC,NadeauL,BardC,LambertJ,MajnemerA, Mal-ouinF,etal.Visuo-motorcoordinationin8-year-oldchildren born pre-term before and after28 weeksof gestation. Dev Neurorehabil.2008;11:215---24.
47.SchulzJ,HendersonSE,SugdenDA,BarnettAL.Structural valid-ityoftheMovementABC-2test:factorstructurecomparisons acrossthreeagegroups.ResDevDisabil.2011;32:1361---9.