w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Original
article
Physical
activity
level
and
performance
in
the
six-minute
walk
test
of
children
and
adolescents
with
sickle
cell
anemia
Hugo
Nivaldo
Melo
a,∗,
Simone
Joanna-Maria
Stoots
b,
Marijn
Aimee
Pool
b,
Vitor
Oliveira
Carvalho
a,
Lucas
Oliveira
Carvalho
Almeida
a,
Max
Luan
De
Carvalho
Aragão
a,
Charles
Agyemang
b,
Rosana
Cipolotti
a aUniversidadeFederaldeSergipe(UFS),Aracaju,SE,BrazilbUniversityofAmsterdam(UvA),Amsterdam,Netherlands
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received14December2016
Accepted13February2017
Availableonline31March2017
Keywords:
Exercise
Motoractivity
Sicklecellanemia
Physicalexertion
a
b
s
t
r
a
c
t
Background:Toestablishdeterminantsofmaximumwalkingdistanceinthe6-minutewalk
testofchildrenandadolescentswithsicklecellanemia,andtocomparetheperformance
inthistestwithphysicalactivitylevelbetweenpatientsandhealthycontrols.
Methods:Across-sectionalstudywasperformedinwhichtheparticipantsansweredthe
PhysicalActivityQuestionnaireforOlderChildrenandAdolescents,andcompletedthe
6-minutewalktest.
Mainresults:Fifty-sevenpatientsand58controlswerestudied.Byunivariateanalysisofthe
patients,age(p<0.0001)andindirectbilirubin(p=0.008)wereassociatedwithmaximum
walking distanceinthe6-minutewalktest.Inmultivariateanalysis,agewaspositively
associated(p<0.0001;beta:0.75),whilebodymassindexwasinverselyassociatedwith
dis-tancewalked(p=0.047;beta:−0.32).Thisyieldsthefollowingequation:maximumdistance
walked=487.7(age×18.3)−(12×bodymassindex)meters.Patientsreportedalower
phys-icalactivitylevelhowevertherewasnosignificantdifferenceinthedistancewalkedinsix
minutesbetweenpatients(500.6±88.7m)andcontrols(536.3±94m).
Conclusion: Thedeterminantsforthe6-minutewalktestinchildrenandadolescentswith
sicklecellanemiawereageandbodymassindex.Therewasnosignificantdifferenceinthe
6-minutewalktestbutpatientswithsicklecellanemiahadalowerphysicalactivitylevel
comparedtohealthycontrols.
©2017Associac¸ ˜aoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.Published
byElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense
(http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗ Correspondingauthorat:CampusdaSaúde,HospitalUniversitário,Av.CláudioBatista,s/n.49.000-000Aracaju,SE,Brazil.
Tel.:+5579999599391.
E-mailaddress:[email protected](H.N.Melo).
http://dx.doi.org/10.1016/j.bjhh.2017.02.009
1516-8484/©2017Associac¸ ˜aoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.PublishedbyElsevierEditoraLtda.Thisisan
Introduction
Sickle cell anemia (SCA) is the most common monogenic
hereditarydisease inBrazil. Themaincharacteristicisthe
inheritance of the beta-globin gene S (gene s), which is
responsibleforamutanthemoglobin(Hb),HbS.Itisestimated
that2–8%oftheBrazilianpopulationisheterozygousforHb
S.1
Several clinical manifestations are commonly observed
inpatients with SCA, such asocclusive crisis, acute chest
syndrome, stroke, chronic hemolysis and chronic organ
dysfunction.2Theseclinicalmanifestationsalsoappeartobe
associatedwith changes in physical capacity, higher basal
metabolicrate,3 lowerlevelsofHb,pulmonaryandvascular
diseases,andmyopathy.4
Differentmethodsareavailableintheclinicalpracticeto
assess physical capacity, suchas the six-minute walk test
(6MWT),whosemainresponsevariableisthemaximum
walk-ingdistance(6MWD),and cardiopulmonarystress test.The
6MWTisasimpleandinexpensive testthatiswidelyused
inchronic diseases suchaschronic obstructive pulmonary
diseaseandheartfailure.5
Recently,resultsofthe6MWTintheevaluationofpatients
with SCA were published6,7 in an attempt to assess the
adequacyoftheinstrumentinthisstudypopulation.A
pre-vious study showed that the determinants of the 6MWD
in SCA patients were low Hb level, low concentration of
fetal Hb and reduced deformability of red blood cells.8
However, thereare no studies in the Brazilian population,
which,beingmultiracial,doesnotallowthedirect
extrapo-lationofresultsobtainedinmoregeneticallyhomogeneous
populations.9
Inthissense,recurringcomplicationsandhospitalizations
appeartobeassociatedwithlowphysicalactivitylevels(PAL)
inpatientswithSCA.3
The 6MWT and specific questionnaires, with the main
advantagesofsafetyandlowcost,arewidelyusedto
evalu-atethephysicalcapacityandPAL.10–12AssessmentofthePAL
inpatientswithSCA,whetherbyquestionnairesorbydirect
testing,13,14showsatendencyofasedentarylifestyle.15
TheadaptedBorgscale16 isintendedtoclassifythe
sub-jectiveandindividualperceptionofeffortinperformingthe
6MWTinascalefrom0to10.Thismaybeanalyzedin
associa-tionwithexercise-induceddesaturation,thatis,thereduction
intranscutaneoussaturationoxygenbythreeormore
percent-agepointsaftertestingcomparedtobaseline,bothmeasured
usingaportabledigitaloximeter.17
Theaimofthisstudywastoestablishthedeterminantsof
the6MWDinchildrenandadolescentswithSCA,aswellas
tocomparePALandperformanceinthe6MWTbetweenSCA
patientstohealthycontrols.
Methods
Thisisacross-sectionalstudyconductedinanOutpatients’
Clinicofatertiaryteaching hospitalinnortheasternBrazil.
Thishospitalistheregionalreferralcenterforthetreatment
ofpatientswithSCA.
The project was approved by the Ethics Committee
of the Universidade Federal de Sergipe (UFS – protocol:
30661314.0.0000.5546). Thelegalguardians ofboth patients
andcontrolssignedawritteninformedconsentform.
Patientgroup
PatientswereenrolledfromOctober2014toMay2015.Ofthe
patientswithSCA(HbSS)confirmedbyHbelectrophoresis,
thosewhowerefrom6to18yearsold,insteady-state,with
nobloodtransfusionsinthepreviousthreemonthsandwith
noacutesymptomsforatleastonemonthpriortostudyentry
wereconsideredeligibleforthisstudy.Resultsofmolecular
testsandafamilystudywerenotavailable.Patientswith
neu-rologicalororthopedicimpairmentwereexcluded.
Clinicalandlaboratorydata
Hematological data (Hb, hematocrit, the red blood cell,
platelet,leukocyteandreticulocytecounts,indirectbilirubin,
mean corpuscular volume and lactate dehydrogenase), Hb
electrophoresis(fetalHbandHbS)andspirometrydatawere
obtainedfrom anelectronicdatabase createdespeciallyfor
thisresearch.Alltheexamswerecarriedoutwithinfourweeks
beforethe testandunderstableclinicalconditions.All the
testswereperformedatthecentrallaboratoryofthehospital,
usingstandardtechniquesandequipment.
Currentmedicationintake
All patients were taking folic acid supplement (2mg/day).
Thosewhoweretakinghydroxyureareceivedaninitialdose
of 15mg/kg/day and were receiving the standard dose of
20–35mg/kg/dayforatleast12months.18
Datacollection
Dataonvariablesconsideredpotentiallyassociatedwiththe
6MWDwere collected.Theseincludedage, gender,
hydrox-yureatherapy,bodymassindex(BMI),restingheartrate,heart
rateattheendofthetest,andtranscutaneousoxygen
satu-ration atrestandattheendoftesting.Furthermore,blood
tests were performed including Hb, hematocrit, red blood
cell,platelet,leukocyte,neutrophiland reticulocytecounts,
indirectbilirubin,meancorpuscularvolume,lactate
dehydro-genase,andHbfetalandHbSconcentrations.Moreover,the
scoresobtainedwiththeapplicationofthePhysicalActivity
QuestionnaireforOlderChildrenandAdolescents(PAQ-C)and
theadaptedBorgScale16wereincludedasvariables.
Physicalactivityquestionnaireforolderchildrenand
adolescents
Immediatelybeforethe6MWT,allthepatientsansweredthe
BrazilianversionofthePAQ-C,10,19 composedofnine
ques-tions about sports, games and other physical activities at
schoolandforrecreation.Thisquestionnaireaimstoprovide
acompletepictureofthetypeofactivitiesthattheparticipant
had been performingduringthe previoussevendays.Each
sedentary(2),moderatelyactive(3),active(4)orveryactive
(5).Thesumofscoreswascalculatedtodeterminethefinal
score.
The6-minutewalktest
The6MWTwasperformedaccordingtothestandardization
proposedbytheAmericanThoracicSociety.7,11Asingle6MWT
wasperformedalongaflatandstraightcorridorof30mona
hardsurface.Standardverbalencouragementwasusedduring
thetest.Patientswereinstructedtostopwhentheyfelttired.
Attheendoftesting,themaximumdistancewalked(6MWD)
wasdetermined,andthe perceptionofeffort wasrecorded
accordingtotheadaptedBorgscale.
Controlgroup
The control group consisted ofhealthy children and
ado-lescents enrolled in a local public school with similar
characteristics of the schools the cases usually attended.
Controlswerematchedwithcasesbyageandgender.They
performedthe6MWTandansweredthePAQ-C.
Data
analysis
Continuous quantitative variables are expressed as
means±standard deviation and range, and categorical
variables are expressed as percentages. Factors associated
with the 6MWD were evaluated using the Pearson
coeffi-cient.Variableswithp<0.20intheunivariateanalysiswere
selectedbyabackwardstepwisemodelandincludedinthe
multivariateanalysis.Anequationwasestablishedtopredict
the6MWDand its reliabilitywasassessedusingthe Bland
and Altman plot20 in a second independent group of six
patients(10%ofthesample).TheKolmogorov–Smirnovtest
wasusedtoverifyhowthedataweredistributed.ThePearson
correlationandindependentt-testwereusedforparametric
dataandSpearmancorrelationand Mann–Whitneytestfor
nonparametric data. The level of significance was set for
p<0.05.TheStatisticalPackagefortheSocialSciences(SPSS)
(Chicago,IL,USA)version13.0wasusedforanalysis.
Results
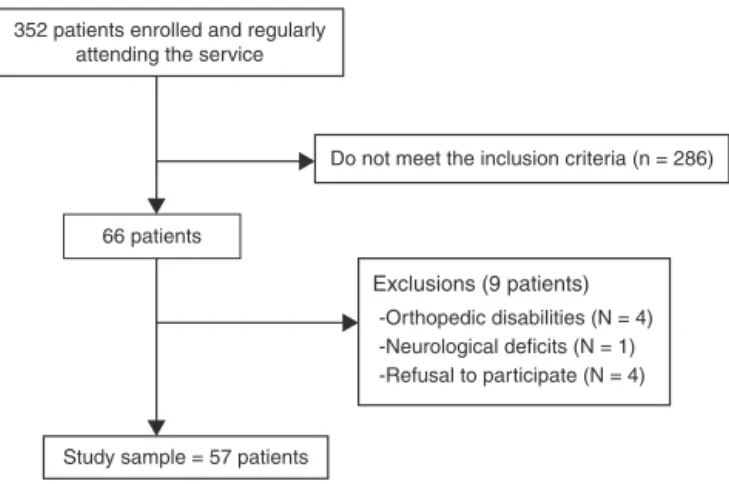
Sixty-sixpatientsinadatabaseofpatientswithSCAwho
reg-ularlyattendedthe clinic(n=352childrenandadolescents)
andwereconsideredeligiblewereselected,butninewerelater
excludedduetoorthopedicdisabilities,neurologicaldeficitsor
becausetheyrefusedtoparticipate(Figure1).
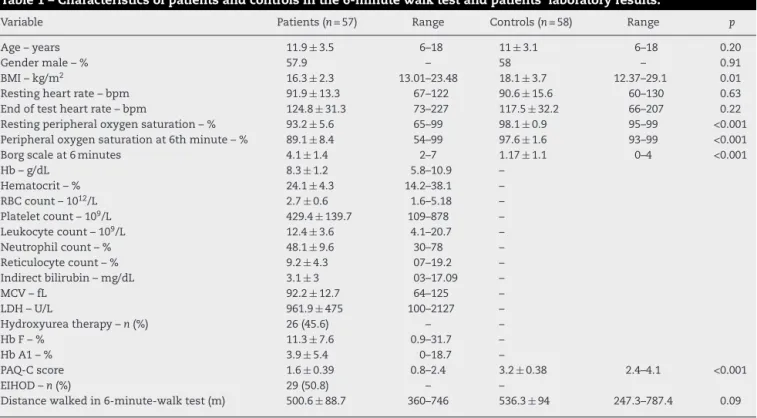
All57patientsand58controlscompletedthe6MWT
with-out any complications. The clinical characteristics of both
groups (SCA patients and healthy controls) are shown in
Table1.Thegroupsweresimilarinrespecttoageandgender,
aswellasforheartratebeforeandafterthe6MWT.
There were statistically significant differences between
groupsinrelationtoBMI,peripheraloxygensaturationatrest
andattheendofthe6MWTandthescoreobtainedusingthe
Borgscale.
352 patients enrolled and regularly attending the service
66 patients
Exclusions (9 patients)
-Orthopedic disabilities (N = 4) -Neurological deficits (N = 1) -Refusal to participate (N = 4)
Study sample = 57 patients
Do not meet the inclusion criteria (n = 286)
Figure1–Patientsincludedinthestudy.
Thefollowingvariableswithp<0.20wereselectedto
iden-tify which were independently associatedwith the 6MWD
in thepatients group: age (p<0.0001),BMI (p=0.118), heart
rate after the test (p=0.069), peripheral oxygen saturation
at the end ofthe test (p=0.125), hematocrit(p=0.188), red
bloodcellcount(p=0.056)andindirectbilirubin(p=0.008).By
multivariateanalysis,agewasfoundtobepositively
associ-ated(p<0.0001;beta:0.75)andBMIwasinverselyassociated
(p=0.047;beta−0.32)withthe6MWD.
The following equation was derived from the
mul-tivariate analysis, and aims to estimate the likely
6MWD from the variables age and BMI: estimated
6MWD=487.7+(age×18.3)−(BMI×12) with 6MWD being
expressedinmeters,ageinyearsandBMIinkg/m2.Asecond
and independentgroupofsixpatients(10%ofthesample)
was analyzedtoassess thereliabilityofthis equation.The
real 6MWDwas 480.5±63.1mwhich represented 99%±2%
of the estimated 6MWD. Thecorrelation between the real
6MWD and estimated 6MWDwas strong according to the
Spearmancoefficient(r=0.98).
AllparticipantscompletedthePAQ-C.Theaveragescore
obtained by patients was 1.6±0.39 with 63.1% of patients
withSCA categorizedasvery sedentaryand theremaining
36.9%assedentary(Table1).Therewasnosignificant
differ-encebetweenthesedentaryandverysedentaryindividualsin
respecttothe6MWD(530±84versus497±87m,respectively;
p=0.16;95%confidenceinterval:−14.19to80.75).Thescoreof
thecontrolswas3.2±0.38,with17.2%beingsedentary,75%
beingmoderatelyactiveand6.8%beingactive.
Table 2 shows the comparison ofthe PAL between the
different categories ofactivity identified bythe PAQ-C and
shows that patients with SCA reported a lower PAL in
all categories compared to the healthy controls. However,
the mean 6MWD was not significantly different between
patients(500.6±88.7m)andcontrols(536.3±94m)asshown
inFigure2.
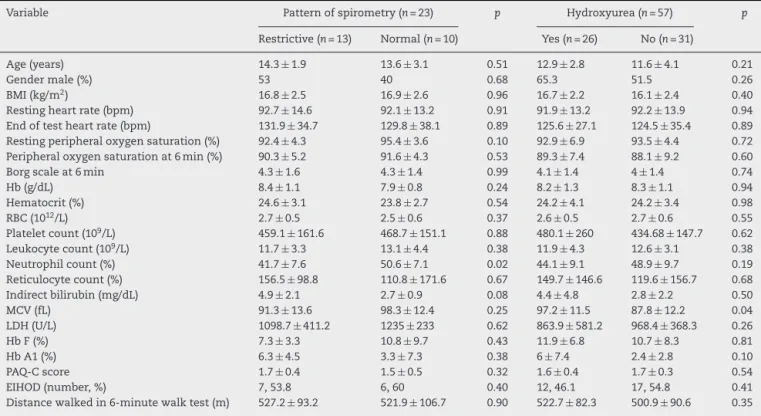
Spirometry was performedtoevaluatepulmonary
func-tion in23 ofthe 57patients (40.3%).Ofthese, arestrictive
pattern wasobservedin13patients(56.5%)andtheresults
werenormalin10patients(43.4%).Nosignificantdifference
wasfoundinrespecttothe6MWDoncomparingrestrictive
andnormalresultsofthespirometrytest.Exceptforthe
Table1–Characteristicsofpatientsandcontrolsinthe6-minutewalktestandpatients’laboratoryresults.
Variable Patients(n=57) Range Controls(n=58) Range p
Age–years 11.9±3.5 6–18 11±3.1 6–18 0.20
Gendermale–% 57.9 – 58 – 0.91
BMI–kg/m2 16.3±2.3 13.01–23.48 18.1±3.7 12.37–29.1 0.01
Restingheartrate–bpm 91.9±13.3 67–122 90.6±15.6 60–130 0.63 Endoftestheartrate–bpm 124.8±31.3 73–227 117.5±32.2 66–207 0.22 Restingperipheraloxygensaturation–% 93.2±5.6 65–99 98.1±0.9 95–99 <0.001 Peripheraloxygensaturationat6thminute–% 89.1±8.4 54–99 97.6±1.6 93–99 <0.001
Borgscaleat6minutes 4.1±1.4 2–7 1.17±1.1 0–4 <0.001
Hb–g/dL 8.3±1.2 5.8–10.9 –
Hematocrit–% 24.1±4.3 14.2–38.1 –
RBCcount–1012/L 2.7±0.6 1.6–5.18 –
Plateletcount–109/L 429.4±139.7 109–878 – Leukocytecount–109/L 12.4±3.6 4.1–20.7 –
Neutrophilcount–% 48.1±9.6 30–78 –
Reticulocytecount–% 9.2±4.3 07–19.2 –
Indirectbilirubin–mg/dL 3.1±3 03–17.09 –
MCV–fL 92.2±12.7 64–125 –
LDH–U/L 961.9±475 100–2127 –
Hydroxyureatherapy–n(%) 26(45.6) – –
HbF–% 11.3±7.6 0.9–31.7 –
HbA1–% 3.9±5.4 0–18.7 –
PAQ-Cscore 1.6±0.39 0.8–2.4 3.2±0.38 2.4–4.1 <0.001
EIHOD–n(%) 29(50.8) – –
Distancewalkedin6-minute-walktest(m) 500.6±88.7 360–746 536.3±94 247.3–787.4 0.09
Resultsareexpressedasmean,standarddeviationandrangeunlessotherwiseindicated.
BMI:bodymassindex;Hb:hemoglobin;RBC:redbloodcell;MCV:meancorpuscularvolume;LDH:lactatedehydrogenase;HbF:fetalhemoglobin; HbA1:hemoglobinA1;PAQ-C:PhysicalActivityQuestionnaireforolderchildrenandadolescents;EIHOD:exercise-inducedhemoglobinoxygen desaturation.
between the variables associated with the profile and the spirometryresults(Table3).
Twenty-six patients (45.6%) were taking hydroxyurea.
Therewasnosignificant differenceinthe6MWDwhenthe
groupswerecomparedaccordingtotheuseofthemedication.
Onlythe mean corpuscularvolume presentedasignificant
difference(Table3).
Discussion
Thisstudyidentifiedthatthevariablesindependently
associ-atedwiththe6MWDinthe6MWTofchildrenandadolescents
with SCA were age (positively) and BMI (inversely). Other
factorshad beenpreviouslyassociatedwith6MWD:lowHb
level,21increasedhemolysisandlowoxygensaturationatthe
beginningandaftertheexercise,17andlowlevelsoffetalHb
andreduceddeformabilityofredbloodcells.8However,these
associationswerenotfoundinthisstudy.Inaddition,an
equa-tiontoestimatethe6MWDofchildrenandadolescentswas
establishedandtested.
As expected, there was a significant difference in the
means of the BMIs between patients and controls.22 In
addition, the average 6MWD in the group with SCA was
numerically lower than the control group, albeit without
Table2–PhysicalactivitylevelsassessedbythePhysicalActivityQuestionnaireforOlderChildrenandAdolescents
(PAQ-C)ofpatientsandcontrols.
Patients Controls p
Mean±SD Median Min–Max Mean±SD Median Min–Max
Spare-timeactivity 0.77±0.37 0.8 0–1.6 2.37±0.55 2.3 1.4–3.7 <0.001
ActivityduringPEC 1.77±0.68 2 1–3 3.2±0.55 3.2 2–5 <0.001
Lunch-timeactivity 1.4±0.53 1 1–3 3.1±0.72 3 2–5 <0.001
Afterschoolactivity 1.77±0.92 1 1–4 3±0.61 3 2–4 <0.001
Eveningactivity 1.63±0.77 1 1–4 3.22±0.77 3 2–5 <0.001
Weekendactivity 2±0.75 2 1–3 3.44±0.77 4 2–5 <0.001
AFduringthelast7days 2.26±0.76 2 1–4 3.43±0.62 3 2–5 <0.001 AFduringeachdaylastweek 1.63±0.53 1.7 0.1–3 3.21±0.50 3.1 2.3–4.3 <0.001
Score 1.64±0.39 1.7 0.8–2.4 3.2±0.38 3.1 2.4–4.1 <0.001
Table3–Comparisonoflaboratoryand6-minutewalktestresultswiththeresultsofspirometryandtheuseof hydroxyurea.
Variable Patternofspirometry(n=23) p Hydroxyurea(n=57) p
Restrictive(n=13) Normal(n=10) Yes(n=26) No(n=31)
Age(years) 14.3±1.9 13.6±3.1 0.51 12.9±2.8 11.6±4.1 0.21
Gendermale(%) 53 40 0.68 65.3 51.5 0.26
BMI(kg/m2) 16.8±2.5 16.9±2.6 0.96 16.7±2.2 16.1±2.4 0.40 Restingheartrate(bpm) 92.7±14.6 92.1±13.2 0.91 91.9±13.2 92.2±13.9 0.94 Endoftestheartrate(bpm) 131.9±34.7 129.8±38.1 0.89 125.6±27.1 124.5±35.4 0.89 Restingperipheraloxygensaturation(%) 92.4±4.3 95.4±3.6 0.10 92.9±6.9 93.5±4.4 0.72 Peripheraloxygensaturationat6min(%) 90.3±5.2 91.6±4.3 0.53 89.3±7.4 88.1±9.2 0.60 Borgscaleat6min 4.3±1.6 4.3±1.4 0.99 4.1±1.4 4±1.4 0.74
Hb(g/dL) 8.4±1.1 7.9±0.8 0.24 8.2±1.3 8.3±1.1 0.94
Hematocrit(%) 24.6±3.1 23.8±2.7 0.54 24.2±4.1 24.2±3.4 0.98
RBC(1012/L) 2.7±0.5 2.5±0.6 0.37 2.6±0.5 2.7±0.6 0.55
Plateletcount(109/L) 459.1±161.6 468.7±151.1 0.88 480.1±260 434.68±147.7 0.62 Leukocytecount(109/L) 11.7±3.3 13.1±4.4 0.38 11.9±4.3 12.6±3.1 0.38 Neutrophilcount(%) 41.7±7.6 50.6±7.1 0.02 44.1±9.1 48.9±9.7 0.19 Reticulocytecount(%) 156.5±98.8 110.8±171.6 0.67 149.7±146.6 119.6±156.7 0.68 Indirectbilirubin(mg/dL) 4.9±2.1 2.7±0.9 0.08 4.4±4.8 2.8±2.2 0.50
MCV(fL) 91.3±13.6 98.3±12.4 0.25 97.2±11.5 87.8±12.2 0.04
LDH(U/L) 1098.7±411.2 1235±233 0.62 863.9±581.2 968.4±368.3 0.26
HbF(%) 7.3±3.3 10.8±9.7 0.43 11.9±6.8 10.7±8.3 0.81
HbA1(%) 6.3±4.5 3.3±7.3 0.38 6±7.4 2.4±2.8 0.10
PAQ-Cscore 1.7±0.4 1.5±0.5 0.32 1.6±0.4 1.7±0.3 0.54
EIHOD(number,%) 7,53.8 6,60 0.40 12,46.1 17,54.8 0.41
Distancewalkedin6-minutewalktest(m) 527.2±93.2 521.9±106.7 0.90 522.7±82.3 500.9±90.6 0.35
Resultsareexpressedasmean,standarddeviationandrangeunlessotherwiseindicated.
BMI:Bodymassindex;Hb:hemoglobin;RBC:redbloodcells;MCV:meancorpuscularvolume;LDH:lactatedehydrogenase;HbF:fetalhemoglobin; HbA1:hemoglobinA1;PAQ-C:PhysicalActivityQuestionnaireforolderchildrenandadolescents;EIHOD:exercise-inducedhemoglobinoxygen desaturation.
Patients Controls
850
750
650
550
450
350
Distance (m)
250
Figure2–Maximumdistancesinthe6-minutewalktestof patientsandcontrols(Mann–Whitneytest).
statisticalsignificance.Inarecentstudy,adultswithSCAhad 6MWDbelowthevalueexpectedforthe 6MWT.23 Although
therewasnostatisticallysignificantdifferenceinthemeans
of6MWDbetween the patients and controlsin this study,
it was observedthat the perceived effort measured bythe
Borg scale was higher in patients with SCA. A previous
studyshowedthatthe6MWDwaspositivelyassociatedwith
maximaloxygenconsumptionandnegativelytothedegreeof
hypertension.24
Thisstudy demonstrated that children and adolescents
withSCAhadlowerPALthanhealthyindividuals,thus
corrob-oratingapreviousstudy,whichfoundthatSCApatientshad
physicalcapacitybelowthatexpectedfortheirage.13Another
studyshowedthatchildrenwithSCAhadlowerenergy
expen-diture with physical activity than healthy children, which,
incombinationwithgrowthimpairment,indicatesachronic
energydeficiency.25
Recurrent painful crises may have contributed to the
impairmentofphysicalcapacity.26Paininterferesinthe
func-tionalstatus27andpredisposesaffectedindividualstoamore
sedentary lifestyle,lessmuscular work,whichmay leadto
peripheralmuscleweaknessandtoreducedfunctional
capac-ity,aswasobservedinthisstudy,eventhoughthetestwas
accomplished inpatientswithout painfulcrisesforatleast
onemonth.Inapreviousstudy,theauthorsevaluated30
chil-drenandadolescentswithSCAbyexercisetestingwiththe
resultsshowingmoderatetosevereimpairmentofPAL
corre-latedtothebaselineHblevel.6
Thereiscompellingevidencethathydroxyureacanreduce
complicationsand hospitalizationsinchildrenwithSCAat
allages.18Nevertheless,therewasnosignificantdifferencein
the6MWDorPALcorrelatedwiththeuseofthismedication.
Thisfindingmaybejustifiedbythefactthattheindicationof
hydroxyureaisrestrictedtopatientswithmoreacute
com-plications,which, inthe longterm,resultinchronicorgan
andsysteminvolvement,withpossiblerepercussionsonthe
6MWT.
AlthoughpatientswithSCAeventuallypresentlung
func-tion impairment, in this study there was no significant
andnormalpatternsbyspirometry,thuscorroborating
previ-ousresults.8,23
SCApatientsingeneraladapttochronicanemiaandthe
consequent lower tissue oxygenation. Thus, compensatory
mechanisms, such as increased heart rate and decreased
peripheralvascular resistancethat increases the supply of
oxygen totissues, resultin transcutaneous oxygen
satura-tionneartonormal.17 However,thispartialadaptationmay
beinsufficient,especiallyduringexercise,whentheneedfor
higheroxygensaturationincreasesthedemandforenergy.
Physicalexerciseinducesnotablemetabolicchanges,such
aslactateproductionbytheactivemuscles. Thus,reduced
physicalcapacitycanbeexplainedbythepresenceof
ane-mia,becauselevelsofHbbelownormalvaluesinducerapid
transitionfromaerobictoanaerobicrespirationduring
exer-cise, which can trigger the polymerization of Hb S and
promote microvascular occlusions. Furthermore, although
habitualmoderate exercisecan improve immunefunction,
intenseexercisecancausetemporarydysfunctionwith
tran-sientincreasesincirculatingcytokines,28reducingbloodflow
inthemicrocirculationandcausingveno-occlusivecrises.29
Alimitationofthisstudy wasusingclinical and
labora-torydatafrommedicalrecordsandnotthoseevaluatedon
thesamedayofthetest.However,thetestswerecarriedoutin
steady-stableandthe6MWTwasperformedunderthesame
conditions. Moreover,PAL wasbased on self-reported data
andthusmightbebiasedbysociallydesirableresponses.A
studyofpatientswithfibromyalgia30showedthatthereported
information can overstate the PAL when confronted with
data acquired using accelerometers,indicating no
associa-tionbetweendirectandindirectmeasuresintheevaluationof
thePAL.However,althoughitisnottheonlyavailableoption,
self-reportingisapracticalandcheapmannertoacquirethis
information.Furthermore,byusingthesamestrategyinboth
thestudyandcontrolgroups,thepotentialbiasisequally
dis-tributedinbothgroups.
Conclusion
This study found that the determinants of the 6MWD in
childrenandadolescents withSCAwere age(positive
rela-tionship)andBMI(inverserelationship).Furthermore,itwas
observedthattheevaluatedpatientshavelowerPALcompared
tohealthyindividuals.
There was no statistically significant difference in the
6MWD between study and control groups. None of the
hematologicparameterswasassociatedwiththe6MWT
per-formance.Itispossiblethataspectsrelatedtocomplicationsof
SCAmayberelatedtothelowPALvaluesandphysicalcapacity
inthisstudy;thisassociationshouldbestudiedinthefuture.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. StuartMJ,NagelRL.Sickle-celldisease.Lancet. 2004;364(9442):1343–60.
2.ReesDC,WilliamsTN,GladwinMT.Sickle-celldisease. Lancet.2010;376(9757):2018–31.
3.PettoJ,deJesusJB,VasquesLMR,PinheiroRLS,OliveiraAM, SpinolaKAB,etal.Restingbloodlactateinindividualswith sicklecelldisease.RevBrasHematolHemoter.
2011;33(1):26–30.
4.vanBeersEJ,vanderPlasMN,NurE,BogaardH-J,van SteenwijkRP,BiemondBJ,etal.Exercisetolerance,lung functionabnormalities,anemia,andcardiothoracicratioin sicklecellpatients.AmJHematol.2014;89(8):819–24.
5.GuyattGH,SullivanMJ,ThompsonPJ,FallenEL,PugsleySO, TaylorDW,etal.The6-minutewalk:anewmeasureof exercisecapacityinpatientswithchronicheartfailure.Can MedAssocJ.1985;132(8):919–23.
6.LiemRI,NevinMA,PrestridgeA,YoungLT,ThompsonAA. Functionalcapacityinchildrenandyoungadultswithsickle celldiseaseundergoingevaluationforcardiopulmonary disease.AmJHematol.2009;84(10):645–9.
7.ConnesP,MacHadoR,HueO,ReidH.Exerciselimitation, exercisetestingandexerciserecommendationsinsicklecell anemia.ClinHemorheolMicrocirc.2011;49(1-4):
151–63.
8.WaltzX,RomanaM,Hardy-DessourcesM-D,LamarreY, Divialle-DoumdoL,PetrasM,etal.Hematologicaland hemorheologicaldeterminantsofthesix-minutewalktest performanceinchildrenwithsicklecellanemia.PLoSOne. 2013;8(10):e77830.
9.BandeiraFM,LealMC,SouzaRR,FurtadoVC,GomesYM, MarquesNM.Hemoglobin“S”positivenewborndetectedby cordbloodanditscharacteristics.JPediatr(RioJ).
1999;75(3):167–71.
10.KowalskiKC,CrockerPRE,FaulknerRA.Validationofthe PhysicalActivityQuestionnaireforolderchildren.Pediatr ExercSci.1997;9(2):174–86.
11.CrapoRO,CasaburiR,CoatesAL,EnrightPL,MacIntyreNR, McKayRT,etal.ATSstatement:guidelinesforthesix-minute walktest.AmJRespirCritCareMed.2002;166(1):111–7.
12.DuH,NewtonPJ,SalamonsonY,Carrieri-KohlmanVL, DavidsonPM.Areviewofthesix-minutewalktest:its implicationasaself-administeredassessmenttool.EurJ CardiovascNurs.2009;8(1):2–8.
13.HostynSV,CarvalhoWB,JohnstonC,BragaJA.Evaluationof functionalcapacityforexerciseinchildrenandadolescents withsicklecelldiseasethroughtheSixMinuteWalkTest.J Pediatr(RioJ).2013;89(6):588–94.
14.MaroufR,BehbehaniN,ZubaidM,AlWazzanH,ElMuzainiH, AbdullaR,etal.Transthoracicechocardiographyand 6-minutewalktestinKuwaitisicklecelldiseasepatients. MedPrincPract.2014;23(3):212–7.
15.PlattOS,BrambillaDJ,RosseWF,MilnerPF,CastroO, SteinbergMH,etal.Mortalityinsicklecelldisease.Life expectancyandriskfactorsforearlydeath.NEnglJMed. 1994;330(23):1639–44.
16.CarvalhoVO,BocchiEA,GuimarãesGV.TheBorgscaleasan importanttoolofself-monitoringandself-regulationof exerciseprescriptioninheartfailurepatientsduring hydrotherapy.Arandomizedblindedcontrolledtrial.CircJ. 2009;73(10):1871–6.
17.CampbellA,MinnitiCP,NouraieM,ArtetaM,RanaS, OnyekwereO,etal.Prospectiveevaluationofhaemoglobin oxygensaturationatrestandafterexerciseinpaediatric sicklecelldiseasepatients.BrJHaematol.2009;147(3):352–9.
18.StrouseJJ,HeeneyMM.Hydroxyureaforthetreatmentof sicklecelldisease:efficacy,barriers,toxicity,and managementinchildren.PediatrBloodCancer. 2012;59(2):365–71.
19.SilvaRC,MalinaRM.Níveldeatividadefísicaem
20.BlandJM,AltmanDG.Statisticalmethodsforassessing agreementbetweentwomethodsofclinicalmeasurement. Lancet.1986;1(8476):307–10.
21.SettyBN,StuartMJ,DampierC,BrodeckiD,AllenJL.
Hypoxaemiainsicklecelldisease:biomarkermodulationand relevancetopathophysiology.Lancet.2003;362(9394):1450–5.
22.Al-SaqladiA-WM,CipolottiR,FijnvandraatK,BrabinBJ. Growthandnutritionalstatusofchildrenwithhomozygous sicklecelldisease.AnnTropPaediatr.2008;28(3):165–89.
23.OharaDG,RuasG,WalshIA,CastroSS,JamamiM.Lung functionandsix-minutewalktestperformanceinindividuals withsicklecelldisease.BrazJPhysTher.2014;18(1):79–87.
24.AnthiA,MachadoRF,JisonML,Taveira-DaSilvaAM,RubinLJ, HunterL,etal.Hemodynamicandfunctionalassessmentof patientswithsicklecelldiseaseandpulmonary
hypertension.AmJRespirCritCareMed.2007;175(12):1272–9.
25.BardenEM,ZemelBS,KawchakDA,GoranMI,
Ohene-FrempongK,StallingsVA.Totalandrestingenergy
expenditureinchildrenwithsicklecelldisease.JPediatr. 2000;136(1):73–9.
26.OharaDG,RuasG,CastroSS,MartinsPR,WalshIA.
Musculoskeletalpain,profileandqualityoflifeofindividuals withsicklecelldisease.RevBrasFisioter.2012;16(5):
431–8.
27.TaylorLE,StottsNA,HumphreysJ,TreadwellMJ,Miaskowski C.Areviewoftheliteratureonthemultipledimensionsof chronicpaininadultswithsicklecelldisease.JPain SymptomManage.2010;40(3):416–35.
28.GleesonM.Immunefunctioninsportandexercise.JAppl Physiol(1985).2007;103(2):693–9.
29.MakisAC,HatzimichaelEC,BourantasKL.Theroleof cytokinesinsicklecelldisease.AnnHematol. 2000;79(8):407–13.