REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologiawww.sba.com.br
SCIENTIFIC
ARTICLE
Effects
of
lidocaine
and
magnesium
sulfate
in
attenuating
hemodynamic
response
to
tracheal
intubation:
single-center,
prospective,
double-blind,
randomized
study
Fabricio
Tavares
Mendonc
¸a
∗,
Lucas
Macedo
da
Grac
¸a
Medeiros
de
Queiroz,
Cristina
Carvalho
Rolim
Guimarães,
Alexandre
Cordeiro
Duarte
Xavier
CentrodeEnsinoeTreinamentodoHospitaldeBasedoDistritoFederal,UnidadedeAnestesiologiaeMedicinaPerioperatória, Brasília,DF,Brazil
Received3March2015;accepted17August2015 Availableonline22November2016
KEYWORDS
Laryngoscopy; Trachealintubation; Lidocaine;
Magnesiumsulphate; Cardiovascular physiological phenomena
Abstract
Backgroundandobjectives: Hemodynamicresponsetoairwaystimuliisacommonphenomenon anditsmanagementisimportanttoreducethesystemicrepercussions.Theobjectiveofthis studyistocomparetheefficacyofintravenousmagnesiumsulfateversuslidocaineonthisreflex hemodynamicsafterlaryngoscopyandtrachealintubation.
Methods:Thissingle-center,prospective,double-blind,randomizedstudyevaluated56patients ASA1or2,aged18---65years,scheduledforelectivesurgeriesundergeneralanesthesiawith intubation.Thepatientswereallocatedintotwogroups:GroupFreceived30mg·kg−1of
mag-nesiumsulphateandGroupL,2mg·kg−1oflidocaine,continuousinfusion,immediatelybefore
theanestheticinduction.Bloodpressure(BP),heartrate(HR),andbispectralindex(BIS)were measuredinbothgroupsatsixdifferenttimesrelatedtoadministrationofthestudydrugs.
Results:InbothgroupstherewasanincreaseinHRandBPafterlaryngoscopyandintubation, comparedtobaseline.GroupMshowedstatisticallysignificantincreaseinthevaluesofsystolic anddiastolicbloodpressureafterintubation,whichwasclinicallyunimportant.Therewasno differenceintheBISvaluesbetweengroups.Amongpatientsreceivingmagnesiumsulfate,three (12%)hadhighbloodpressureversusonlyoneamongthosereceivinglidocaine(4%),withno statisticaldifference.
∗Correspondingauthor.
E-mail:[email protected](F.T.Mendonc¸a).
http://dx.doi.org/10.1016/j.bjane.2015.08.004
Conclusion: Magnesiumsulfateandlidocainehavegoodefficacyandsafetyforhemodynamic managementinlaryngoscopyandintubation.
©2016SociedadeBrasileiradeAnestesiologia.Publishedby ElsevierEditoraLtda.Thisisan openaccessarticleundertheCCBY-NC-NDlicense( http://creativecommons.org/licenses/by-nc-nd/4.0/).
PALAVRAS-CHAVE
Laringoscopia; Intubac¸ão intratraqueal; Lidocaína;
Sulfatodemagnésio; Fenômenos
fisiológicos cardiovasculares
Osefeitosdalidocaínaedosulfatodemagnésionaatenuac¸ãodaresposta hemodinâmicaàintubac¸ãoorotraqueal:estudounicêntrico,prospectivo, duplamenteencobertoealeatorizado
Resumo
Justificativaeobjetivos: Arespostahemodinâmicaaosestímulosdasviasaéreaséum fenô-menocomumeseucontroleéimportanteparadiminuirasrepercussõessistêmicas.Oobjetivo deste trabalhoé compararos efeitos daadministrac¸ão endovenosa desulfato demagnésio versuslidocaínanahemodinâmicadessereflexoapósalaringoscopiaeintubac¸ãoorotraqueal.
Métodos: Esteestudoduplamenteencoberto,aleatorizado,unicêntricoeprospectivoavaliou 56pacientes,ASA1ou2,entre18e65anos,escaladosparacirurgiaseletivassobanestesia geral comintubac¸ão orotraqueal. Foramalocados em dois grupos,o M recebeu30mg·kg−1
de sulfatode magnésioeoL, 2mg·kg−1 delidocaína, eminfusão contínua,imediatamente
antesdainduc¸ãoanestésica.Osvaloresdepressãoarterial(PA),frequênciacardíaca(FC)e índicebiespectral(BIS)foramaferidosnosdoisgruposemseismomentosrelacionadoscoma administrac¸ãodosfármacosdoestudo.
Resultados: EmambososgruposhouveaumentonaFCePAapósalaringoscopiaeintubac¸ão, emrelac¸ãoaosvaloresbasais.NoGrupoMobservou-seelevac¸ãoestatisticamentesignificativa, mas clinicamentepoucoimportante, nosvalores daspressõesarteriaissistólicae diastólica apósaintubac¸ão.Nãohouvediferenc¸anosvaloresdeBISentreosgrupos.Dospacientesque receberamosulfatodemagnésio,3(12%)apresentaramepisódiodehipertensão,aopassoque apenasumdosquereceberamlidocaína(4%)apresentouessesinal,semdiferenc¸aestatística.
Conclusão:Sulfatodemagnésioealidocaínaapresentamboaeficáciaeseguranc¸anocontrole hemodinâmicoàlaringoscopiaeintubac¸ão.
©2016SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Este ´eum artigo OpenAccess sobumalicenc¸aCCBY-NC-ND( http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
The hemodynamic response to stimuli evoked by laryn-goscopyandintubationisacommonphenomenon,resulting fromthereleaseofendogenouscatecholaminesreflexively totheupperairwayafferentswhenstimulated.1This inap-propriate response may increase perioperative morbidity and mortality, especially in patients with coexisting dis-ease,particularlypatientswithcardiovasculardisease.The management of this defensive reflex is essential because it prevents adverse events, suchas tachycardia, systemic hypertension, pulmonary hypertension, and arrhythmias, whichmayresultinstrokeormyocardialinfarctionresulting fromhemodynamicinstabilityproducedbylaryngoscopyand intubation.Manydrugsarethesubjectofstudies,including thosewithgoodresults,suchasmagnesium sulfate1---3 and lidocaine.4---6
The magnesium sulfatemechanism ofaction for hemo-dynamic response attenuation appears to result from the inhibition of catecholamine release from the adrenal medulla,maintainstheplasmaconcentrationofepinephrine practicallyunchanged,andalsoreducestheincreased cir-culatingnorepinephrinewhencomparedtothatofacontrol group.2 It also has a systemic and coronary vasodilation effect by antagonizing calcium ion in vascular smooth
muscle.7Asforlidocaine,whenusedsystemically,ithasan antagonisticactiononsodiumchannelsandNMDAreceptors, reducesthereleaseofsubstanceP,hasglycinergicaction, whichdecreasestheairwayreactivity.8,9
Theaimofthisstudywastocomparetheeffectsof intra-venousmagnesiumsulfatewithlidocaineonhemodynamics duringintubation.
Material
and
methods
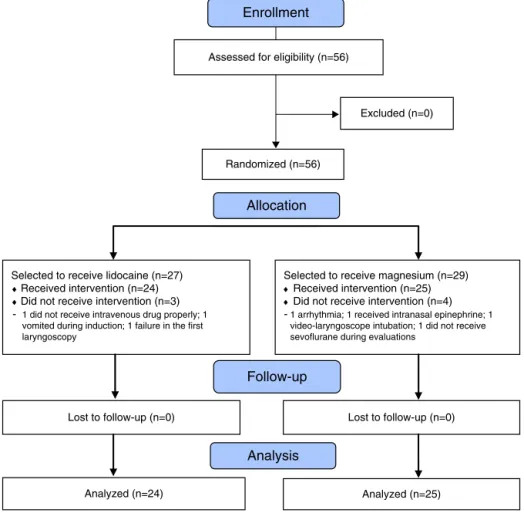
This prospective,randomized, doubleblind, single-center studywas approvedby the ResearchEthics Committee ----FEPECS/SES-DF ---- under the opinion number 799,112 on September 22, 2014, and is identified in the Plataforma Brasil (http://aplicacao.saude.gov.br/plataformabrasil) as CAAENo33365114.7.0000.5553 andregistered in Clinical-Trials(NCT02359370).Afterwritten informedconsentwas given,56patients,ASA1or2,agedbetween18---65years, scheduledforelective surgerywithorotrachealintubation (OTI)wereassessedforeligibility,betweenSeptemberand November2014attheHospitaldeBasedoDistritoFederal
(Fig.1).
Follow-up
Analysis
Assessed for eligibility (n=56)
Excluded (n=0)
Analyzed (n=24) Lost to follow-up (n=0) Selected to receive lidocaine (n=27)
♦Received intervention (n=24) ♦Did not receive intervention (n=3)
-1 did not receive intravenous drug properly; 1 vomited during induction; 1 failure in the first laryngoscopy
Lost to follow-up (n=0) Selected to receive magnesium (n=29)
♦Received intervention (n=25) ♦Did not receive intervention (n=4)
-1 arrhythmia; 1 received intranasal epinephrine; 1 video-laryngoscope intubation; 1 did not receive sevoflurane during evaluations
Analyzed (n=25) Randomized (n=56)
Allocation Enrollment
Figure1 Flowchartofrandomization.
disease,atrioventricularblockofanydegree,knowncardiac arrhythmias,heartfailure,renalfailureofanykind,onbeta blockers or calcium channel blockers, expected difficult intubation,andBMI≥35kg·m−2wereexcluded.Patientswho
hadundergoneneuraxialblockbeforetheanesthetic induc-tion, who refused to participate after informed consent presentation, required two or more attempts at laryn-goscopy for orotrachealtube placement,as wellas those withanyother conditionthat,intheresearchers’opinion, couldpose riskstothepatientorinterferewiththestudy objectiveswerealsoexcluded.
Ofthe56patientsselectedforthestudyaccordingtothe inclusioncriteria,sevenwereexcludedduringassessments (Fig.1)for patients’ safety reasonsor issues notcovered by theProtocol. Four patients fromGroup M (magnesium sulfate)wereexcludedduetofrequentventricular extrasys-toles,introductionof nasalswabofadrenalinebeforethe endoftheassessments,intubationwithvideo-laryngoscope andlack of sevofluranein thevaporizer notchecked dur-ingtheevaluations.ThreepatientsfromGroupL(lidocaine) were excluded due to leakage of drugs (loose fixation of venous access), anotherdue tovomiting withconsequent aspirationundermaskventilation,andanotherfor intuba-tionfailureinthefirstlaryngoscopy.
Patientswhomettheinclusioncriteriawereselectedand receivedan identification number, according tothe order ofinclusionin thestudy.Theinvestigatorsresponsible for assessingthestudy periodwereblindtogroup allocation.
Patients were randomized using a list of numbers gener-ated in random order. An investigator not involved with dataassessment randomlyassignedthepatients toone of two groups using sealed envelopes containing a numeric sequencegeneratedinrandomorder,recordedtheirdatain medicalcharts,preparedtheinfusion pumpanddelivered itintheoperatingroom,sotheinvestigatorswereunaware ofwhichdrugisused.
Intheoperatingroom, thepatientwasfirstidentified, followed by standard monitoring with electrocardiogram (ECG),saturationofperipheraloxygen(SpO2),noninvasive
bloodpressure(NIBP),andbispectralindex(BIS). Venipunc-turewasperformedatthediscretionoftheanesthesiologist, in accordance with the surgery/anesthesia scheduled (admission time). Subsequently, midazolam 0.05mg·kg−1
wasusedaspremedication.Aftertwominutes(time2 post-MDZ), infusion with the study drug was started with 2% lidocaine (2mg·kg−1) without vasoconstrictor (Xylestesin,
Cristália®)ormagnesiumsulphate(30mg·kg−1),bothdiluted
in 15mL of solution and infused in 10min by continuous infusionpump(CIP).Attheendofinfusion(CIPendtime), pre-oxygenationandanestheticinductionwithintravenous fentanyl2mcgkg−1 wereperformed,followed bypropofol
2mg·kg−1androcuronium0.6mg·kg−1(post-inductiontime).
administered.Afterorotrachealintubation,anesthesiawas maintainedwith2%inhaledsevoflurane,andnew measure-ments weretaken three and six minutes afterintubation (3′ post-OTIand6′ post-OTI).Hypertensionwasconsidered whentheBPvalueswere20%abovebaselinevaluesorSBP >140mmHg. Hypotension was considered when BP values werelowerthan20%ofbaselineorSBP<90mmHg. Tachycar-diawasconsideredwhenHRwashigherthan20%ofbaseline orHR>100bpm.Bradycardia wasconsideredwhenHR val-ueswerelowerthan50bpm.
The primaryendpoint wasto determine the effectsof lidocaineandmagnesiumsulfate(GroupLvs.GroupM)on SBPimmediatelyafterintubation(post-OTI).Thesecondary endpointsweretheassessmentofchangesinSBP,DBP,HR, andBISbeforeandaftertheadministrationofstudydrugs, itschangeswithinsixminutesafterintubation,aswellthe identificationofadverseeventswiththeuseofboth tech-niques.
Considering the primary outcome of SBP immediately after intubation (post-OTI PAS), a 24% variance with20% effectdifference, two-tailedalpha errorof 5%andpower of80%,thecalculatedsamplesizewouldbe25patientsin eachgroup.
StatisticalanalysiswasperformedwiththeXLSTAT soft-warefor Excel.Shapiro---Wilkstest wasusedtodetermine the normal distribution of continuous variables. All con-tinuous variables were expressed as mean and standard deviation. Categorical variables were expressed as num-ber of patients or percentage (%). Quantitative variables withnormaldistributionwereassessedusingtheStudent’s
t-test for independent samples; variables without normal distribution were assessed using the Mann---Whitney non-parametric U test; and categorical variables using the chi-squaretestorFisher’sexacttest,asappropriate.Ap -value<0.05wasconsideredsignificant.Datawereexpressed as mean±SD (mean, standard deviation) or absolute numbers.
Results
Therewasnostatisticaldifferenceinbothgroupsregarding age, sex, weight, height, and BMI, as well as physical status classification by ASA. The drugs taken as antihy-pertensive agents by the study patients were diuretics, angiotensin receptor blockers (ARBs), and angiotensin-converting enzyme (ACE) inhibitors, with no statistical differenceinthenumberofhypertensivepatientsorusers ofdrugsfromeachmedicationclass(Table1).
TherewasnostatisticaldifferencebetweengroupsinHR, SBP,DBPandBISvaluesatadmission;aftermidazolam, infu-sionpump,andinduction times.Therewasan increasein HR,SBPandDBPinbothgroupsafterlaryngoscopycompared tobaseline.GroupMhadastatisticallysignificantincreasein SBP(p=0.018)andDBP(p=0.0467)post-OTI(Fig.2),butof littleclinicalimportance.Therewerehigherpressurevalues inthe3rdand6thminutespost-OTIinGroupM, but with-outstatistical significance. After this period,both groups showedagradualreductioninbloodpressurevalues.There wasatrendtohigherHRvaluesinthecontinuousinfusion post-pumptime(CIP end)inGroup M, alsowithno statis-ticaldifference.There wasnostatisticaldifferencein HR valuesattimepoints(Fig.3).Therewasanincreaseinheart rateafterlaryngoscopyinbothgroups,followedbygradual decline.RegardingBISvalues,both groupsshowed a simi-largradualdecreasetrenduptotheinduction,followedby anincreaseafterintubation,without statisticaldifference (Fig.4).
TherewasatendencytohypotensioninGroupL,defined asadecreaseover20%ofthebaselineSBPorSBP<90mmHg, but without statistical significance (p=0.062). Nopatient receivedatropineorephedrine.InGroupM,threepatients (12%)had episodesof hypertension (increase in SBP>20% ofbaseline)comparedtoonepatient(4%)inGroupL,with nostatisticaldifferencebetweengroups.InGroupM,seven patients(28%)hadtachycardiacomparedtothreepatients
Table1 Demographicandclinicaldataofpatients.
GroupL GroupM p
Age(years) 48.54±12.28 43.32±13.63 0.1651
Weight(kg) 71.30±14.48 71.08±13.29 0.95
Height(cm) 164±10 168±9 0.1328
BMI(kgm−2) 26.47±3.6 25.22±3.69 0.2372
Sex(n) 0.879
Male 13 13
Female 11 12
Physicalstate(n) 0.32
ASAI 11 15
ASAII 13 10
SAH(n) 7 3 0.098
Drugsused(n)
Diuretics(n) 4 1 0.143
ARA 4 3 0.641
ACE 3 0 0.068
Valuesareexpressedasmean±DPandnumbers;therewasnostatisticaldifferencebetweengroups.BMI,bodymassindex;SAH,systemic
0
Admission 2’ post-MDZ
CIP end post-Ind post-OTI
3’ post-OTI 6’ post-OTI 20
40 60 80 100 120 140 160
SBP-L SBL-M DBP-L DBP-M
∗ ∗
Figure 2 Mean systolic blood pressure (SBP) and diastolic bloodpressure(DBP)values.Therewasstatisticaldifferencein thepost-OTItime(*p=0.0180forSBP,and*p=0.0467toDBP). MDZ,midazolam;CIP,continuousinfusionpump;Ind,anesthetic induction;OTI,orotrachealintubation.
65.00
Admission 2’ post-MDZ CIP end Ind
post-OTI
3’ post-OTI 6’ post-OTI 70.00
75.00 80.00 85.00 90.00 95.00
HR-L HR-M
Figure3 Meanheart ratevalues.Therewerenostatistical differences.HR, heartrate;MDZ,midazolam; CIP,continuous infusionpump;Ind,anestheticinduction;OTI,orotracheal intu-bation.
(12%)inGroupL,alsowithnostatisticaldifference.There werenoepisodesofbradycardiainbothgroups(Table2).
Discussion
Similar to the results reported by Ramires et al.10 and Nooareietal.7,weobservedatendencytoincreasedheart rate in Group M at the end of magnesium sulfate infu-sion,whichcanbe physiologicallyexplainedbythedirect vasodilatoreffectofthisdrug.2,7,10,11Despiteitsvasodilator properties,therewasagreatertendencytohypotensionin
0
Admission 2’ post-MDZ
CIP end post-Ind post-OTI
3’ post-OTI 6’ post-OTI
10 20 30 40 50 60 70 80 90 100
BIS-L BIS-M
Figure 4 Meanbispectral index(BIS) values; there was no statisticaldifference.MDZ,midazolam;CIP,continuousinfusion pump;Ind,anestheticinduction;OTI,orotrachealintubation.
Table2 Intraoperativedata.
GroupL GroupM p
(n=24) (n=25)
Ephedrine(n) 0 0 1.0
Atropine(n) 0 0 1.0
Hypotension(n) 13 7 0.062 Hypertension(n) 1 3 0.317
Tachycardia(n) 3 7 0.178
Bradycardia(n) 0 0 1.0
Dataareexpressedasnumberofpatients.GroupG,lidocaine;
GroupM,magnesiumsulfate.Therewasnostatisticaldifference
betweengroups.
GroupL,butwithoutstatisticalsignificance.Therewasno useofvasopressorinpatients,ashypotensionwasobserved immediatelybeforelaryngoscopy,atimeknowntoincrease vasomotortone.
Airway management during laryngoscopy and intuba-tioncausephysiological changesthat canbeharmful toa numberofpatients.12Pharynx,larynx,trachea,andcarina arehighlyinnervatedbysympatheticandparasympathetic fibers. Defensive reflex responses to airway manipulation include tachycardia, bronchospasm,increasedblood pres-sure and intracranial pressure. Studies have shown that laryngoscopy causes 20mmHg increase in systolic blood pressure12---17andasimpletrachealsuctioncausesatleasta 5mmHgincreaseinintracranialpressure.12,18,19
InasimilarstudyperformedbyNooraeietal.,theauthors compared the effect of lidocaine and magnesium sulfate onthe hemodynamic variables of laryngoscopy andfound bettercontrolofbloodpressurevalueswithmagnesium sul-fate,althoughwithincreasedHR.7
Puri et al.1 also compared the effects of magnesium sulfateandlidocaineoncardiovascularresponseto intuba-tion in coronaryartery disease patients undergoing CABG and found better attenuation of the hemodynamic varia-bleswithmagnesiumsulfate.Thehemodynamicresultswere highercardiacindex,minimumincreaseinHR,and signifi-cantreductioninsystemicvascularresistance.Inthisstudy, theauthorsobservedthatthreepatientsinGroupLshowed STsegmentdepression,whilethisfindingwasnotobserved inGroupM.
Theaboveresultsdivergefromthepresentstudy proba-blyduetothedifferenceinuseddosesofthedrugsstudied. Noorei et al.7 used magnesium sulfate (60mg·kg−1) and
lidocaine (1.5mg·kg−1) and Puri et al.1 used magnesium sulfate(50mg·kg−1)andlidocaine(1mg·kg−1).Weused
mag-nesium sulfate (30mg·kg−1) because, according to Panda
etal.,3itistheoptimaldrugdosetoattenuatethe hemo-dynamicresponsetointubationinhypertensivepatients.In thisstudydoseswerecomparedat30,40,and50mg·kg−1of
magnesiumsulfateand1.5mg·kg−1oflidocaineanditwas
concludedthatmagnesiumsulfatemaintainsbetterstability comparedtothepretreatmentwithlidocaineandthatthe useofdosesat 40and50mg·kg−1 ledtomoreepisodesof
hypotensionrequiringintervention.3 Therefore,ourchoice wastousemagnesiumsulfate30mg·kg−1,inordertoavoid
complicationsduringtheprocedure.Thedose oflidocaine waschosenbasedontheworkbyVivancosetal.4
Ourstudywasperformedwithhealthypatientsscheduled for elective surgeries.Our techniqueof anesthesia induc-tion caused some degree of hypotension, which waswell toleratedinthispopulation.Therefore,ourresultsmaynot extendtoemergencysurgeryorelderlypatientsorpatients ASA3---4inwhichthehemodynamictolerancemaybepoor. Magnesium may cause a dose-dependent potentiation of neuromuscularblockers (NB),which wasnotmonitoredin ourstudy.SooneshouldbecautiouswhenusingMgSO4witha non-depolarizingNB,22suchasrocuronium,forshort surger-iesorinspecialsituations,whenadifficultmaskventilation orintubationisexpected.
Conclusion
Our study showed that lower magnesium sulfate doses are sufficient toattenuate the hemodynamic response to tracheal intubation, withresults similar tolidocaine. We conclude that the used doses of magnesium sulfate and lidocainehave goodefficacy and safetyfor hemodynamic control during laryngoscopyand intubation, presenting as an option to mitigate the stimulation of upper airway in patientsundergoinggeneralanesthesia.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.PuriGD,MarudhachalamKS,ChariP,etal.Theeffectof magne-siumsulphateonhemodynamicsanditsefficacyinattenuating theresponsetoendotrachealintubationinpatientswith coro-naryarterydisease.AnesthAnalg.1998;87:808---11.
2.Fawcett WJ, HaxbyEJ, MaleEA.Magnesium: physiologyand pharmacology.BrJAnaesth.1999;83:302---20.
3.Panda NB, Bharti N, Prasad S. Minimal effective dose of magnesium sulfatefor attenuationof intubation responsein hypertensivepatients.JClinAnesth.2013;25:92---7.
4.Vivancos GG, Klamt JG, Garcia LV. Efeito da utilizac¸a˜o de 2mg·kg−1delidocai´naendovenosanalateˆnciadeduasdoses diferentes de rocuroˆnio e na resposta hemodinaˆmica à intubac¸a˜o traqueal. Rev Bras Anestesiol. 2011;61: 1---12.
5.Kindler CH, Schumacher PG, Schneider MC, et al. Effects of intravenous lidocaine and/or esmolol on hemodynamic responsestolaryngoscopyandintubation:adouble-blind, con-trolledclinicaltrial.JClinAnesth.1996;8:491---6.
6.SouzaACD,AlvarezMAP,MenezesMS.Bloqueiodasalterac¸ões cardiocirculatóriasprovocadaspelalaringoscopiaeintubac¸ão traqueal:estudocomparativoentrefentanilelidocaínavenosa. RevBrasAnestesiol.1991;41:381---5.
7.NooraeiN,DehkordiME,RadpayB,etal.Effectsofintravenous magnesium sulfate and lidocaine on hemodynamic variables followingdirectlaryngoscopyandintubationinelectivesurgery patients.Tanaffos.2013;12:57---63.
8.OliveiraCMB,IssyAM,SakataRK.Lidocaínaporviavenosa intra-operatória.RevBrasAnestesiol.2010;60:325---33.
9.FinnerupNB,Biering-Sorensen F,JohannesenIL,et al. Intra-venouslidocainerelievesspinalcordinjurypain:arandomized controlledtrial.Anesthesiology.2005;102:1023---30.
10.Paesano CR, GonzálezOM,Rodríguez B, et al.Laringoscopia eintubacióntraqueal:usodesulfatodemagnesiopara aten-uar la respuesta cardiovascular refleja. Rev Ven Anestesiol. 1998;3:66---71.
11.TurlapatyPDMV,CarrierO.Influenceofmagnesiumoncalcium inducedresponsesofatrialandvascularmuscle.JPharmacol ExpTher.1973;187:86---98.
12.CaroD-Pretreatmentagentsforrapidsequenceintubationin adults.In UpToDate,WallsRM(ed), UpToDate,WalthamMA. (Accessedon04January2015).
13.Choyce A, Avidan MS, Harvey A, et al. The cardiovascular responsetoinsertionoftheintubatinglaryngealmaskairway. Anaesthesia.2002;57:330---3.
14.Kihara S, Brimacombe J, Yaguchi Y, et al. Hemody-namic responses among three tracheal intubation devices in normotensive and hypertensive patients. Anesth Analg. 2003;96:890---5.
15.TongJL,AshworthDR,SmithJE.Cardiovascularresponses fol-lowinglaryngoscopeassisted,fibreopticorotrachealintubation. Anaesthesia.2005;60:754---8.
16.XueFS,LiaoX,LiuKP,etal.Thecirculatoryresponsesto tra-chealintubationinchildren:acomparisonoftheoralandnasal routes.Anaesthesia.2007;62:220---6.
17.XueFS,ZhangGH,SunHY,etal.Bloodpressureandheartrate changesduringintubation:acomparisonofdirectlaryngoscopy andafibreopticmethod.Anaesthesia.2006;61:444---8. 18.Kerr ME, Rudy EB, Weber BB, et al. Effect of
short-duration hyperventilation during endotracheal suctioning on intracranialpressureinseverehead-injuredadults.NursRes. 1997;46:195---201.
19.RudyEB,TurnerBS,BaunM,etal.Endotrachealsuctioningin adultswithheadinjury.HeartLung.1991;20:667---74. 20.RamirezPC,RodríguezB,LenguaM,etal.Magnesioy
21.FigueredoE,Garcia-FuentesEM.Assessmentoftheefficacyof esmololonthehaemodynamicchangesinducedbylaryngoscopy and tracheal intubation: a meta-analysis. Acta Anaesthesiol Scand.2001;45:1011---22.