LETTERSTOTHEEDITOR 667 also be reviewed by the authors, effectiveness is the
termsuggested;
5. Finally,Ileaveasarecommendationtheobservationto theauthorsthattherearelargerdoses,equallysafeand equally effective, that could have been tested in this clinical trial and increased the degree of information relatedtothetopic.3
I congratulate the authors for the brilliant initiative, while celebrating at thesame timethe possibilityof cre-atingthislineofresearchinanesthesiainBrazil.Thankyou fortheopportunitytocontributetothistopic.
Conflicts
of
interest
Theauthordeclaresnoconflictsofinterest.
References
1.Mendonc¸aFT,QueirozLMGM,GuimarãesCCRG,etal.Osefeitos dalidocaínaedosulfatodemagnésionaatenuac¸ãodaresposta
hemodinâmica à intubacão orotraqueal: estudo unicêntrico, prospectivo, duplamente encoberto e aleatorizado. Rev Bras Anestesiol.2016.Emprocessodepublicac¸ão.
2.KimHY.Statisticalnotesforclinicalresearchers:two-way analy-sisofvariance(ANOVA)---exploringpossibleinteractionbetween factors.RestorDentEndod.2014;39:143---7.
3.BarbosaFT1,BarbosaLT,JucáMJ,etal.Applicationsof magne-siumsulfateinobstetricsandanesthesia.RevBrasAnestesiol. 2010;60:104---10.
FabianoTimbóBarbosa
CentroUniversitárioTiradentes,CiênciasdaSaúde,
Maceió,AL,Brazil
E-mail:[email protected]
http://dx.doi.org/10.1016/j.bjane.2017.04.009 0104-0014/
©2017PublishedbyElsevierEditoraLtda.onbehalfofSociedade BrasileiradeAnestesiologia.Thisisanopenaccessarticleunder theCCBY-NC-NDlicense(http://creativecommons.org/licenses/ by-nc-nd/4.0/).
Reply
to
the
letter
to
the
Editor
夽Resposta
à
carta
ao
Editor
DearEditor,
WethankBarbosa’s1letterinwhichheappreciatesourwork andpraisesthestudy‘‘Effectsoflidocaineandmagnesium sulfateinattenuatinghemodynamicresponsetoorotracheal intubation:asingle-center,prospective,double-blind, ran-domizedstudy’’carriedoutinourservice.2Forus,author andauthor’sguesttowritethisreplay,itisonlyfairthatwe respondwithattention toall questions,withinour limita-tions:
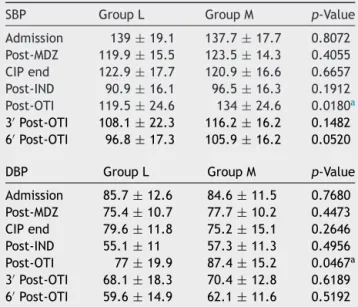
(1) Question:Theauthorsrefertoadiscretestatistical dif-ference,which does notallow the readertodrawhis ownconclusions:‘‘GroupMhadastatisticallysignificant increaseinSBP(p=0.018)andDBP(p=0.0467)post-OTI (Fig.2),butof littleclinical importance.’’The values shouldbedemonstratedintextbecause,asitisinFigure 2,itisnotpossibletocapturethemagnitudeofthem,so thatthelackofclinicalimportancedoesnotrepresent absenceofbiologicalrelevance.
DOIofreferstoarticle:
http://dx.doi.org/10.1016/j.bjane.2015.08.004
夽 Author’sreplytotheLettertotheEditor:Effectsoflidocaine
and magnesiumsulfate inattenuating hemodynamicresponseto orotrachealintubation:asingle-center,prospective,double-blind, randomizedstudy.
RegardingItem1,itwasreallyflawed,butnot inten-tional,onourparttoomitthesedata.Themissingdata
areonTable1.
(2) Question:Datawere,inpartorinwhole,analyzedover timeandpatientsalsoreceivedanesthetics,inaddition tothemedicationstested,whichmaybeadditionalor not.Itisknownthatmagnesiumsulfatehasaprolonged clinicaleffectaftervenoususe,whereaslidocainehasa
Table1 Comparisonofthemean±standarddeviationof bloodpressureinmmHgatthedifferenttimesofthestudy.
SBP GroupL GroupM p-Value
Admission 139±19.1 137.7±17.7 0.8072 Post-MDZ 119.9±15.5 123.5±14.3 0.4055 CIPend 122.9±17.7 120.9±16.6 0.6657 Post-IND 90.9±16.1 96.5±16.3 0.1912 Post-OTI 119.5±24.6 134±24.6 0.0180a
3′Post-OTI 108.1±22.3 116.2±16.2 0.1482 6′Post-OTI 96.8±17.3 105.9±16.2 0.0520
DBP GroupL GroupM p-Value
Admission 85.7±12.6 84.6±11.5 0.7680
Post-MDZ 75.4±10.7 77.7±10.2 0.4473
CIPend 79.6±11.8 75.2±15.1 0.2646
Post-IND 55.1±11 57.3±11.3 0.4956
Post-OTI 77±19.9 87.4±15.2 0.0467a
3′Post-OTI 68.1±18.3 70.4±12.8 0.6189
6′Post-OTI 59.6±14.9 62.1±11.6 0.5192
SBP, systolicbloodpressure;MDZ,midazolam;CIP,continuous infusionpump;IND,induction(ofanesthesia);OTI,orotracheal intubation;DBP,diastolicbloodpressure.
a
668 LETTERSTOTHEEDITOR shortprotectiveeffectagainstmagnesium.Thus,there
aretwofactorsthatmust beconsidered inthis statis-ticalanalysis:timeandtreatment.Thebeststatistical testtobeperformedinthissituationistwo-wayANOVA. Theresultsanalyzedastheyareinthetextmaybe erro-neouslypositive,andthepossibilityofatypeIerrorin thisstudyisclearlyperceived.
Regarding Item2, we disagree with the statement. Two-wayANOVAisapplicablewhentherearea numeri-caldependentvariableandtwocategoricalindependent variables.3,4Timeisanumericalvariable,andthisdata collectiondesignisknownasrepeatedmeasures.ANOVA with repeated measures or a non-parametric option (such as mixed effects models) is indicated in these situations,nottwo-wayANOVA.3,5Considerthe follow-ing: there is no independence between measures in relation to time (historical dependence), which vio-lates an important assumption of two-way ANOVA.3,4 And,contrarytowhathasbeenstated,repeatedlyusing hypothesis testsat each time-pair increasesthe num-beroftestsandalsotheincidenceoffalse-positive,one ofthemainreasonsforrepeatedmeasuresANOVA.5On the other hand,several factorspreventusfrom using repeated measures ANOVA in this sample because we wouldviolateassumptions,suchassphericityand nor-mality (note that timebetween measurements is not regular).Mixedeffectsmodelscouldbeapplied; how-ever, duetoitslowsensitivity,theyrequireverylarge samples,beingoflittleuseinthissample.Furthermore, consideringthatthemainobjectiveofthestudyisthe oneusedtocalculatethesamplesize,thatis,the sys-tolicblood pressuresimplevariationafterorotracheal intubation(OTI),performingrepeatedmeasures analy-sisthatwerenotpredictedwouldbecharacterizedas datamining,whichwouldbeinappropriate.
(3) Question: If the authors consider correct the use of the Student’s t-test, or more appropriately in some casestheMann---WhitneyUtest,accordingtothetext, they shouldhave corrected the p-valuewith the pro-cedureformultiplehypothesiscorrectiontest,instead ofconsideringonly5%asthelevelofsignificanceinall analysis.Thepossibilitythattheresultwaspositivein the statistical analysisand occurred at randomis 5%. Correctingthe p-valuewould decreasetheprobability of thestatistical resultrandomoccurrence.Thus,the possibilityoftypeIerrorinthisstudyisclear.
RegardingItem 3,we partially agree.Manyauthors recommend that the exact p-values should be published,6 since there is no consensus regarding the best method for correction using multiple tests, andthecriticalp-valuecorrectionbeingconsideredfor significanceratherthancorrectingthep-valueofeach hypothesis test performed as a well-recommended alternative.7Inthisstudy,usingthecorrectionmethod proposed by Bonferroni, for example, the critical
p-value would be 5%/16=0.003125%. Bonferroni’s correctionisthemostconservative,buttherearethose whodiscusswhether itappliestothesole test ofthe study main outcome or only to all other additional hypothesistests,orevenwhetheritshouldbeused.8,9 (4) Question: The authors’ objective was ‘‘to compare
the efficacy of intravenous magnesium sulfate versus
lidocaine on this reflex hemodynamics after laryn-goscopyandtrachealintubation’’.Theauthors’ conclu-sionwas‘‘magnesium sulfateandlidocainehavegood efficacy and safety for hemodynamic management in laryngoscopyand intubation’’, which does not fit the proposed objective. It is necessary that the authors relatewhichweretheefficacyvariablesandthesafety variablesso that theconclusion is betterunderstood. Itshouldbenotedthatthetermefficacyshould gener-allybeusedinstudieswhose executionconditionsare ideal, as with laboratory studies. The authors should alsoreviewthis term,asuggestion istousethe term effectiveness.
RegardingItem4,therewasreallyaproblemin draft-ingconclusions.Themostaccurateconclusionwouldbe: ourstudywasnotabletodetectastatistically signifi-cantdifferenceinpost-OTIsystolicbloodpressure(SBP) amongthegroups thatreceivedmagnesium sulfateor lidocaine.Becauseitisastudyofsuperiority(itisnot written, butaswe donotuse margin ofinferiority in calculatingthesamplesize,onlythisoptionis compat-ible),thestudymaynotconclude,besides,everything elseisdiscussion.Wereinforceforotherreadersthatif nodifferenceisfoundinastudyofsuperiority,itdoes notmeanthatthereisequalityornon-inferiority. (5) Question: Finally, I leave as a recommendation the
authors’observationthattherearelargerdoses,equally safeandequallyeffective,thatcouldhavebeentested inthisclinicaltrial andincreasedthedegreeof infor-mationrelatedtothetopic.
RegardingItem5,weappreciatethesuggestionand willconsideritinfuturestudies.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.BarbosaFT.Effectsoflidocaineandmagnesiumsulfatein attenu-atinghemodynamicresponsetoorotrachealintubation:a single-center,prospective,doubleblind,randomizedstudy.BrazJ Anes-thesiol. 2017, http://dx.doi.org/10.1016/j.bjan.2017.01.002 [Epubaheadofprint].
2.Mendonc¸a FT, de Queiroz LM, GuimarãesCCR, et al. Effects of lidocaine and magnesium sulfate in attenuating hemody-namicresponsetotracheal intubation:single-center, prospec-tive, double-blind, randomized study. Braz J Anesthesiol. 2017;67:50---6.
3.GelmanA.Analysisofvariance?Whyitismoreimportantthan ever.AnnStat.2005;33:1---53.
4.FujikoshiY.Two-wayANOVAmodelswithunbalanceddata. Dis-creteMath.1993;116:315---34.
5.MaY,MazumdarM,MemtsoudisSG.Beyondrepeated-measures analysisofvariance:advancedstatisticalmethodsforthe anal-ysisoflongitudinaldatainanesthesiaresearch.RegAnesthPain Med.2012;37:99---105.
6.RothmanKJ.Noadjustmentsareneeded formultiple compar-isons.EpidemiolCambMass.1990;1:43---6.
7.Narum SR. Beyond Bonferroni: less conservative analyses for conservationgenetics.ConservGenet.2006;7:783---7.
LETTERSTOTHEEDITOR 669
9.Armstrong RA. When to use the Bonferroni correction. Oph-thalmic Physiol Opt J Br Coll Ophthalmic Opt Optom. 2014;34:502---8.
FabricioTavaresMendonc¸aa,∗,
GabrielMagalhãesNunesGuimarãesb
aHospitaldeBasedoDistritoFederal,Unidadede
AnestesiologiaeMedicinaPerioperatória,Brasília,DF,
Brazil
bHospitalUniversitáriodeBrasília,Brasília,DF,Brazil
∗Correspondingauthor.
E-mail:[email protected](F.T.Mendonc¸a).
http://dx.doi.org/10.1016/j.bjane.2017.08.003 0104-0014/